
Abstract
Background:
Personal protective equipment used for protection of healthcare workers in the combat against Severe Acute Respiratory Syndrome Coronavirus 2 pandemic is in limited supply worldwide at present – 2020. Use of barrier enclosure during endotracheal intubation can potentially act as a cost-effective adjunct to minimize risks of transmitting the infection to healthcare workers. However, there is concern that the enclosure itself will act as a barrier to the intubation procedure in the emergency settings.
Objective:
To evaluate the negative effect of barrier enclosure (an aerosol box) on the performance of video-assisted intubation in a manikin
Methods:
A total of 41 Emergency Department doctors from a local hospital were recruited to perform intubation in a manikin simulating normal and more difficult airways (Cormack-Lehane grades I and IIb) with and without the box. The primary outcome was time of successful intubation. The secondary outcomes were first-attempt success rate, number of successful attempts, need of adjuncts, dental injury and ease of intubation as perceived by the participants.
Results:
The aerosol box had no significant negative effect on the time of successful intubation (p = 0.630 (Grade I airway) and p = 0.436 (Grade IIb airway)), first-attempt success rate, number of successful attempts, need of adjuncts or dental injury. Participants subjectively reported extra yet minor challenges during intubation in the presence of the box.
Conclusion:
Within limits of the pilot study, the aerosol box had no statistical significant difference but an increasing trend of prolonged endotracheal intubation interval in the Grade IIb airway and negative impact on first-pass success, and could potentially be used to protect healthcare workers during the aerosol-generating intubation procedure.
Introduction
The ongoing Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic has resulted in more than 2 million confirmed cases and 0.2 million deaths as at late April 2020 world-wide. 1 The major modes of transmission are believed to be contact and droplet, and therefore hand-hygiene is an important measure. 2 According to World Health Organization (WHO), during the pandemic, personal protective equipment (PPE) in particular surgical and N95 masks are in extreme shortage globally. 3 WHO has called for increased manufacturing of PPE by 40% to cope with the rising global demand. 4 Locally, in March 2020, Hospital Authority of the Hong Kong Special Administrative Region reported to have a stockpile of 30 million surgical masks adequate for 3 months’ consumption only. 5 This problem of shortage has posed extra risk to healthcare workers especially when performing aerosol-generating procedures (AGP) such as endotracheal intubation (ETI).
ETI is an important, lifesaving procedure performed by emergency physicians, anesthetists and intensivists in critically ill patients requiring acute airway management. It is also applicable for elective cancer surgery under general anaesthesia which cannot be delayed despite the SARS-CoV-2. Because of the potential aerosol-generating risk inherent to ETI, therefore, the barrier enclosure method was introduced informally in Taiwan and Hong Kong during the SARS in 2003, and its use has recently been revisited in the literature in the midst of the pandemic.6–8 Although the efficacy in infection risk reduction is yet to be proven, barrier methods such as an aerosol box appeared to be a simple, reusable and inexpensive way to minimize the risk of transmission outside the vicinity of the box. 6 However, the restriction of movement in the presence of a box has raised the concern of adversely affecting the performance of ETI. This study aimed to investigate the effect of the aerosol box on the performance of intubation in a local hospital.
Methods
This study was a randomized crossover manikin study. No previous study on the barrier method was available for sample size calculation. By convenience sampling, doctors in the Accident and Emergency Department (AED) of Queen Elizabeth Hospital (QEH) in Hong Kong with different years of experience were recruited. Doctors without experience in intubation were excluded.
