
Abstract
Background:
The Suction-Assisted Laryngoscopy and Airway Decontamination techniques are newly designed emergency airway management skills to assist endotracheal intubation with the complementary use of suction catheters and video laryngoscopes in patients with severe vomiting or massive hematemesis.
Objectives:
To evaluate the performance of emergency department doctors in using the two Suction-Assisted Laryngoscopy and Airway Decontamination techniques (level 1 and level 2) to assist endotracheal intubation by GlideScope® in an airway manikin simulating massive hematemesis, the Nasco airway decontamination simulator.
Methods:
A total of 30 emergency department doctors were recruited in a pilot study. Their performance of using two levels of Suction-Assisted Laryngoscopy and Airway Decontamination techniques (Suction-Assisted Laryngoscopy and Airway Decontamination 1 and Suction-Assisted Laryngoscopy and Airway Decontamination 2) with two different suction catheters, the DuCanto suction catheter and Yankauer suction catheter, were compared with the conventional suction technique. The failed endotracheal intubation rates, time for intubation and number of attempts, amount of aspirated fluid, and the subjective ease of different methods by the participants were compared.
Results:
Irrespective the choice of suction catheter, endotracheal intubation in the manikin by using Suction-Assisted Laryngoscopy and Airway Decontamination 1 had the lowest failure rate which is much better than conventional suction technique (p = 0.012), smaller amount of aspiration compared with the conventional suction technique (p = 0.027), and comparable intubation time with the conventional suction technique (p = 0.850). Most participants were able to intubate the manikin successfully in the first attempt by Suction-Assisted Laryngoscopy and Airway Decontamination 1 with the DuCanto suction catheter, and they were of the opinion that such combination was the most preferred in performing endotracheal intubation.
Conclusion:
Suction-Assisted Laryngoscopy and Airway Decontamination 1 has the best performance in this manikin study, and Suction-Assisted Laryngoscopy and Airway Decontamination 1 with the DuCanto suction catheter was the most favorable method for endotracheal intubation in this manikin study by the participants.
Introduction
Endotracheal intubation (ETI) is an important life-saving procedure in resuscitating critically illed patients. ETI not only ensures oxygenation and ventilation to patients in respiratory failure but also helps to protect the airway from gastric contents and blood in patients with massive hematemesis. Direct laryngoscopy is the standard technique to perform ETI, whereas the airway structures are directly visualized by the provider. However, ETI by direct laryngoscopy is difficult to acquire, and a long training time is often required to master the skill. Traditionally, the use of direct laryngoscopy in aligning the oro-pharyngo-laryngeal axis often poses challenges in emergency and critical situations. The incidents of failed intubation have been reported to be about 1 in 50–100 in the emergency department (ED) 1 and intensive care unit (ICU). 2 Video laryngoscopes are developed to improve airway management by improving the glottis view and also allowing supervision by experienced operator during the intubation process. Recent meta-analysis showed that video laryngoscopes were helpful in reducing the number of failed intubation particularly among patients presenting with a difficult airway. 3 However, despite their enhanced views, the presence of blood or vomitus in the oropharynx remains a major hindrance for successful intubation as the view of the video laryngoscopes may become unavoidably obscured. In a study comparing direct and video laryngoscopy for intubating adult patients with gastrointestinal bleeding retrieved from the third iteration of the National Emergency Airway Registry (NEARIII), ETI by both laryngoscopes had similar proportion of successful first attempts. However, the use of video laryngoscopes rendered a higher rate of device change, although it was not statistically significant due to limited number of cases using video laryngoscopes. 4
In managing patients with massive hematemesis, the traditional practice is to place a suction catheter in the oropharynx to clear out the laryngoscopic view. The major limitation of this practice is the problem of rapid re-accumulation of vomitus and blood in the oropharynx once the suction catheter is removed. Two levels of Suction-Assisted Laryngoscopy and Airway Decontamination (SALAD) techniques (SALAD-1 and SALAD-2) are newly designed emergency airway management skills tailored for patients with severe vomiting or massive hematemesis. The techniques purposely provide constant suction by the placement of suction catheter in the upper airway and hence continuously offer a better laryngoscopic view for ETI. 5 In addition, a specially designed suction catheter, the DuCanto suction catheter, is used to further augment the effectiveness of airway decontamination. The DuCanto catheter has a larger internal diameter than the traditional Yankauer suction catheter making it significantly less likely to be clogged. Also, its hyper-curved contour is designed to fit the oropharyngeal anatomy in order to facilitate the positioning and working with other complementary devices for airway decontamination. Finally, the absence of thumb port allows a more handy control of continuous suction once the catheter is connected to the suction source (Figure 1(c)).
