
Abstract
Ligamentum arteriosum calcification is the calcification or ossification of arterial ligaments. However, on computed tomography images, ligamentum arteriosum calcification is often mistaken for esophageal perforation when a patient has a medical history of foreign body ingestion. Ligamentum arteriosum calcification is uncommon in clinical practice. In this case report, we confirm the presence of this condition intraoperatively, which has seldom been reported previously. Increased awareness of the clinical characteristics of this uncommon disease can help thoracic surgeons with proper patient management.
Keywords
Introduction
Ligamentum arteriosum calcification (LAC), which is encountered uncommonly in clinical practice, is a pathological abnormality for which no treatment is needed. 1 Thus, the diagnostic rate is low. On computed tomography (CT), LAC appears to be similar to an esophageal perforation that was induced by foreign body (FB) ingestion. It can therefore be difficult to differentiate between the two conditions. Here, we report an uncommon case of LAC and present a relevant literature review.
Case report
A 15-year-old boy ingested a duck bone 2 days before presentation. Since ingestion, he had been coughing severely and belching intermittently. He aspirated a few rice grains at night, coughed severely, and developed chest pain. He visited a local hospital that night and was diagnosed with esophageal perforation induced by foreign body (FB) ingestion. Physicians recommended surgical treatment, but his parents refused. He was then fasted and received total parenteral nutrition combined with antibiotic therapy, but his symptoms were not relieved.
Twelve hours later, he was transferred to the thoracic department at our hospital for aggravated chest pain and dysphagia. Physical examination findings indicated a body temperature of 37.4°C and no abnormalities other than low-sound bilateral thoracic auscultation. Blood cell count analysis revealed a white blood cell count of 13.23 × 109/L and 80.5% neutrophils. Contrast-enhanced CT (Figures 1a, 1b, 1c) images indicated that the FB was located below the aortic arch and near the descending aorta. The average CT value was approximately 224 HU. Therefore, we made the same diagnosis. Gastroscopy and esophagoscopy were not chosen because esophageal perforation is a contraindication for endoscopy. The patient’s condition was critical, and thus, we performed an emergency left thoracotomy to avoid worsening his condition. However, intraoperatively, we found no considerable damage to the esophagus wall, no purulent secretions, and no FB in the mediastinum. Instead, we found calcification of the inferior wall of the arterial duct ligament that was approximately 0.8 cm long. Intraoperative gastroscopy revealed smooth esophageal mucosa and no erosions or ulcers. The esophageal barium radiography, which was performed on postoperative day 3 (Figure 2), showed no signs of esophageal perforation. We eventually made the diagnosis of LAC. Ten days later, the patient was discharged. The patient and his parents provided consent to publish this case.
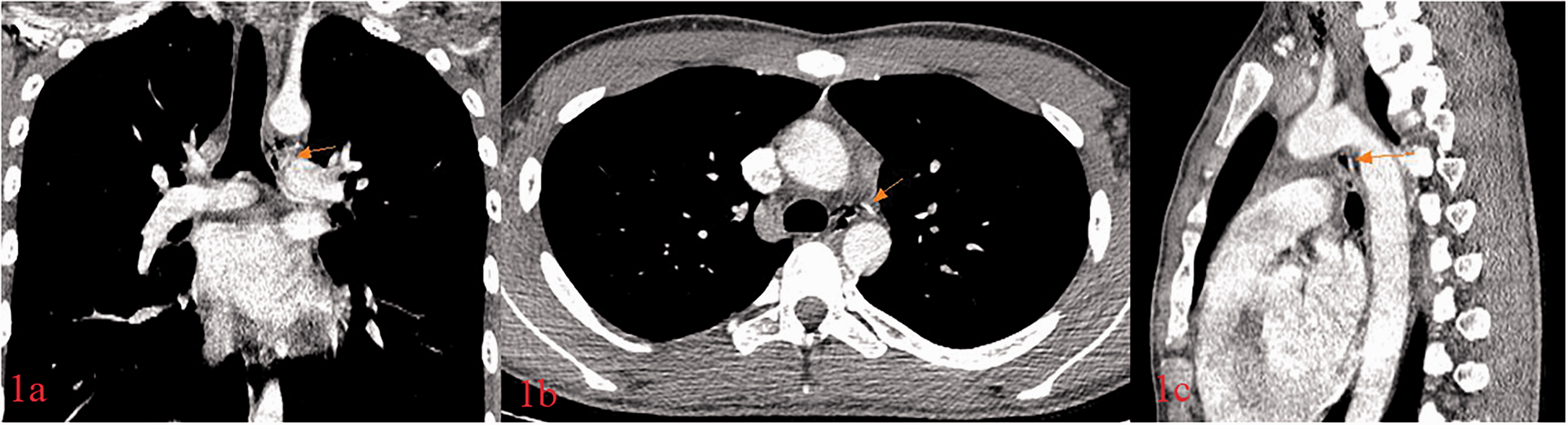
Computed tomography images of an FB in the mediastinum: (a) coronal plane, (b) cross-sectional, and (c) sagittal plane and gases that exist in the mediastinum.