Our design of the box was based on the aerosol box by Dr. Lai HY (Department of Anaesthesiology, Mennonite Christian Hospital, Taiwan). 9 Video-assisted ETI (using C-Mac®) with and without an aerosol box covering a manikin’s head was performed (An adult manikin, model: ALS Skillmaster 4000 by Laerdal). The box was a self-assembled transparent acrylic open cube with two ports (on the side facing the participant) through which the participants’ hands would be introduced to perform the intubation (Figure 1). All ETIs were performed using a 7 mm cuffed endotracheal tube with C-Mac® disposable blade size 3. Standardized instructions were given to each participant, followed by a 5-min practice session prior to the study. The participants were asked to perform intubation with and without the box, of which the order was randomized by asking the participants to select a concealed envelope containing ‘box’ or ‘no box’. The procedure was then repeated, with and without the box, with restriction of cervical spine motion (manually by the investigator) to simulate a more difficult airway as encountered in a trauma setting. The Cormack-Lehane grading of the airways was determined independently by two anaesthetists with fellowship in Anaesthesia and more than 8 years of clinical practice to be Grade I (no restriction) and Grade IIb (with restriction).
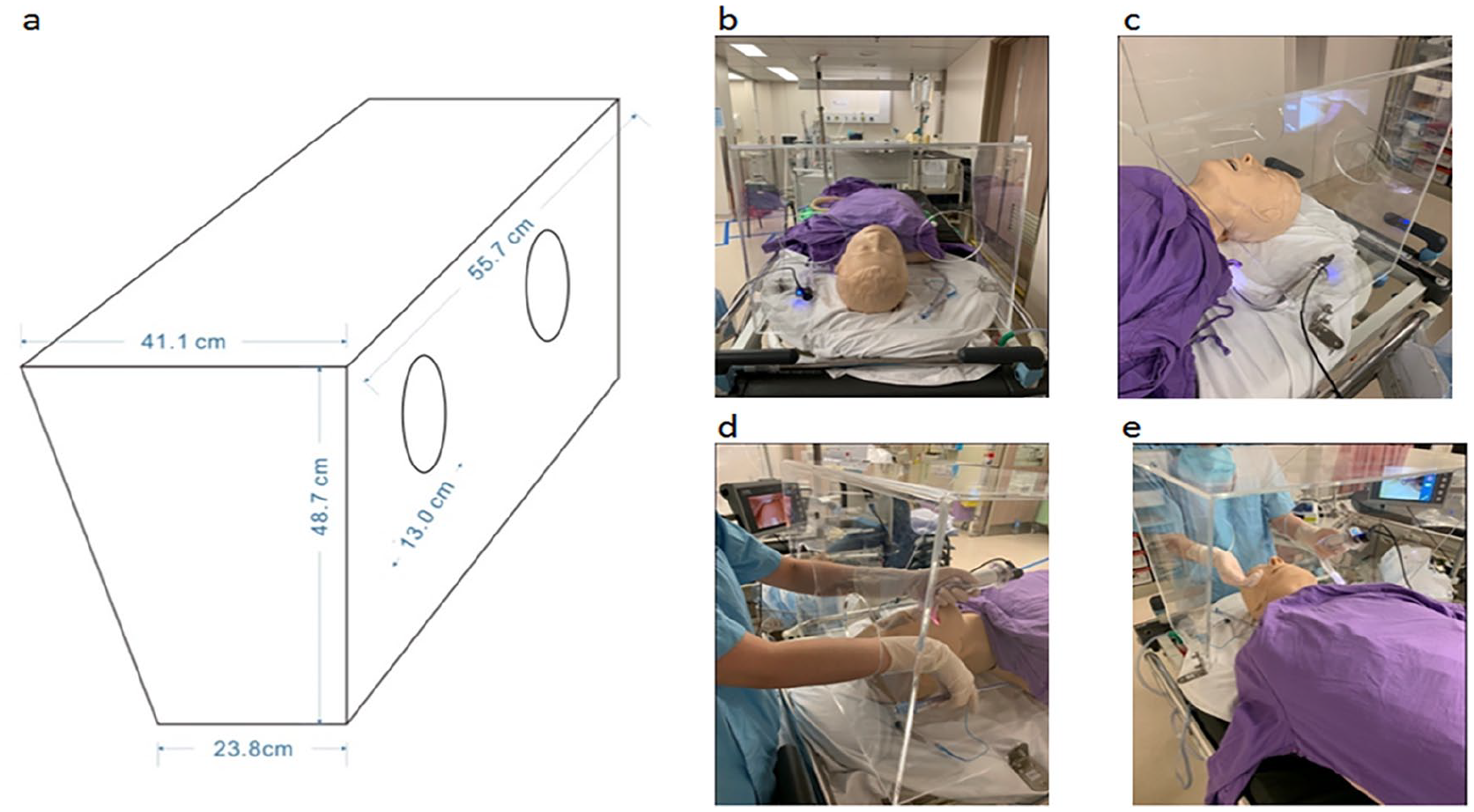
(a) A schematic diagram showing the measurements of the box. (b) and (c) The positions of the aerosol box with the manikin. (d) and (e) participants performing video-assisted ETI through the ports.
