
Abstract
Background:
Direct laryngoscopy is often poorly tolerated in patients with foreign body ingestion. The use of flexible endoscopes, which are reported to be better tolerated, was described. However, studies on endoscopy usage by emergency physicians are lacking.
Objective:
This study evaluates whether using a bronchoscope is as effective as the direct laryngoscopy for localising pharyngeal foreign bodies by emergency physicians.
Methods:
This was a randomised cross-over manikin study conducted on 32 emergency physicians. Four foreign bodies were placed at the oropharynx, vallecula, arytenoid and post-cricoid area of a manikin. Participants, being randomised into two groups, examined the pharynx with a bronchoscope and a direct laryngoscope in designated orders. The primary outcome was the complete visualisation rate defined as visualising all the four foreign bodies within the time limit. Secondary outcomes included participants-rated difficulty scores, device preferences, the time needed for complete visualisation and cumulative success rates.
Results:
Complete visualisation rate was significantly higher using the bronchoscope (93.8%) than the direct laryngoscope (62.5%) p = 0.02. The overall difficulty score was lower using the bronchoscope (median 4, interquartile range: 3–5) than the direct laryngoscope (median 6, interquartile range: 5–8), p < 0.001. The bronchoscope was the preferred method for overall examination (71.9%) over the direct laryngoscope (28.1%), p = 0.001. There were no significant differences in times needed for complete examination for the bronchoscope (median 73.6 s, interquartile range: 54.7–97.7 s) and the direct laryngoscope (median 82.2 s, interquartile range: 40.1–120 s), p = 0.9, and cumulative success rates, p = 0.081.
Conclusion:
The bronchoscope was associated with an increased complete visualisation rate and was the easier and preferred method for pharyngeal examination.
Introduction
Direct laryngoscopy is commonly performed for foreign body ingestion in local emergency departments, with fish bones commonly involved in Asian Chinese. 1 Identified foreign bodies are removed with a pair of laryngeal forceps. Referral for oesophagogastroduodenoscopy, performed by surgeons or gastroenterologists, may be warranted if no foreign body is found in the pharynx. 2
However, complete pharyngeal examination with direct laryngoscopy is often difficult, poorly tolerated, and carries risks. It causes trauma to the tongue, teeth, oropharynx, and larynx. 3 Nontraumatic complications including aspiration, 4 sympathetic surge, 5 and vasovagal responses 6 may also result. On the contrary, flexible laryngoscopy is widely performed by otorhinolaryngologists for a wide range of office-based laryngeal procedures. It is safe and well tolerated.7–10 Local emergency trainees have scarce opportunities for endoscopy training. For instance, flexible fiberoptic intubation only accounted for 1.1% in a series of 17,910 intubations in emergency departments; 11 and studies on endoscope usage by emergency physicians are relatively lacking. This study compared endoscopic examination with a bronchoscope (BR), available in most emergency departments as an airway adjunct, to a direct laryngoscope (DL) for localising pharyngeal foreign bodies by emergency physicians who are less trained for endoscopy. A manikin was used as it permitted repeatable examinations with different devices by our participants.
Methods
It was a randomised cross-over manikin study conducted in Tseung Kwan O Hospital Accident and Emergency department, Hong Kong SAR.
Participants
All working emergency physicians were recruited.
Equipment
An airway model, Laerdal® Airway Management Trainer, was used. Four blue-coloured foreign bodies of 4-millimetre diameter were placed at the oropharynx, vallecula, arytenoid, and post-cricoid area in advance (Figure 1), corresponding to the commonest sites of impaction reported in local literature.12,13 No foreign bodies were placed inside the oral cavity, as they could be identified without laryngoscopy; and no foreign bodies were placed at or below the cricopharyngeus, as their identification likely requires oesophageal examination by experienced endoscopists. An Airway Anatomy Demonstration Model provided in the same training set was used for technique demonstration.