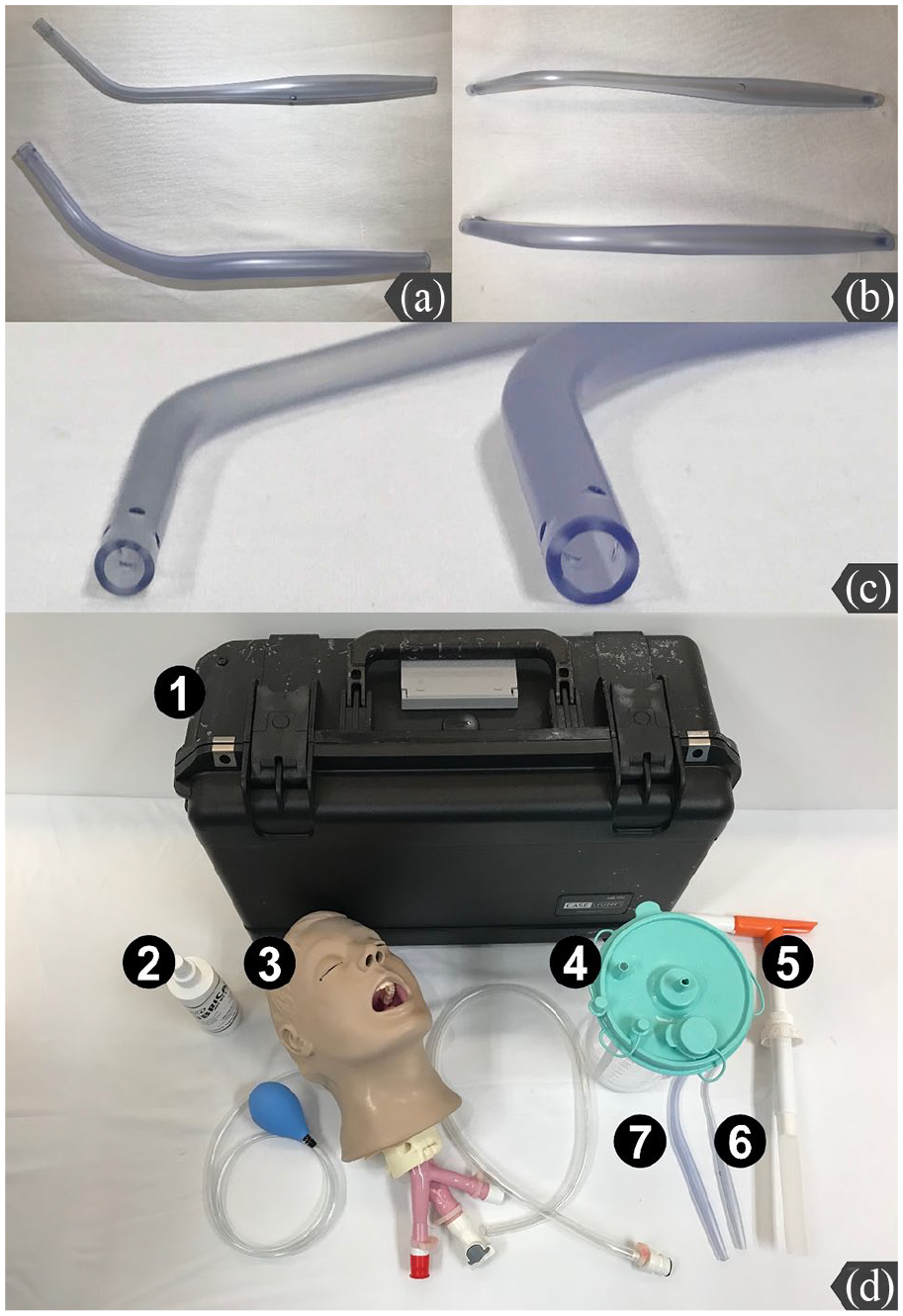
Differences between the DuCanto suction catheter and the Yankauer suction catheter. (a) The DuCanto suction catheter has a hyper-curved shape to fit the oropharyngeal anatomy (upper: Yankauer suction catheter, lower: DuCanto suction catheter). (b) There is no thumb port in the DuCanto suction catheter which allows for continuous suction (upper: Yankauer suction catheter, lower: DuCanto suction catheter). (c) The DuCanto suction catheter has a larger internal diameter than the traditional Yankauer suction catheter (left: Yankauer suction catheter, right: DuCanto suction catheter). (d) Components of the Nasco airway decontamination simulator: (1) case, (2) pump spray lubricant, (3) adult airway management trainer head, (4) suction canister, (5) hand pump, and (6 and 7) suction catheters.
There is no local study about the use of the SALAD techniques in the literature. The purpose of this study is to evaluate the performance of the SALAD techniques and the DuCanto suction catheter to assist ETI by video laryngoscopy in a manikin simulating massive hematemesis (Nasco airway decontamination simulator).
Methods
This was a randomized crossover manikin study. The performances of ED doctors in using the two SALAD techniques and their usual practice (conventional technique) to assist ETI by video laryngoscopy in the Nasco airway decontamination simulator were evaluated and compared. All the participants had clinical experience in ED for at least 2 years. In this study, we also compared the performance of the DuCanto suction catheter with the Yankauer suction catheter.
The participants were instructed to perform ETI by using GlideScope® on the Nasco airway decontamination simulator which was a novel airway training tool that simulates massive emesis. The Nasco airway decontamination simulator was a specially designed intubation manikin with hardware store equipment to allow pumping of simulated airway contaminant (SAC) into the airway (Figure 1).
The SAC was prepared by mixing 500-mL white vinegar with half cup of xanthan gum powder in 1 L of distilled water. Pink watercolor dye was added to the mixture to simulate hematemesis. The flow of SAC was controlled by the investigator who pressed on the hand pump every 6 s. The SAC in the airway was collected in plastic bags, and the amount of the SAC was measured after each ETI.
Standardized training was offered to all participants prior to the study. The training consisted of 5-min demonstration and instruction of the two SALAD techniques by a pre-recorded video.
In SALAD-1, oral decontamination was first performed by suctioning the oropharynx with a suction catheter followed by insertion of the laryngoscopy blade hugging the anterior surface of the tongue, which helped avoid submerging the optical part into the blood and vomitus (Figure 2(a) and (b)). The suction catheter was simultaneously functioned as a tongue lifter for adjusting the best position of the video laryngoscope (Figure 2(c)). After further decontamination of the hypopharynx, larynx, and the proximal esophagus, the suction catheter was then repositioned to the left corner of the patient’s mouth (Figure 2(d)) with its tip inserting into the proximal esophagus for continuous suction (Figure 2(e)). The laryngoscope blade was then slightly rotated leftward 30° to open a channel on right corner of mouth to facilitate endotracheal tube (ETT) passage (Figure 2(f) to (h)). Prior to connection to ventilator, the tracheal tube was suctioned after inflation of the ETT cuff.