The primary outcome was time of successful intubation, which was defined as the time (in seconds) from the blade of the Cmac® passing through the incisors to directly visualized passage of the endotracheal tube cuff beyond the vocal cord. Correct placement of the endotracheal tube was further confirmed by auscultation by the investigator. An additional attempt was defined as withdrawal of endotracheal tube followed by repositioning of the intubating device. Failed ETI was defined as failure to intubate after more than three attempts. The secondary outcomes were first-attempt success rate, number of successful attempts, need of adjuncts, dental injury as evidenced by a click sound of the manikin, and the subjective ease of intubation by the participants using Likert-type scale from 1 to 5.
Using The Statistical Package for Social Sciences (SPSS) version 25, the time for ETI (medians (interquartile range (IQR))) was compared using Mann–Whitney U test. First-attempt success rate, number of attempts, need of adjuncts and dental injury were analysed with Chi-square test/Fisher exact test, where appropriate. For all the statistical analysis, a p-value < 0.05 was regarded as being significant.
Results
Participants’ characteristics
A total of 41 participants were included in the study. 21 out of 41 participants (51.2%) were randomized to perform intubation without the box first in both airway models. 27 (65.9%) had more than 5 years of AED experience while 14 (34.1%) had 5 or less. 19 (46.3%) were specialists in Emergency Medicine while 22 (53.7%) were resident trainees.
Intubation time
In the Grade I airway model, the median time for intubation (seconds) was 13.5 (9.5–23.8) (no box) and 13.1 (9.4–17.3) (with box). In the Grade IIb airway model, the median time for intubation was 16.9 (12.7–25.4) (no box) and 18.4 (12.1–35.2) (with box). In both models, no statistical significant difference was observed (Figures 2 and 3 A).
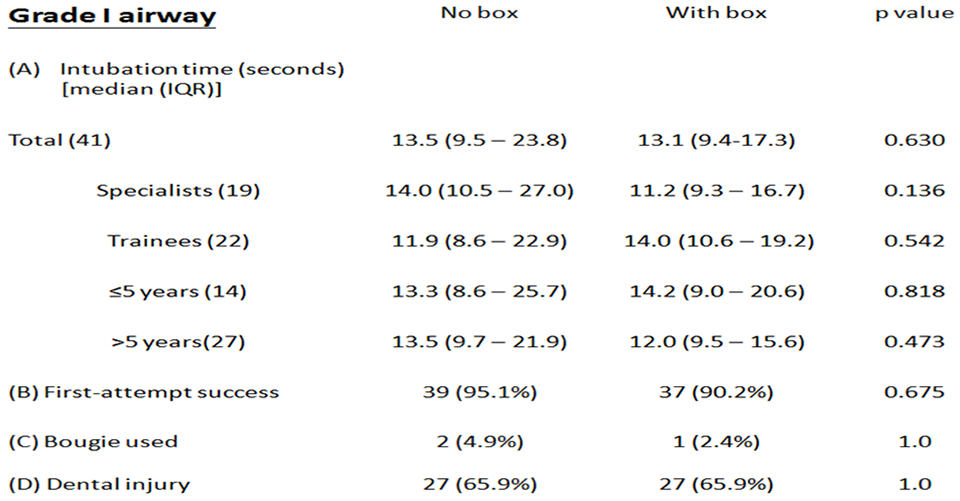
Comparisons of intubation time, first-attempt success, use of bougie and dental injury with and without the box in the Grade I airway.