The esophageal barium radiography showed that the esophageal wall was smooth, soft, and well-expanded. The mucosa was regular and there was no leakage of contrast agent.
Discussion
LAC is relatively rare and it was first proposed by Durst-Zivkovic in 1972. 2 The occurrence of LAC is related to mucinous degeneration of the arterial ligament wall. It is often incidentally found on chest CT or autopsy. Hong et al. 3 proposed the following imaging diagnostic criteria: high-density structures (mean CT measurements greater than 100 HU) in the axial and coronal planes after reconstruction or in a typical position in either plane (i.e., around the main pulmonary artery window). LAC is a pathological condition, 1 but it requires no special treatment. In this case, contrast-enhanced CT findings indicated that the FB was located below the aortic arch and near the descending aorta, which is around the main pulmonary artery window, with an average CT value of 224 HU. This result supported the diagnosis of LAC. In addition, intraoperative exploration revealed the presence of a calcified arterial duct ligament and excluded the possibility of esophageal perforation. Thus, we diagnosed the patient with LAC. A literature review showed that nearly all reported cases of LAC were diagnosed using imaging or biopsy results. However, reports on the intraoperative discovery of LAC were uncommon.
Esophageal perforation caused by an FB is relatively uncommon, and delayed treatment is an independent risk factor for high mortality and complication rates (10% to 40%). 4 , 5 Thoracic esophageal perforation induced by an FB primarily manifests as back and thoracic pain. Other nonspecific symptoms include fever, dyspnea, vomiting, mediastinal gas, and dysphagia. 6 Most of these symptoms were found in this case. CT examinations are more sensitive for identifying small-scale perforations. Imaging may detect mediastinal gas, pneumothorax, pleural effusion, and FB density. Esophageal extraluminal gas is the most common sign of esophageal perforation. 7 On the patient’s chest CT, we identified a high-density bar and mediastinal gas. Combined with the patient’s medical history and symptoms, an initial diagnosis of esophageal perforation induced by an FB was made.
Patients with esophageal perforation can rapidly progress to severe mediastinitis and multiple organ failure. Once diagnosed, surgery within 24 hours is considered to be the gold standard to remove the FB directly and to restore esophageal function. 6 , 8 Survival rates increase with early diagnosis and treatment. When surgical intervention is provided beyond 24 hours, the prognosis is worse, with a mortality rate of up to 19%. 9 In the current case, the medical history of esophageal perforation exceeded 24 hours, and the chest CT findings suggested that the FB was located near the aortic arch and descending aorta. Delayed surgery may worsen the prognosis. Because the boy’s condition permitted the intervention, we chose to perform thoracotomy. However, no FB was found intraoperatively; only the LAC was evident. No leakage of the contrast agent was found on postoperative day 3.
The reasons for making the initial diagnosis are described below. First, management of an esophageal perforation that was induced by an FB requires standardization. In this case, we did not choose preoperative gastroscopy to confirm the diagnosis, and taking the risk of piercing the thoracic aorta was not necessary. It is possible that the duck bone completely broke inside the mediastinum and that contraction of the esophageal muscularis obscured the rupture. However, in this case, gastroscopy may not identify the hole, but instead provide the opportunity to avoid surgery. Second, we lacked sufficient understanding of LAC, which is a clinically uncommon disease that is usually identified on chest CT or autopsy. The imaging diagnostic criteria proposed by Hong et al. 3 may help in such situations. Additionally, Hong et al. 3 suggested that unenhanced CT is more sensitive compared with enhanced CT for detecting LAC (37.8% vs. 16.4%), and the sensitivity for identifying LAC on the CT angiography might be adversely affected by adjacent enhancing cardiovascular structures. Thus, CT angiography may not be sensitive to detect LAC and might not be helpful to differentiate between LAC and FB. Third, there is insufficient understanding of the progress of esophageal perforation induced by an FB. The patient’s condition can rapidly progress to severe mediastinitis and multiple organ failure in cases where esophageal perforation has occurred more than 24 hours previously. The case presentation was inconsistent with late-stage esophageal perforation, and the patient’s symptoms did not worsen, but instead, they were slightly relieved. Conservative treatment may delay disease progression, and thus, we should pay more attention to the CT findings. Moreover, it was difficult to distinguish between the duck bone and LAC on the CT image that was taken in a similar position. The high-density bar and mediastinal emphysema also misled our diagnosis. We could not exclude the diagnosis of spontaneous pneumomediastinum because gas was noted in the mediastinum.
In conclusion, LAC is an uncommon disease that is difficult to distinguish from esophageal perforation caused by an FB, especially when a patient has a medical history of ingesting duck bones. When we encounter similar cases, we should pay more attention to disease progression and CT presentation. However, when the patient’s medical history exceeds 24 hours, but the symptoms are alleviated and no serious infection develops, we should doubt the presence of esophageal perforation during diagnosis and consider a diagnosis of LAC. Gastroscopy in the operating room should be performed to confirm the diagnosis, if possible. However, increasing our understanding of LAC can aid in making a differential diagnosis and avoid trauma caused by thoracotomy.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Patient’s consent
We have obtained the consent of the patient and his parents to publish this case.