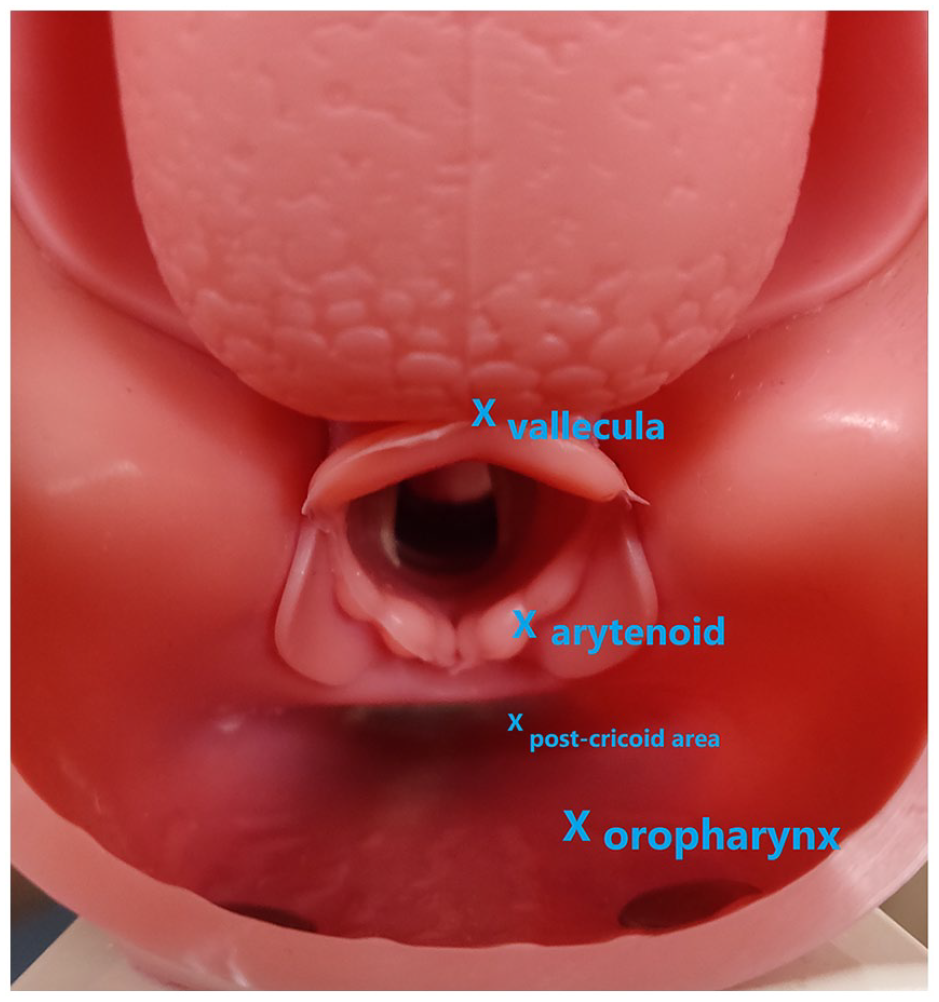
The four positions of foreign bodies inside the pharynx: oropharynx, vallecula, arytenoid, and post-cricoid area (marked with X).
The DL used was manufactured by Welch Allyn, which is composed of an E-MacIntosh blade #3 and a standard handle. The BR, the Airway Mobilescope MAF-TM manufactured by Olympus, was a portable, flexible one with a 5.2 mm outer diameter, 2.6 mm suction channel, and a 600 mm working length. Its outer diameter was comparable to the flexible laryngoscopes used by otorhinolaryngologists (Figure 2).

Laerdal® airway management trainer and the Airway Anatomy Demonstration Model (left), Macintosh laryngoscope with E-Mac blade #3 (middle), Airway Mobilescope (right).
Study protocol
Participants were randomised into two groups, Group A (DL-BR) and Group B (BR-DL), in a 1:1 ratio with the randomisation sequence generated by ‘www.randomisation.com’, stratified by their emergency specialist qualification. In group A (DL-BR), the examination was first performed with DL, and then with BR; in group B, the examination was first performed using BR, and then DL.
Techniques of using both DL and BR were demonstrated on the Airway Anatomy Demonstration Model before the study. Ten minutes were given to participants for hands-on experience until they were ready to use both devices. They were then instructed to localise all pre-placed foreign bodies within 2 minutes, using the respective device without knowing the exact number or locations of the foreign bodies. The study began once the device was inserted; and ended either when all the foreign bodies were localised, or the 2 minute time limit passed. The positions of the foreign bodies were reviewed to the participants at the end of the study.
Data collection
Objective assessments included success rates and timings for localising the foreign bodies. Subjective assessments included participants’ rated difficulty scores (on a numeric rating scale 0–10, 10 being the most difficult) and device preferences. The primary outcome was the complete visualisation rate (expressed in %), with complete visualisation defined as localising all the foreign bodies within the 2 minutes. Secondary outcomes included participants’ self-rated difficulty scores (0–10) and device preferences (%). Subgroup analyses were done for foreign bodies at the four specific sites respectively. The time needed for complete visualisation (s) and cumulative success rates were also evaluated.