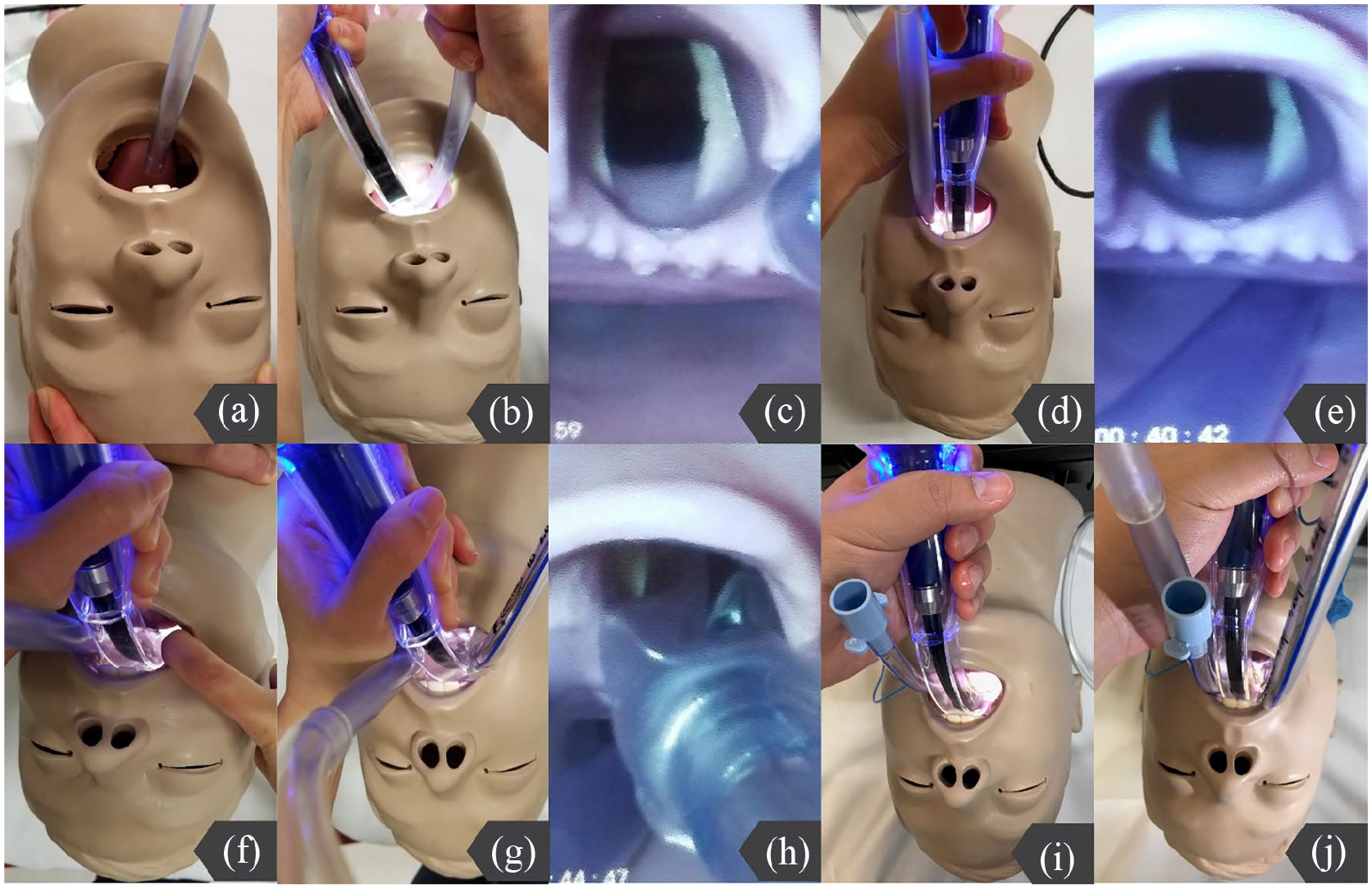
The SALAD level-1 technique: oral decontamination was first performed by suctioning the oropharynx with a suction catheter (a) followed by insertion of the laryngoscopy blade hugging the anterior surface of the tongue. (b) The suction catheter was functioned as a tongue lifter to adjust the position of the video laryngoscope. (c) The suction catheter was then repositioned to the left corner of the patient’s mouth. (d) The tip of suction catheter was inserted into the proximal esophagus for continuous suction. (e) The laryngoscope blade was then slightly rotated leftward 30° to open a channel on right corner of mouth to facilitate ETT passage (f to h). The SALAD-2 technique: an esophageal diversion procedure was first performed by deliberately inserting a 7.0-mm cuffed ETT into the esophagus to divert the gastroesophageal content. (i) ETI was then performed same as SALAD-1 (j).
In SALAD-2, a slight modification was added on top of SALAD-1. An esophageal diversion procedure is first performed. A 7.0-mm cuffed ETT was deliberately inserted into the esophagus to divert the gastroesophageal content (Figure 2(i)). This ETT cuff was inflated after the ETT was inserted into the esophagus to minimize the amount of blood and vomitus entering into the oropharynx. Partial diversion of the airway contamination from esophagus helped improve the effectiveness. ETI was then performed same as SALAD-1 (Figure 2(j)).
