
Abstract
Introduction
Accidental swallowing of foreign bodies (FBs) is common in emergency department (ED). However, if the objects are sharp, the complication rate is higher. 1 Toothpick can cause severe complications of gastrointestinal (GI) tract due to being long, sharp ends on both sides, slender, and resistant to digestion. 2
Toothpick ingestion without patient’s awareness is rare but could be fatal, 3 especially if the physicians failed to think of this differential diagnosis.
We present a case of colonic perforation due to toothpick ingestion.
Case report
A 64-year-old man presented to the ED with fever and right upper abdominal pain for 3 days. He had nausea with abdominal pain, but there was no vomiting or diarrhea. He did not have any previous surgical interventions and denied any previous traumas. His vital sign showed a blood pressure of 130/80 mm Hg, pulse rate of 80 beats per minute, respiratory rate of 20 breaths per minute, and body temperature of 38.7°C. The physical examination revealed severe pain with rebound tenderness in the right upper abdominal quadrant and positive Murphy’s sign. The electrocardiography (ECG) showed normal sinus rhythm. Laboratory findings showed leukocytosis (white blood cells, 15,300/mm3) and an elevated C-reactive protein level (102.9 mg/L). Other laboratory tests (such as lactate and pro-calcitonin) were normal.
A plain abdominal radiograph showed mild ileus without pneumoperitoneum. The provisional diagnosis of acute cholecystitis was made. The abdominal sonography revealed normal finding. To differentiate other hepatobiliary diseases, we obtained a computed tomography (CT) scan of the abdomen.
The contrast abdominal-pelvic CT scan revealed linear-shaped lesion penetrating hepatic flexure of colon and proximal transverse colon (Figure 1). It showed the possibility of FB with focal edematous wall thickening or acute colitis at hepatic flexure of colon and proximal transverse colon.
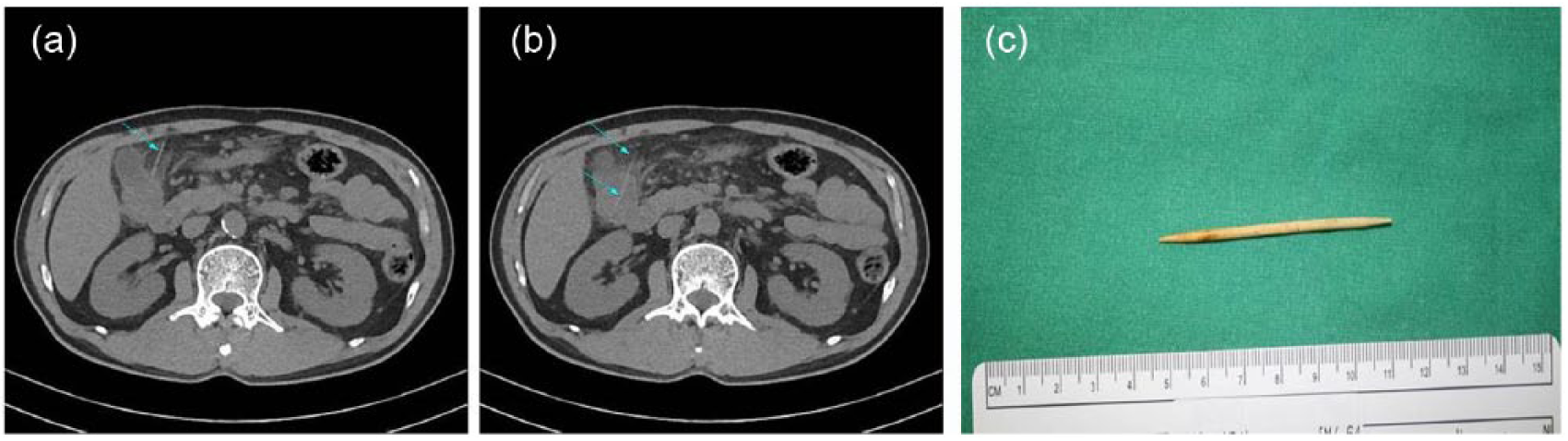
(a) and (b) Abdominopelvic computed tomography revealed linear shaped lesion penetrating hepatic flexure of colon and proximal transverse colon (arrow). (c) Photography. About 6-cm-sized toothpick was removed.