Data analysis
Data were analysed with SPSS 26.0. The chi-square test and the Mann–Whitney U test were used for categorical data and non-parametric data respectively. The cumulative success rates were analysed with Kaplan-Meier analysis and log-rank test. Alpha was set at 0.05 (two-sided), and beta was set at 0.2, and power 80%. Data are presented as median, interquartile range (IQR), or percentages (%).
Results
Recruitment
The minimum sample size was estimated to be 48, using data from an unpublished pilot of 8 participants, with complete visualisation rates of 93.8% using BR and 62.5% using DL. Thirty-two emergency physicians were recruited (Figure 3), giving 64 examination attempts after crossover. All recruited participants completed the study, and there was no loss of data. Their demographics are summarised in Table 1.
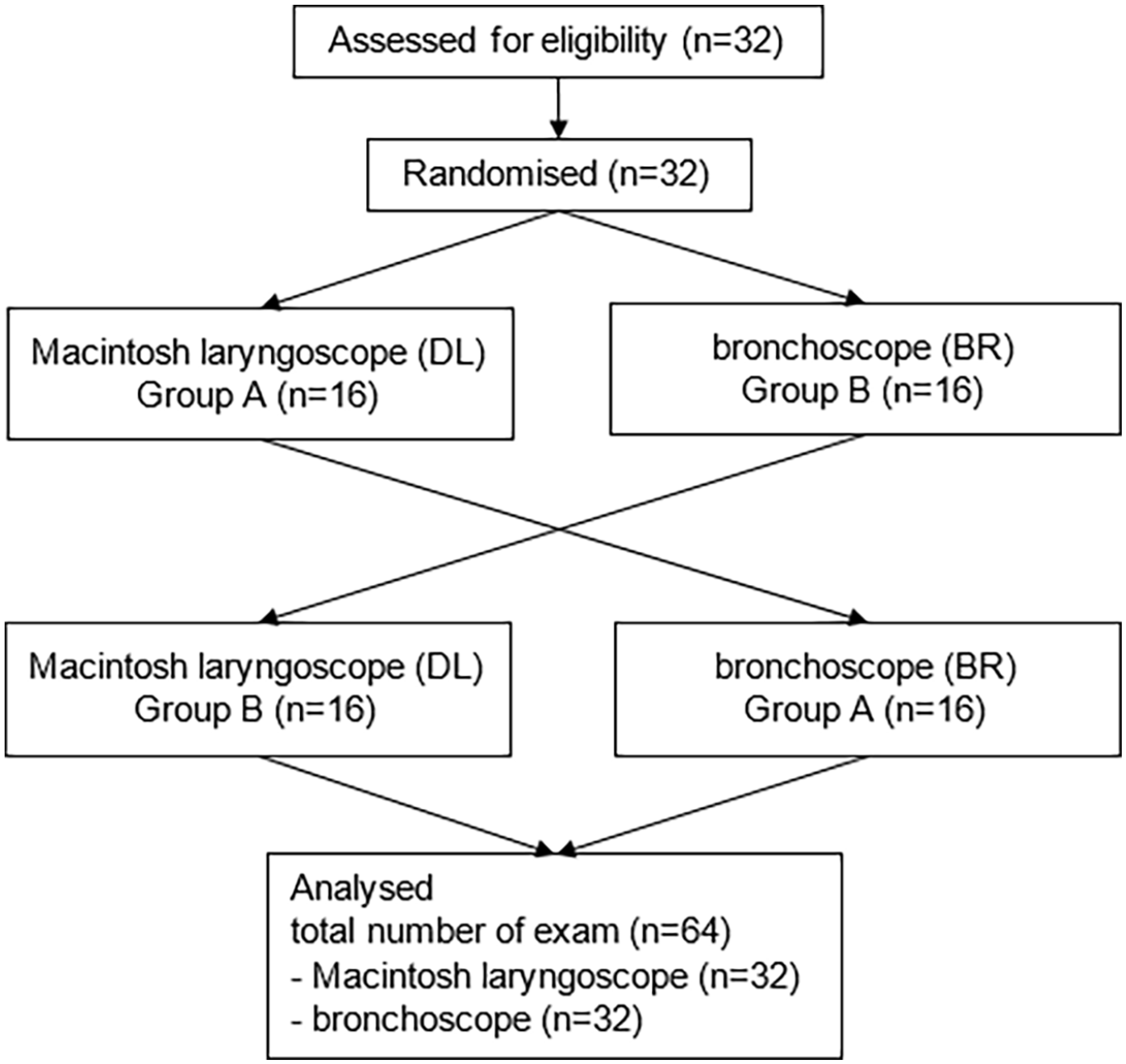
Flow diaphragm concerning the recruited emergency physicians.