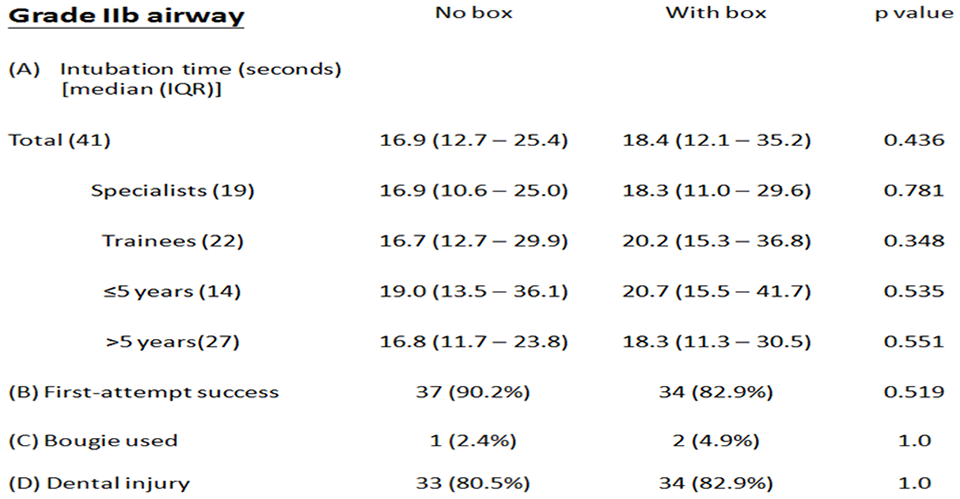
Comparisons of intubation time, first-attempt success, use of bougie and dental injury with and without the box in the Grade IIb airway.
In an attempt to assess whether specialty status and years of experience had any effect on the intubation time, subgroup analyses of specialists Vs trainees and experience (>5 years vs ⩽ 5 years) were performed. As shown in Figures 2 and 3 A, there was no significant difference in the intubation time in both airways in these subgroups.
First-attempt success rate/number of attempts
No failed intubation was observed throughout the study. For the Grade I airway, the first-attempt success rate was respectively 95.1% (39/41) and 90.2% (37/41) in the absence and presence of the box; while for the Grade IIb airway, the respective success rate was 90.2% (37/41) and 82.9% (34/41) (Figures 2 and 3 B). There was a trend of lower success rate of first-pass ETI observed in both airway models. However, there was no statistical difference in the number of attempts of ETI with and without the box in both airways.
Use of adjuncts
There was no statistical difference in the need to apply bougie with and without the box in both airway models (Figures 2 and 3C).
Dental injury
There was no statistical difference in the incidence of dental injury with and without the box, in both airway models (Figures 2 and 3D).
Subjective ease of intubation
Addition of the box reduced the ease of intubation for both airways (Figure 4). In addition, in the presence of the box, only 29% (12/41) of the participants scored 3 or below (neutral to very difficult) with the Grade I airway, while 83% (34/41) of the participants scored the same with the Grade IIb airway.