Two hours after ED admission, his vital sign showed a blood pressure of 85/60 mm Hg and pulse rate of 117 beats per minute, so the patient underwent emergent explorative laparotomy. Intestinal perforation with localized peritonitis around the proximal transverse colon was found. Colonic perforation was caused by a 6 cm of wooden toothpick (Figure 1). The toothpick was removed and the patient underwent a segmental resection of the colon with primary anastomosis.
The patient’s postoperative course was uneventful, and he was discharged without any complaint on the post-operation day 7.
In retrospect, the patient ate meat and vegetable rolls with alcohol beverage as main course for dinner 4 days before admission. But the patient did not recall swallowing of any toothpick.
Discussion
Accidental FBs ingestion is common in clinical practice, especially in emergence department. 4 Most of ingested FBs pass through the GI tract uneventfully within 1 week and perforation is rare (<1%). However, if the objects are sharp, the complication rate is higher. The perforation of GI tract can occur higher rate if ingested FBs are sharp, pointed ends, long body such as fish bones, chicken bones, needles, toothpicks. 1 Toothpick can cause severe complications of GI tract due to being long, sharp ends on both sides, slender, and resistant to digestion (toothpick was made of wood in this case). Toothpicks account for about 9% of ingested FBs. 2
Male gender, habitual chewing toothpicks, meals containing toothpick, and alcohol drinks were major risk factors of toothpick ingestion. 5
Toothpick-related injury occurs in the duodenum (25%); sigmoid (14%); ileum (9%); jejunum (7%); cecum (7%); and ascending, descending, and transverse colons (7%). There were seven cases in which toothpicks migrated outside the GI tract: pleura, pericardium, peritoneum, ureter, or bladder. 6 Ingestion of FBs can cause GI complications: bleeding, obstruction, perforation, abscess, and sepsis. Even toothpick ingestion caused death. 3 Li and Ender 6 reported that the mortality rate was 18% of toothpick ingestion.
Diagnosis of toothpick ingestion is very difficult. Definitive diagnosis of toothpick ingestion was most commonly made by laparotomy (53%), endoscopy (19%), imaging study (14%), and autopsy (12%). Patients rarely recall the event of toothpick ingestion. Actually, 12% of patients could recall history of toothpick swallowing.1,6 Our patient did not know that he swallowed the toothpick.
There is limitation to use plain radiography for diagnosis of nonmetallic FBs. Because most toothpicks are made of wood or starch, they are radiolucent on plain radiography. Even radiopaque objects are indistinguishable due to large soft tissue masses or fluid. Sonography and CT scan are preferred techniques when there is clinical suspicion of severe and rare diagnosis. 1 Our patient had pain and tenderness on right upper quadrant; therefore, physicians had impressions about hepatobiliary problems. We conducted CT scan with pre- and post-contrast images. There was linear-shaped hyperdense lesion penetrating hepatic flexure of colon and proximal transverse colon in pre-contrast images of CT scan that was suspicious of a FB. And there was layered wall thickening and peri-colic infiltration in contrast images of CT scan. 3 For avoiding radiation hazards, we did not fulfill pre- and post-contrast CT scan in childhood. There are five cases of toothpick ingestion in childhood. Although the number of cases is small, pre- and post-contrast CT scan should be performed if toothpick ingestion is suspected.
In many complicated cases such as perforation, intractable bleeding, abscess, or fistula, surgery is the treatment of choice. There was an uneventful recovery followed by the endoscopic removal of the FBs. Endoscopic removal and laparoscopic exploration have been reported as new modalities in the management of ingested FBs.2,7,8
Conclusion
Toothpick ingestion without awareness is rare but fatal. FB ingestion is frequently not suspected by physician. It is important to keep in mind that ingested FBs in the differential diagnosis of acute abdomen, and timely pre- and post-contrast CT scan should then be performed.
Footnotes
Acknowledgements
All authors have made substantive contributions to the study, and all authors endorse the data and conclusions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We confirm that guidelines on patient consent have been met and any details of informed consent obtained.