Demographics of recruited participants.
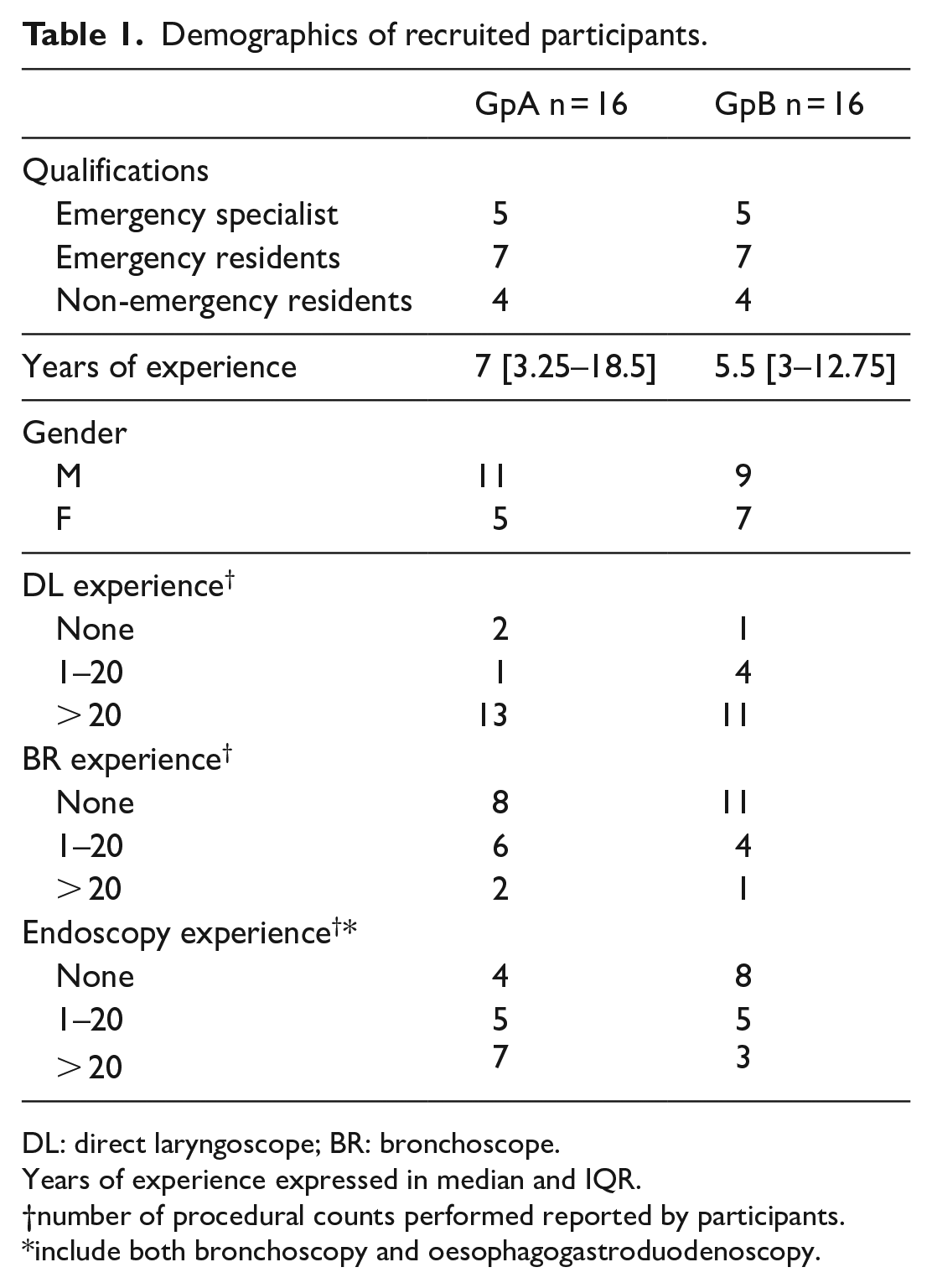
DL: direct laryngoscope; BR: bronchoscope.