The participants were then allowed 10 min to practice ETI by using GlideScope® on the Nasco airway decontamination simulator. Immediate constructive feedback was provided by the investigator during the practice time. After completing the training session, each participant was randomly assigned a sequence of ETI using conventional technique, SALAD-1, and SALAD-2 pairing with either Yankauer suction catheter or DuCanto suction catheter. All the ETI were performed by using a 7.5-mm cuffed ETT with the GlideScope® designed stylet.
The primary outcome measures were the rate of failed ETI, time for intubation, and number of attempts. A failed ETI was defined as the failure to intubate within 180 s or more than three attempts. The time required for successful ETI was defined as the time (in seconds) from touching the laryngoscope to passage of vocal cords with balloon inflation. An attempt was defined as the withdrawal of the intubating device from the mouth followed by repositioning. The secondary outcome was the amount of aspirated fluid in the lungs. The participants were also asked to indicate their subjective ease of ETI with the different techniques on a Likert-type scale from 1 to 5 at the end of the study. Open comments were collected, if any.
The Statistical Package for Social Sciences (SPSS) version 20.0 for Windows was used for analysis. The performances of the participants using the two SALAD techniques and conventional technique with either the Yankauer suction catheter or the DuCanto suction catheter were compared. The time for ETI and the amount of aspirated fluid in the lungs were compared using one-way analysis of variance (ANOVA). For post hoc multiple comparisons, Tukey’s method was used. The number of attempts (one attempt vs more than one attempt) and the failed ETI rate were analyzed using Chi-square test or Fisher’s exact test, if appropriate. The subjective ease of ETI by using different methods was shown in a bar chart. For all statistical analysis, a p-value of less than 0.05 was considered to be significant.
Since there was no previous study on the SALAD techniques which could provide direct relevant figure for the sample size estimation, we conducted a pilot study to evaluate the SALAD techniques in an experimental setting. A convenient sample of 30 ED doctors was recruited. The results of this pilot study could help further evaluation of the SALAD techniques in different settings.
Results
Comparison of ETI failure rate
Comparing the performance of the three suction techniques, SALAD-1 could achieve zero failure rate of ETI despite which catheter was used. SALAD-1 significantly performed better than conventional suction technique (p = 0.012) with less ETI failure while there was no significant difference between SALAD-1 and SALAD-2 (p = 0.079). When using DuCanto suction catheter, the ETI failure rate were similar using either technique (p = 0.355). However, when using Yankauer catheter, SALAD-1 was noted to be superior than the conventional technique (p = 0.020) (Table 1).
Analysis of the failure rate of ETI by using different methods.
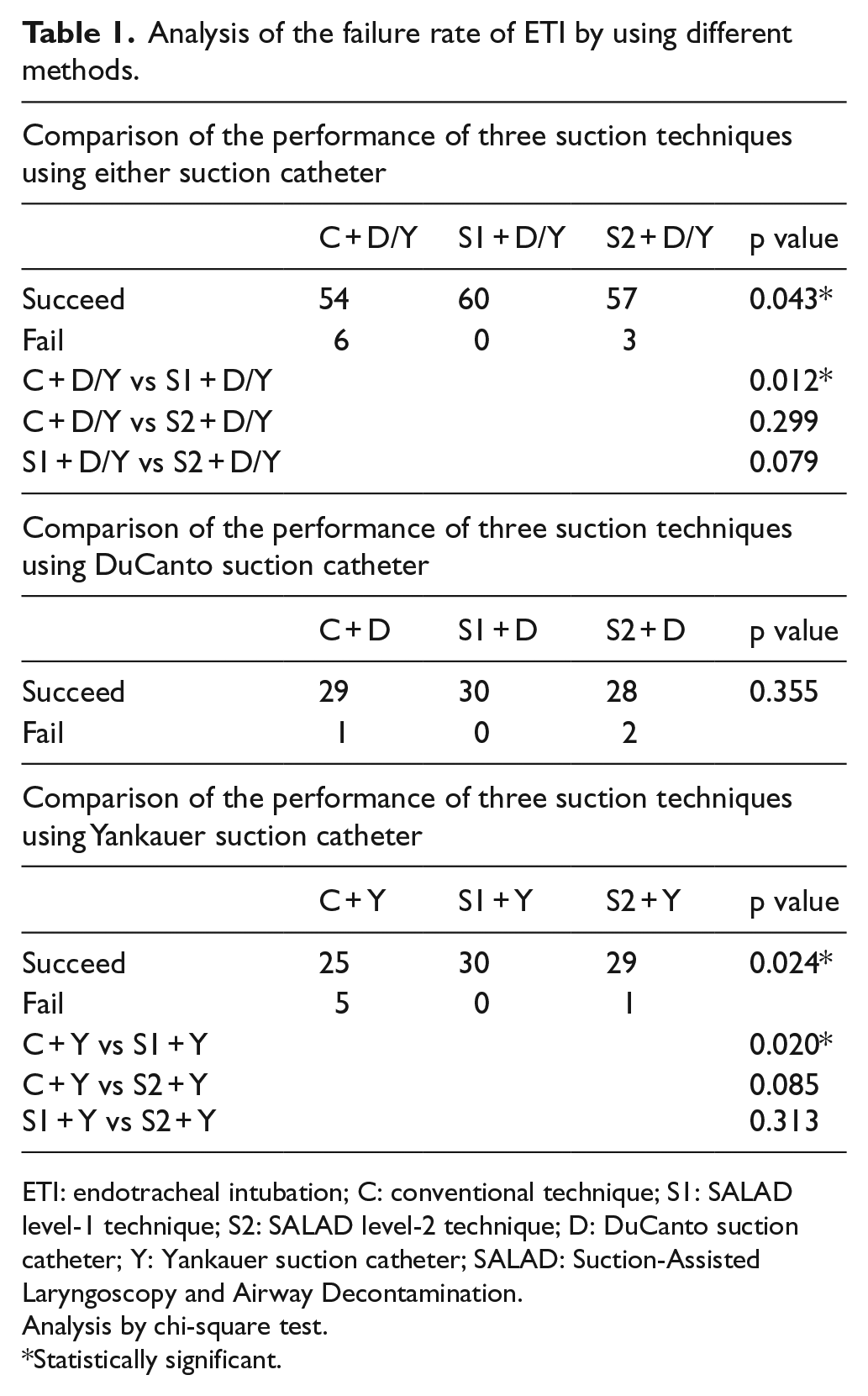
ETI: endotracheal intubation; C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; D: DuCanto suction catheter; Y: Yankauer suction catheter; SALAD: Suction-Assisted Laryngoscopy and Airway Decontamination.