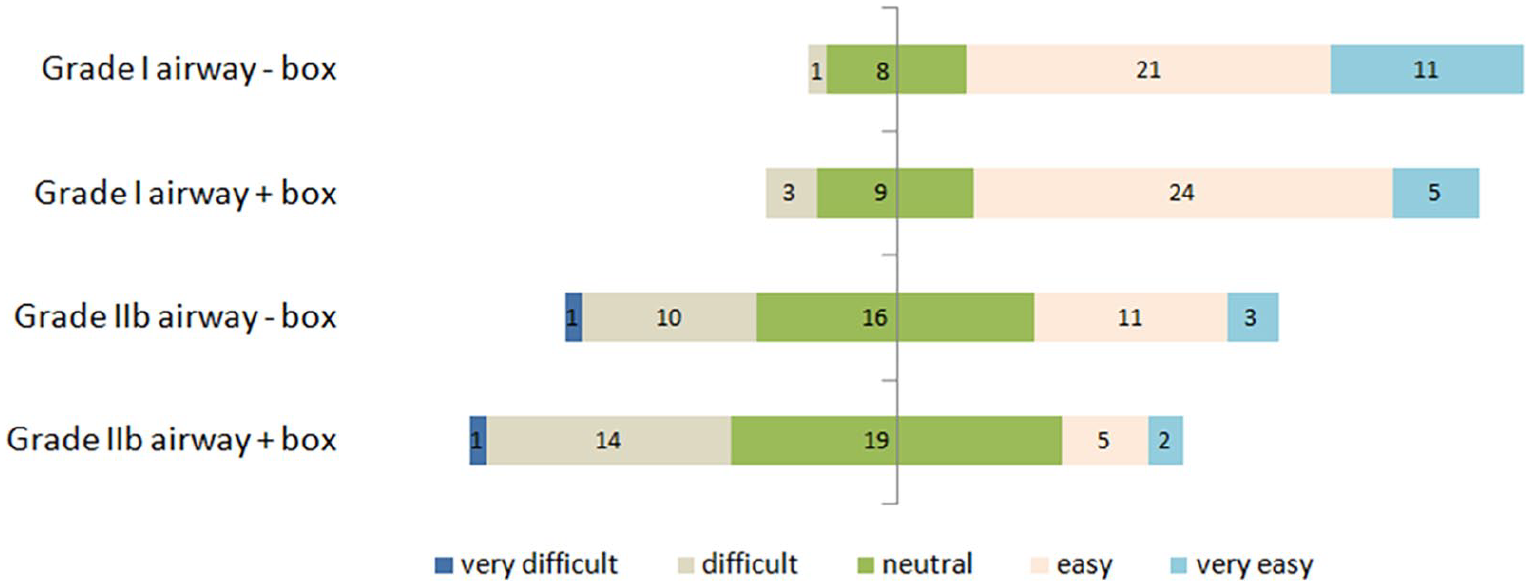
A divering stacked bar chart showing the subjective ease of ETI with and without the box using Linkert type scale.
Discussion
SARS-CoV-2 infection has resulted in a pandemic soon after its emergence in late 2019. 1 Effective protection of healthcare workers is one of the major challenges worldwide. 10 Personal protective equipment such as N95 respirator, fluid-resistant gowns, gloves, eye protection, and so on is getting limited because of sudden tremendous increase in demand and consumption with massive patient load and unstable supply, partly due to restriction of transport between countries and regions. In addition, airborne precautions are recommended during ETI, which is considered as an AGP.2,11 In this regard, innovative and cost-effective means to minimize risk of transmission from suspected or confirmed patients are being devised: one such method is barrier enclosure during intubation.
Our study showed that the aerosol box had no significant effect on the intubation time, number of attempts, use of bougie and dental injury in both airway models, irrespective of clinical experience in terms of years of working in AED or specialist status. That being said, use of the box was reported by the participants to have added extra challenges during the intubation. In other words, despite the subjective feeling that the box might impede the intubation procedure, our study demonstrated that the aerosol box aligns with the ‘do-no-harm’ principle. A larger sample size is needed for verification. Moreover, the best ergonomic requirement of the box needs to be further addressed and evaluated in future studies. Nonetheless, there was a trend of ETI interval increase in the Grade IIb airway, although there was no statistical significance owing to the small sample size. The more important and clinically relevant aspect is whether the interval increase would induce significant hypoxia during ETI. Further studies are warranted for evaluation.
These results suggested that use of an aerosol box can serve as an extra protective device during intubation without compromising the time of intubation in both airways. However, while the use of an aerosol box was shown to reduce aerosol spreading within the containment,6 its clinical efficacy to reduce infection risk remains to be elucidated. Evaluation with fluorescent stain contamination studies is needed in the future.