Years of experience expressed in median and IQR.
number of procedural counts performed reported by participants.
include both bronchoscopy and oesophagogastroduodenoscopy.
Complete visualisation rate
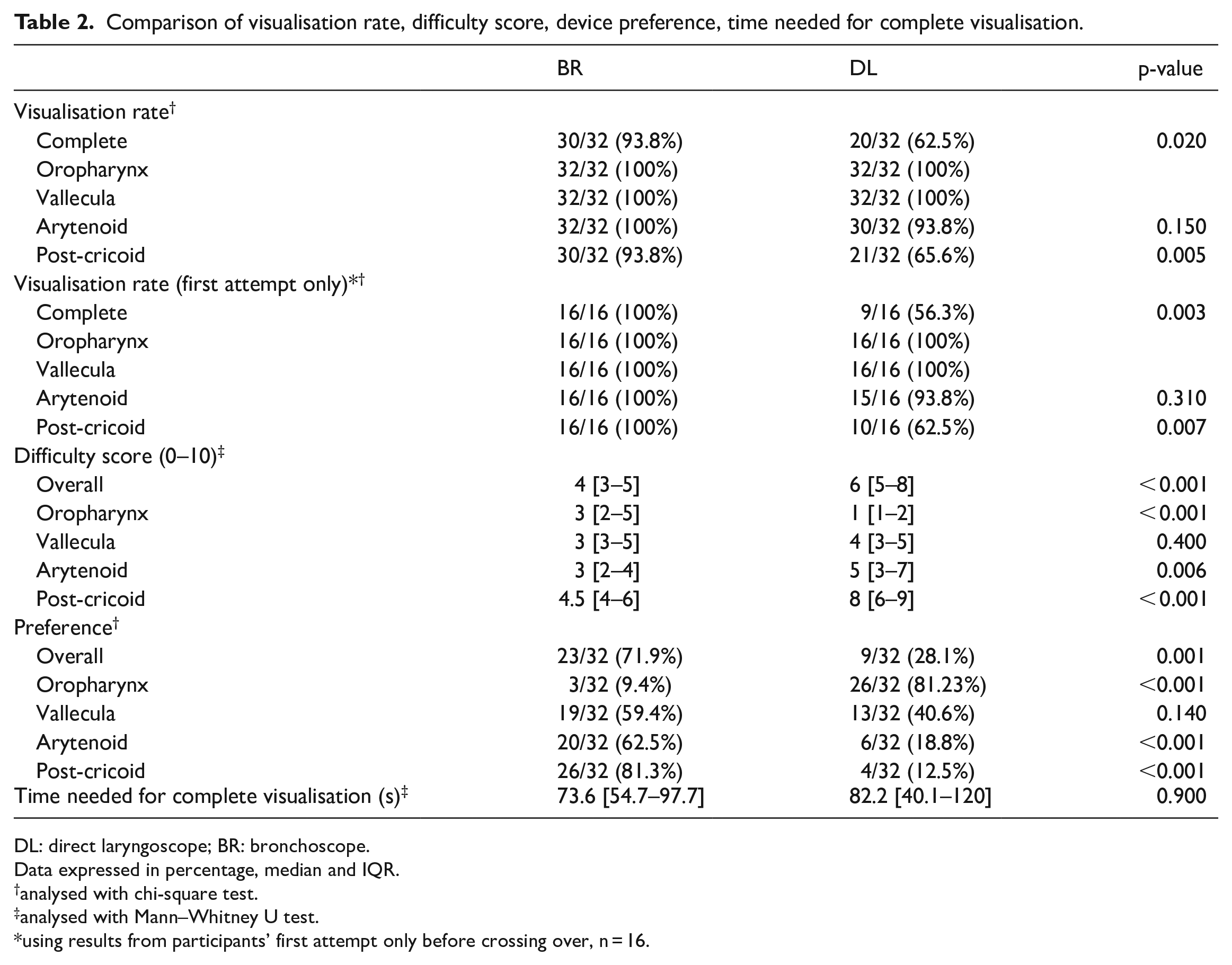
At 2 minutes, the complete visualisation rate was significantly higher for BR than DL (p = 0.02). The post-cricoid area was the most commonly missed site in both groups. The comparison was repeated using data before the cross-over to eliminate any carry-over effects, and the difference was still significant (p = 0.003). Results are summarised in Table 2.