Analysis by chi-square test.
Statistically significant.
Comparison of the intubation time
When using either suction catheter, both SALAD-1 and conventional technique performed equally well (mean intubation time: 43.7 vs 47.4 s, p = 0.850), while that by SALAD-2 was significantly lengthened (mean intubation time: 70.1 s; vs SALAD-1, p < 0.001; vs conventional, p = 0.003). Nevertheless, the above difference can only be observed in the sub-group analysis when DuCanto suction catheter was used. The shortest mean intubation time was achieved by using SALAD-1 with combination of DuCanto suction catheter (mean intubation time: 35.8 s), and the most time-consuming one was SALAD-2 with combination of Yankauer catheter (mean intubation time: 73.6 s) (Table 2).
Analysis of intubation time and amount of aspiration by using different methods.
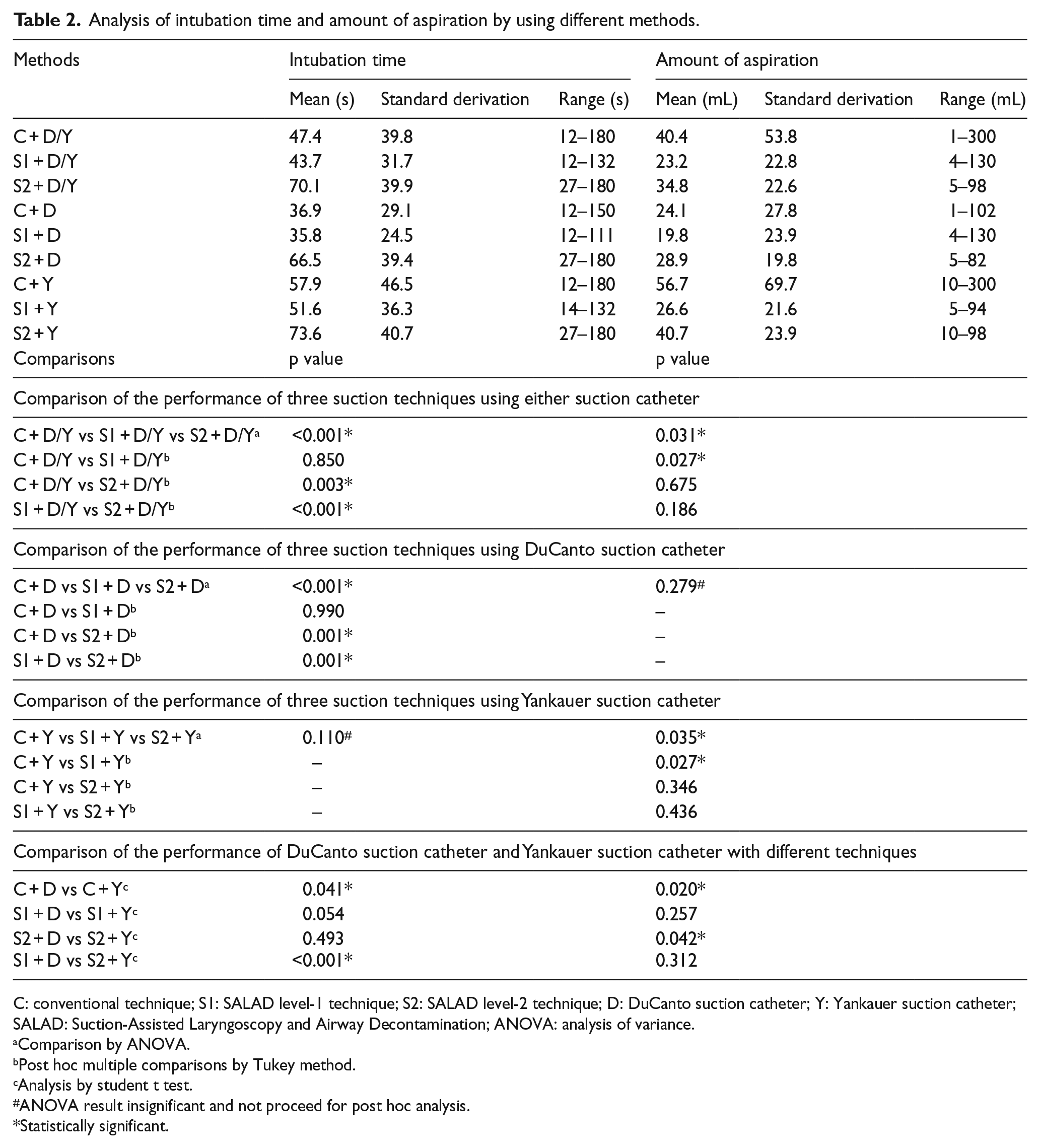
C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; D: DuCanto suction catheter; Y: Yankauer suction catheter; SALAD: Suction-Assisted Laryngoscopy and Airway Decontamination; ANOVA: analysis of variance.