Concerning the duration of the whole intubation procedure, only the time from the equipment passing through the incisors to the cuff of the endotracheal tube passing through the vocal cord was chosen as our primary outcome in this manikin study. This was because theoretically it is in proportion to the apnoea time and possibility of desaturation in real patients. The subsequent procedures such as connection to ventilators and securing of the ET tube by nursing colleagues were not evaluated, and these could potentially be affected by the box in reality, though to a much lesser extent.
It has been suggested that the aerosol box has some disadvantages, including limited evidence of reducing aerosol dispersal, limited use in short-neck or obese patients, scenarios which require ramping up the patient, difficulty when inserting a bougie or a hyperangulated blade, and possible contamination to assisting staff. 12 Also, cautions have to be exercised to prevent the box from falling off bed resulting in patient or staff injury. Another recent study has reported that the aerosol boxes resulted in longer times to intubation, lower first-pass success rate and damage to PPE. 13 To overcome these disadvantages, modifications of aerosol box designs such as addition of self sealing openings with viral filters, or a suction device to capture aerosols have been suggested. 14 Further studies are needed to shed insights into the influence of these modifications on the dispersion of aerosols. Taken together, we believe that with selected patients and adequate staff training, the box can serve as an adjunct of containing expelled droplets during intubation. However, if difficult airways are anticipated, intubationists should readily abandon the box and use their best trained practice for airway management.
Apart from intubation, AGPs also include other clinical procedures such as non-invasive ventilation with positive pressure, extubation, sputum suction, endoscopy (bronchoscopy and upper gastrointestinal endoscopy, etc.). One recent study has looked into the possibility of collecting nasopharyngeal aspirate with a barrier. 8 The efficacy of barrier enclosure on these other AGPs is yet to be investigated in the future.
Limitations
The small number of participants, use of manikin and simulated intubation settings were the major limitations. In real situations, a multitude of factors can influence the performance of intubation, such as use of PPE, stress, patient factors (airway anatomy, effect of sedation and muscle relaxants, etc.). It is uncertain how the aerosol box will affect the actual intubation procedure.
As a pilot study, the power of this study design might not be adequate. Outliers could potentially affect the statistical calculations. In addition, only doctors from Emergency Department were involved. Recruiting anaesthetists and intensivists would allow a more indepth look into the barrier effect on intubation. Also, convenience sampling involving only the doctors in the centre under study might lead to selection bias and sampling error. The study could be improved by recruiting doctors from other specialties and hospitals, thereby increasing the power and allowing more generalizability and less bias.
Conclusion
With the limits of this small-sized pilot study, it has been demonstrated that the use of an aerosol box had no statistical significant difference but with an increasing trend of ETI interval in a more difficult airway condition, and negative impact on first-pass success. Further studies on the best ergonomic requirement and fluorescent stain contamination evaluation are needed to validate the potential role of barrier enclosure on SARS-CoV-2 and other infectious diseases as a cost-effective adjunct in intubation for extra protection against transmission of infection.
Footnotes
Acknowledgements
The authors would like to thank Ms Katherine Chan, statistician at Queen Elizabeth Hospital, for her statistical support of this publication.
Author contributions
C.K.W., A.L. and C.F.H. conceived the study. C.F.H. was responsible for synthesis of the dataset. C.F.H. and A.L. did literature search, statistical analysis and first draft of the manuscript. C.F.H., A.L. and C.K.W. were responsible for revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Since only volunteers and manikins were involved, no patient’s data were collected. All participants’ identifications were concealed during data collection. Access to password-protected dataset was only limited to the investigators.
Ethical approval
Ethical approval was granted by the Research Ethics Committee of the Kowloon East and Central Clusters of the Hospital Authority, Hong Kong (Reference number: KC/KE-20-0111/ER-1)
Informed consent
Written consent from each participant was obtained before the study.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.