Comparison of visualisation rate, difficulty score, device preference, time needed for complete visualisation.
DL: direct laryngoscope; BR: bronchoscope.
Data expressed in percentage, median and IQR.
analysed with chi-square test.
analysed with Mann–Whitney U test.
using results from participants’ first attempt only before crossing over, n = 16.
Difficulty scores, and device preferences
For overall assessment, BR had a lower difficulty score than DL (p < 0.001). BR also had lower difficulty scores for localising foreign bodies at the arytenoid (p = 0.006) and the post-cricoid area (p < 0.001) (Table 2, Figure 4). For preferences, BR was the preferred method for overall examination (p < 0.001) and examining foreign bodies at the arytenoid (p < 0.001) and the post-cricoid area (p < 0.001).
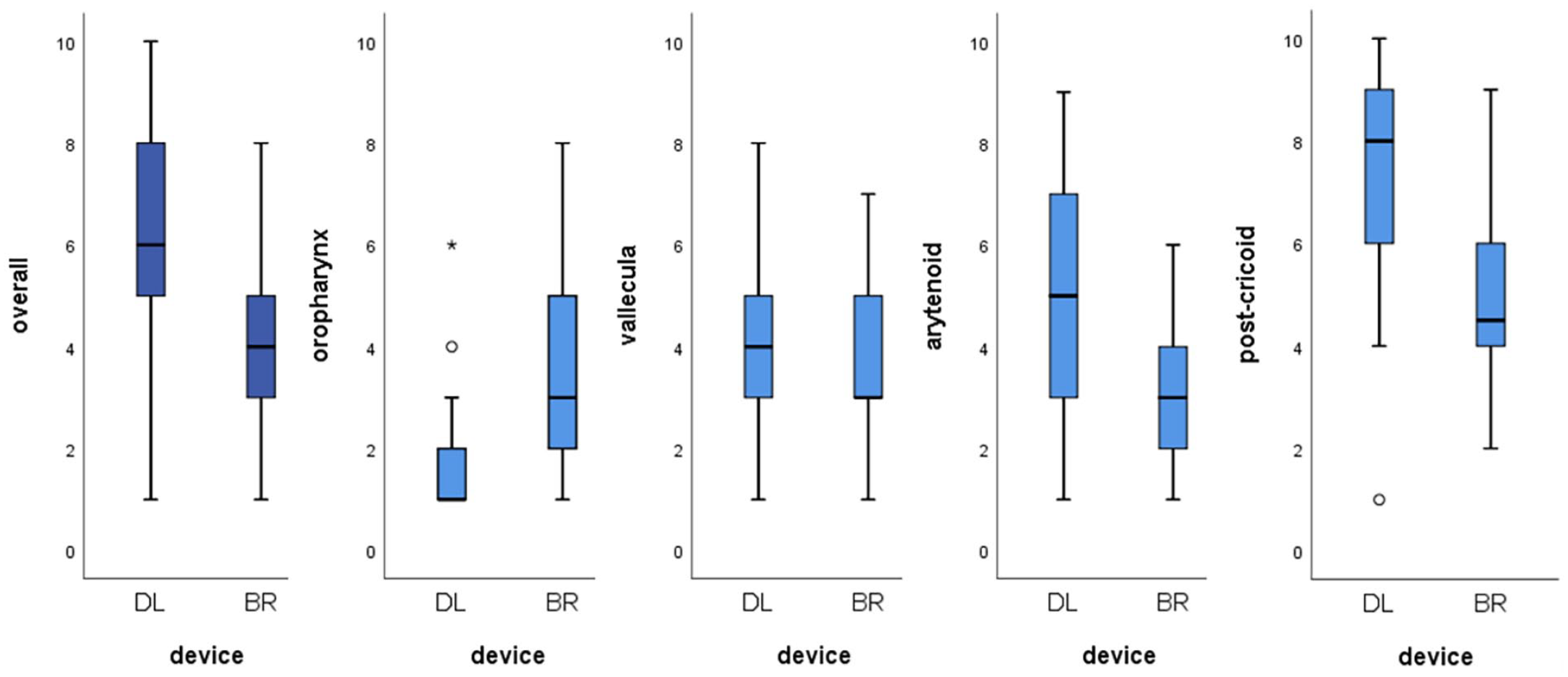
Boxplots summarising participants’ rated difficulty scores for overall examination, and examining foreign bodies at oropharynx, vallecula, arytenoid, and post-cricoid area.