Comparison by ANOVA.
Post hoc multiple comparisons by Tukey method.
Analysis by student t test.
ANOVA result insignificant and not proceed for post hoc analysis.
Statistically significant.
Comparison of amounts of aspiration
In general, SALAD-1 resulted in the smallest amount of aspiration when using either suction catheter (mean amount aspiration: 23.2 mL) while conventional technique resulted in the largest amount of aspiration (mean amount aspiration: 40.4 mL). The amount of aspiration was significantly reduced using SALAD-1 when compared with conventional suction technique (p = 0.027) though the difference was not significant when compared to SALAD-2 (p = 0.186). The choice of catheter mattered only when performing conventional technique or SALAD-2. Less aspiration was resulted when the DuCanto suction catheter was chosen for these two techniques (conventional: p = 0.020, SALAD-2: p = 0.042). Meanwhile, the degree of aspiration was equally well-controlled by SALAD-1 despite which catheter was used (Table 2).
Comparison of the first attempt success rate
The first attempt success rates of the three suction techniques were similar (p = 0.531). Although SALAD-1 apparently had a higher rate of success in first-go, the result was not statistically significant (Table 3).
Analysis of the first attempt succeed rate by using different methods.
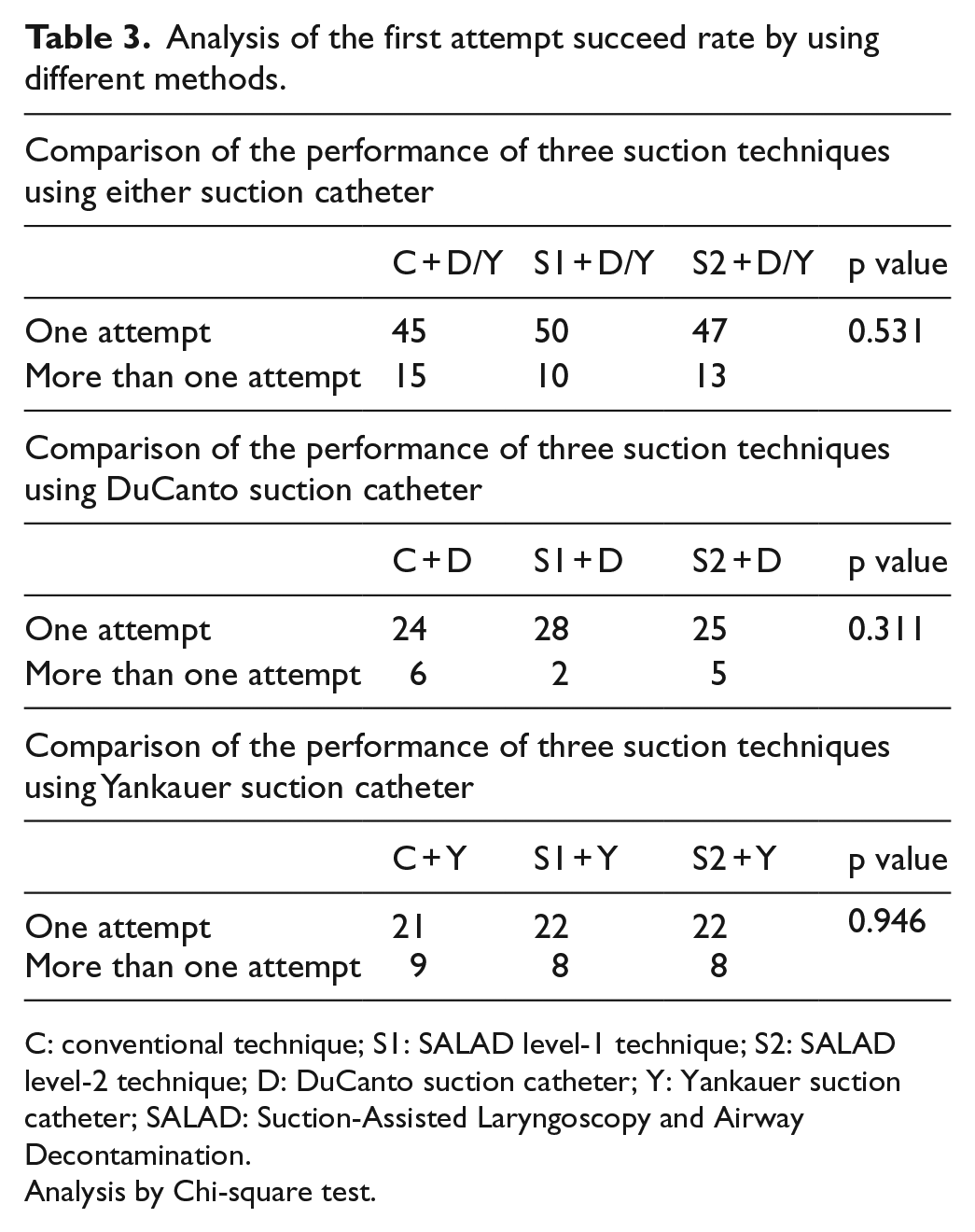
C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; D: DuCanto suction catheter; Y: Yankauer suction catheter; SALAD: Suction-Assisted Laryngoscopy and Airway Decontamination.