Time needed for complete visualisation
The difference in times needed for complete visualisation between the devices was insignificant (p = 0.903) (table 2).
Cumulative success rate of success
The cumulative rates for completing the study were summarised (Figure 5). The difference, analysed with the log-rank test, was insignificant (p = 0.081).
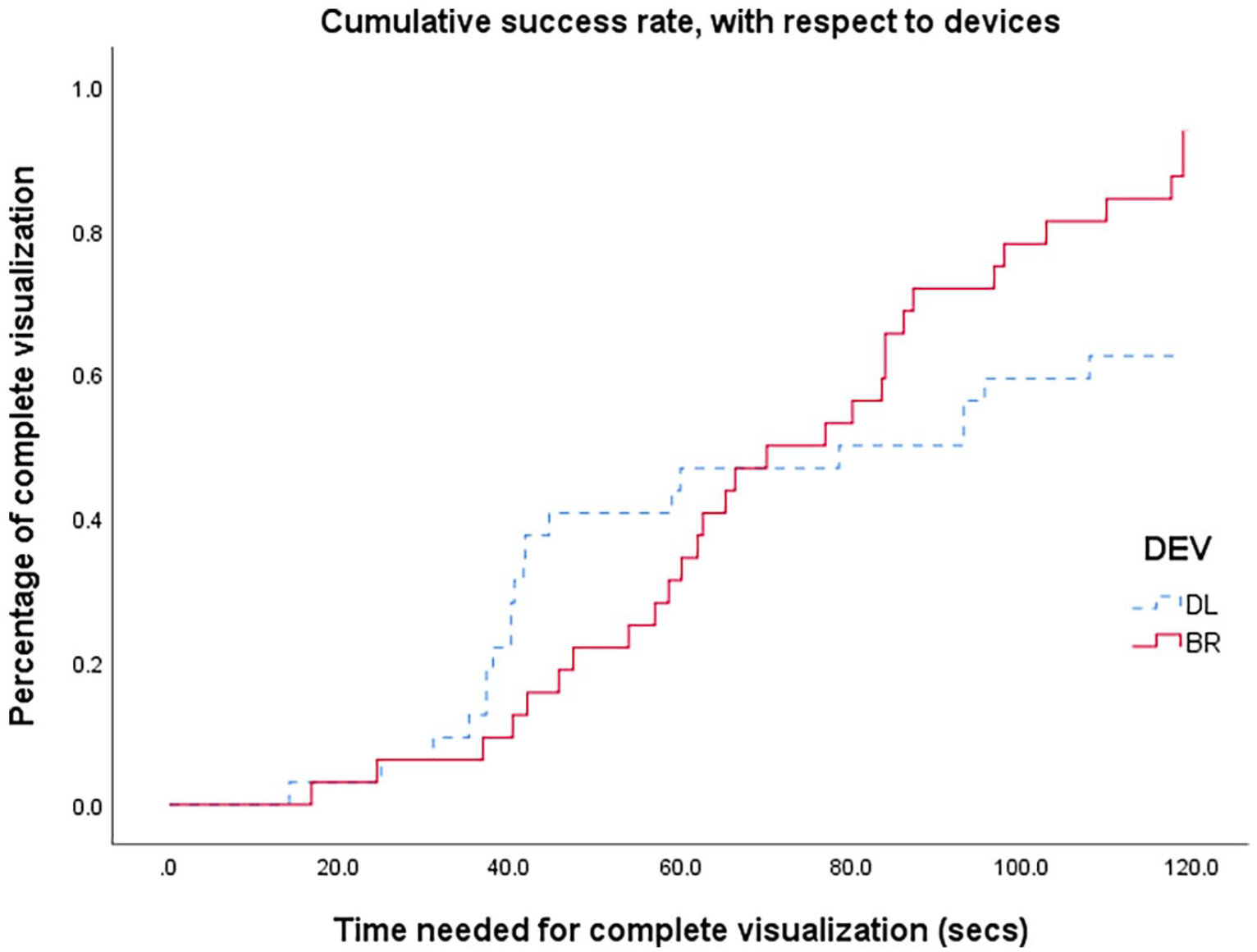
Cumulative rates of complete visualisation using DL and BR. Difference analysed with log-rank test, p = 0.081.
Discussion
Our results showed BR was associated with a higher complete visualisation rate and was the easier and preferred pharyngeal examination method by our emergency participants. It is possibly because of the wider angle of view obtained by the endoscope’s camera after entering the glottis in which all four foreign bodies could be visualised simultaneously. Operating a BR is relatively simple–involving passing the scope into the larynx transnasally. Difficulties were occasionally encountered for manipulating the endoscope through the nasopharynx; nevertheless, most participants managed to enter the larynx within a reasonable time limit. The oropharyngeal foreign body was were sometimes overlooked initially if the scope was being pushed directly into the hypopharynx on entering the glottis. On the other hand, examination using DL involves a more ‘stepwise’ approach, including patient positioning to align the axes, blade placement and advancement, visualising the larynx through a narrow-angle, and continuous ‘airway manoeuvres’ to optimise views. 14 A satisfactory glottic view may not be possible despite the maximal effort. In this study with the identical manikin, the glottic views obtained by DL varied among participants with different experiences, accounting for their variable visualisation rates.
Despite no direct comparison on the ease the of use for BR and DL from literature, previous studies investigating their learning curves revealed that a mean of 6 attempts was required to perform a competent flexible laryngoscopy among a group of untrained medical students; 15 while it took up to a median of 22–47 attempts for satisfactory direct laryngoscopic tracheal intubation among groups of nurse assistant trainees and non-anaesthesia trainees respectively.16,17 This indirect evidence suggests BR may be the easier-to-learn, and the more friendly option for pharyngeal examination, especially for inexperienced emergency trainees. This may also explain our results of consistently higher complete visualisation rates using BR when compared to DL, even for junior trainees.
There were a few limitations of this study. First, a manikin was used. While it might be ideal for training, examinations are being performed on awake patients in real life, who might have a difficult airway anatomy and strong gag reflexes. On the other hand, unrecognised nasal pathologies, for example, polyps and deviated nasal septum, may pose risks of complications for BR, including nasal trauma and epistaxis. 7 Second, large size colour tagged foreign bodies were used for easy identification. However, in real life, the impacted foreign bodies, most likely fish bones, could be much smaller and of indistinguishable colour with the mucosa. While successful extractions of tiny fish bones have been reported using high-resolution flexible laryngoscopes,10,18 visualisation of such could be challenging and very much depending on the resolution of BR available locally. Last but not least, this study did not compare any foreign body extraction methods, as operating endoscopic grasping forceps requires expertise and additional personnel, which is beyond the aim of this pilot study.
While BR may not fully replace DL, the implication is that it helps identify deep-seated foreign bodies which are deemed less approachable by conventional DL. Successful localisation of foreign body aids decision making – for example, whether to attempt a targeted DL removal for the foreign body with favourable location or straight oesophagogastroduodenoscopy referral without any DL attempts if the foreign body’s location is unfavourable or suspected to be in the oesophagus. It is of particular importance if DL is anticipated to be difficult, or the foreign body is expected to be deeply located based on the patient’s symptom location. 19 Further studies can be pursued for the feasibility of endoscopic forceps removal of foreign bodies in emergency departments when emergency physicians are more well equipped.
Currently, BR in emergency departments is primarily reserved for airway emergencies, like airway obstruction, or laryngeal trauma. These situations are uncommon and unfavourable for training. Extending its indication of use in foreign body ingestion provides more opportunities for trainees to equip themselves for these emergency procedures.
Conclusion
In this pilot manikin study, endoscopic examination with the bronchoscope was associated with a higher complete visualisation rate and was the easier and preferred method for pharyngeal examination and localising deep-seated foreign bodies at the arytenoid and the post-cricoid area, when compared to the direct laryngoscopy. It may serve as an adjunct examination to aid clinical decision making. And further studies may be pursued for the feasibility of endoscopic forceps removal of foreign bodies by emergency physicians.
Footnotes
Acknowledgements
All authors are acknowledged for their contributions to the article.
Author contributions
All authors are responsible for the conception and design of the study. C.K.S. is responsible for data collection and analysis. The manuscript was written and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The individual data were anonymised. The master dataset was kept by the investigators in computer and was password protected. Access to the data would be limited to the investigators and Research Ethics Committee of Kowloon Central and Kowloon East, Hong Kong Hospital Authority. Please contact the corresponding author for further information of data if required.
Ethical approval
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. This study was approved by the Research Ethics Committee of Kowloon Central and East Cluster, Hong Kong Hospital Authority [reference: KC/KE-21-0044/ER-3, 19 April 2021].
Informed consent
Written consent was obtained from the participants for their anonymized information to be published in this article.
Human rights
There were no human rights conflicts to declare.