Analysis by Chi-square test.
Participant’s subjective ease of choice
Considering the participant’s scoring on the ease, performing SALAD-1 using the DuCanto suction catheter had the highest mean and median scores for the subjective ease, that is, 80% of the participants scored 4 or above. On the other hand, only 25% of the participants scored 4 or above for SALAD-2 using the Yankauer suction catheter, which had the lowest mean score (Figure 3).
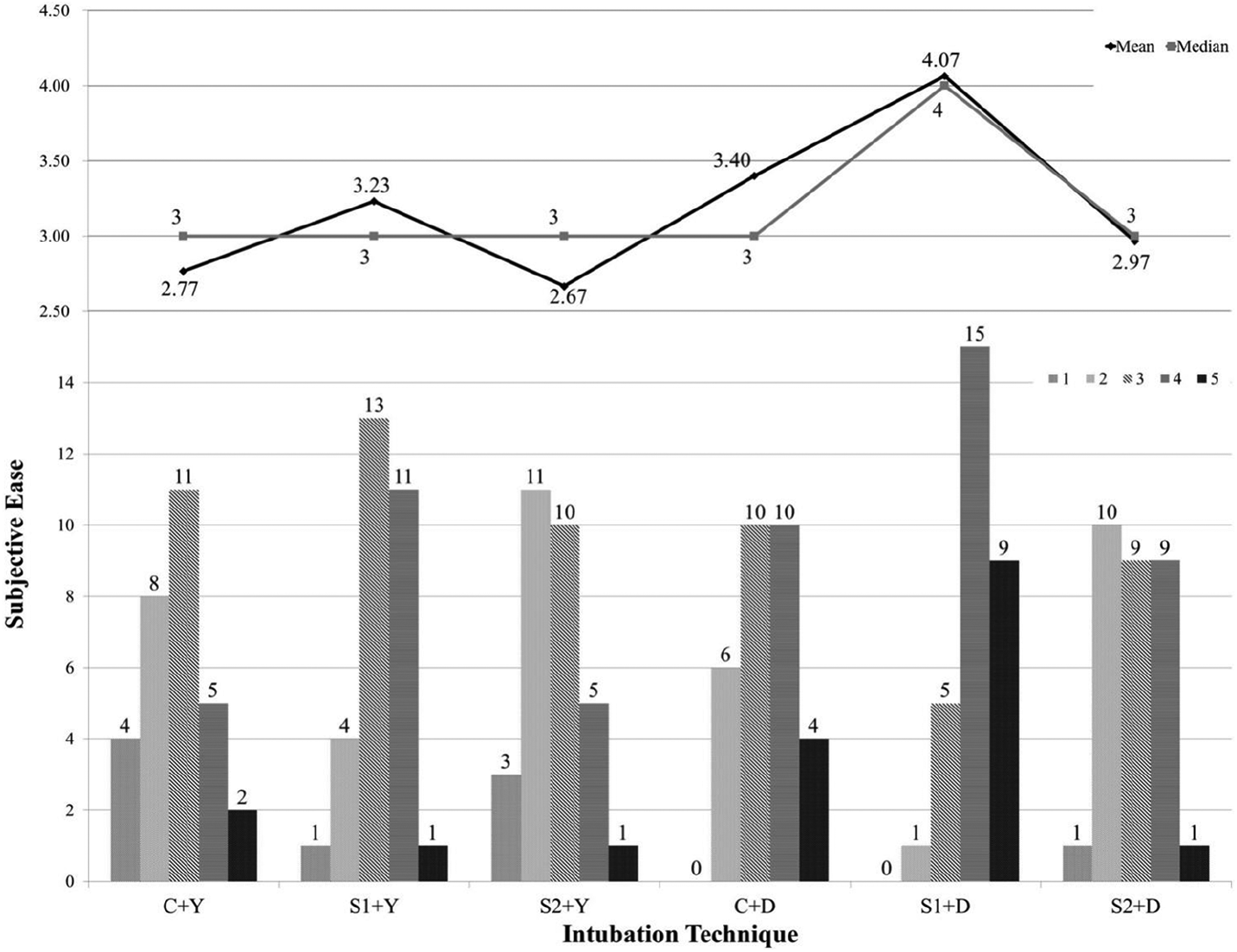
Bar chart of participants’ subjective ease.
Discussion
Blood and vomitus in the airway are the major predictors and challenges of difficult intubation6–8 which could pose a great threat for the emergency airway management. The training of ETI using the SALAD techniques in the airway manikin simulating severe vomiting and massive hematemesis has been shown to improve the confidence of emergency physicians in managing such situations in the real patients. 5
Video laryngoscopy can provide superior intubating view compared to direct laryngoscopy, and it was proven to improve the successful rate of ETI in heavily contaminated airway situations.9–11 Compared to direct laryngoscopy, GlideScope® has been shown to improve the first attempt successful ETI rate and shorten the intubation time. However, similar benefits were not observed in the experts. 12
However, the performance of different video laryngoscopes may vary in operators with different specialty training and experience. Further studies on different video laryngoscopes are warranted to validate the use of SALAD techniques on them.13,14
In our study, we have demonstrated that using SALAD-1, irrespective the choice of catheter, had superior performance compared with conventional technique or SALAD-2 in general. All the participants performed well using SALAD-1 in which zero failure rate was achieved, and the intubation times were comparatively shorter. Moreover, the combination of SALAD-1 with the DuCanto suction catheter even striked the highest first attempt success rate, the least amount of aspiration and was being the favorite choice by the participants among all other technique combinations. The subjective ease of learning and mastering SALAD-1 skill for new learner and the efficient way of rate of airway decontamination by the large-bore DuCanto catheter could explained the results.
On the contrary, our results demonstrated the combination of conventional technique with Yankauer suction catheter was associated the highest overall failure rate of ETI, the lowest first attempt success rate, and resulting the largest amount of aspiration in performing ETI using GlideScope®. In view of the poor performance, the low scores of subjective ease by the participants were expected. However, one of the participants successfully intubate the manikin in extremely short intubation time using conventional technique paired with Yankauer suction catheter and resulted in small amount of aspiration. It could probably an outlying result due to chance.
The amount of aspiration was greatest in the group of conventional technique with use of Yankauer suction catheter. Although the conventional technique had been well-known and well-practiced by most of the participants, the rate of decontamination by Yankauer catheter was limited by its relatively smaller diameter compared with the DuCanto suction catheter. Indeed, the large amount of aspirated content could clinically imply a significant risk of aspiration pneumonia in real patients.
Owing to the extra step of esophageal diversion in SALAD-2, participants unavoidably required more time to perform ETI compared with the other two techniques. A major reported concern from the participants about SALAD-2 was the limited physical space available for placement of all the devices including ETT for esophageal diversion, suction catheter, and GlideScope®, leaving too little room to proceed for a smooth ETI. Its downside was compatible with the result of a relatively low first attempt success rate. Although the esophageal diversion procedure in SALAD-2 was intentionally designed to minimize the aspiration into the lungs, the long intubation time and high frequency of repeated attempts may counteract its intention for airway protection and may reflect the limited applicability of this designed technique.
Though our study did not focus on the choice of catheter, yet in the sub-group analysis, our findings revealed that the DuCanto suction catheter was more effective than the Yankauer suction catheter in clearing the SAC in the oral cavity of the manikin as evidenced from the results. The DuCanto suction catheter also demonstrated a significant lower failure rate of ETI, shorter intubation time and less amount of aspiration even using the conventional technique. While comparing with Yankauer suction catheter, the first attempt success rate was the lowest in all three techniques which means that it could be difficult to intubate the patient in one-go using Yankauer suction catheter in situation of massive emesis. Again, this could be greatly attributed to its smaller internal diameter which hinders a rapid decontamination of the laryngoscopic view.
In conclusion, SALAD-1 had the best performance among the three suction techniques, and the DuCanto suction catheter had better performance than the Yankauer suction catheter. In addition, a large portion of participants indicated that SALAD-1 together with the DuCanto suction catheter was the most preferred method for ETI in this manikin study.
Limitations
There were several limitations in our study. As most of the ED doctors were familiar with their own practice (conventional technique) in performing ETI, despite a 15-min training session was offered, the handling of the newly acquired techniques may not be comparable with their well-handled conventional technique. Also, the years of clinical experience in airway management may also affect the performance of individual ED doctors. The seniorities of different ED doctors were not analyzed in this pilot study and bias might be introduced in the overall results. Therefore, further studies involving brand-new learners such as medical students may be able to demonstrate a better unbiased results.
Another important limitation of the study is that the possible complications of ETI associated with different techniques such as tooth dislodgement, airway trauma, and oro-mucosal trauma were not measured. Furthermore, the solid food substance and blood clots in the vomitus may clog the suction catheter in real situation. These associated complications may have important implications on the clinical applicability of different techniques in real lives.
Likewise in all manikin studies, clinician’s challenges in real situation were influenced by multiple factors, including stress in crash condition, distractions during resuscitation, complementary use of sedation and muscle relaxants, and so on. These factors could greatly influence the performance of the doctors. Similarly, the rigid nature of the manikin’s airway and the simulated intermittent flow of vomitus by pumping may be far real patient situation.
Being a pilot study, the power of this pilot study might not be optimal enough to detect the significant differences in the performance for these three suction techniques. Outlier may distort the study result significantly in this small sample size pilot study, for example, one of the participant was able to spent 12 s to intubate the manikin without adequate clearing of the laryngoscopic view. His result might lead to over-estimation or under-estimation of the overall performance of the conventional technique.
Finally, only ED doctors were recruited in this study, other specialists including intensivists and anesthesiologists were not involved, the results may limit the generalizability of this study. Further larger scale studies involving different specialties are warranted for improving the power and the generalizability of these techniques.
Conclusion
The Nasco airway decontamination simulator and the SALAD techniques are good educational tools for doctors in training intubation in patients with severe vomiting and massive hematemesis. We have demonstrated that SALAD-1 irrespective the choice of catheter had the best performance among the three suction techniques and SALAD-1 together with the DuCanto suction catheter was the most favorable method for ETI in this manikin study by the participants. Further studies and more clinical experience are needed to validate the effectiveness of the SALAD techniques in real patients with heavily contaminated airway situations.
Footnotes
Acknowledgements
The authors would like to thank Dr James DuCanto MD, Director of the Simulation Center Aurora St. Luke’s Medical Center, for demonstration of the SALAD techniques, all the emergency doctors to participate in this study, particularly, Dr YY Hui and Dr William Chan, and Mr Lee Wing Chung, Secretary of Accident and Emergency Department of North Lantau Hospital for the clerical support of this publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All the equipment used was purchased by the Accident and Emergency Department (AED) of North Lantau Hospital (NLTH).
Availability of data and materials
All participants’ identifications were removed before storage. The master dataset was kept by the investigators in computer, and password was required to open the file. Access to the data would be limited to the investigators and clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact principal investigator for further information of the data is required.
Informed consent
Informed consent was waived by the Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Ethical approval
This study was approved by the Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.