
Abstract
Background:
The suction-assisted laryngoscopy and airway decontamination (SALAD) techniques (level 1, SALAD-1 and level 2, SALAD-2) are newly proposed airway management skills to facilitate endotracheal intubation in patients with massive haematemesis. A pilot study using GlideScope® demonstrated the superior performance of SALAD-1 technique in massive haematemesis simulation.
Objectives:
To compare the performance of three different video laryngoscopes (the GlideScope®, the Airtraq® and the C-MAC®) in endotracheal intubation using SALAD techniques by emergency doctors in a manikin simulating massive haematemesis.
Methods:
Forty-eight emergency doctors were recruited. The participants’ performance of endotracheal intubation using the GlideScope®, the Airtraq® and the C-MAC® with the conventional and the two SALAD techniques in a manikin simulating massive haematemesis was evaluated. The time for intubation, number of attempts, rate of failed intubation, amount of aspirated fluid and the subjective ease of different devices and techniques were compared.
Results:
The C-MAC® had shorter intubation time compared with GlideScope® when using conventional (mean intubation time: 28.48 vs 47.00 s, p = 0.018) and SALAD-1 technique (mean intubation time: 29.35 vs 43.25 s, p < 0.039). The intubation time of all three video laryngoscopes was similar in SALAD-2 technique. There was no significant difference in the number of attempts and failed intubation rate among different video laryngoscopes in using different techniques. Intubation with the C-MAC® resulted in the least mean amount of aspiration in all the conventional (35.63 mL), SALAD-1 (14.06 mL) and SALAD-2 (18.13 mL) techniques. However, the results were not significantly different from the GlideScope® and the Airtraq®. The C-MAC® was rated the most favourable video laryngoscope for the SALAD-1 technique (p < 0.001). There was no significant preference for different video laryngoscopes in using the SALAD-2 technique (p = 0.111).
Conclusion:
All the video laryngoscopes have similar intubation performance with the SALAD-1 and SALAD-2 techniques. The C-MAC® performed better than GlideScope® in terms of intubation time. The C-MAC® was the most favourable video laryngoscope for the SALAD-1 technique.
Introduction
Emergency airway management is essential in resuscitation. 1 The rapid establishment of a secured airway by endotracheal intubation (ETI) is important for oxygenation and ventilation. It also protects the airway from aspiration. In patients with massive haematemesis, the large amount of blood and vomitus increases the risk of aspiration and subsequent aspiration pneumonia. Failed ETI can result in undesirable outcomes such as death and brain damage. 2 The incidence of difficult or failed tracheal intubation can be up to 15% in the Emergency Department and the Intensive Care Unit. 3
For decades, ETI is accomplished by direct laryngoscopy (DL). It necessitates the alignment of the laryngeal, pharyngeal and oral axes to achieve the best possible view of the glottis, 4 which can be difficult in the emergency settings. In addition, proficiency in DL requires substantial amount of training, exposure and experience. 5
In recent years, video laryngoscopes (VLs) are developed as alternatives to DL. The key difference between DL and VL is that VL is equipped with a video camera, providing an indirect view of the glottis. Various VLs differ in their specifications, user interfaces and geometries. They can be broadly categorized into Macintosh type (e.g. the C-MAC®), angulated blade type (e.g. the GlideScope®) and tube-channel type (e.g. the Airtraq®). 6 Lewis et al. 7 concluded in a recent Cochrane Review that VL improves the glottic view and may reduce the number of failed intubations especially in difficult airway scenarios. In addition, VL allows the sharing of the view of the larynx with others and helps facilitating of supervision. 8
However, the presence of blood and vomitus in the airway in case of massive haematemesis poses additional challenges to ETI by VL as the view may become obscured. When intubating such patients, the traditional practice is first clear up the blood or vomitus by placing a suction catheter in the oropharynx, followed by ETI either by DL or VL. Unavoidably, the blood and vomitus usually reaccumulate rapidly once the suction catheter is removed while the ETT (Endotracheal Tube) could be readily picked up. The need of a constant suction to remove the reaccuumlating vomitus becomes an important issue in order to allow an optimal visualization of the airway structures.
Recently, DuCanto et al. 9 proposed the suction-assisted laryngoscopy and airway decontamination (SALAD) techniques for airway management in patients with severe vomiting or massive haematemesis, which can be further divided into SALAD level-1 (SALAD-1) and SALAD level-2 (SALAD-2) techniques. It involves the decontamination of the airway while preserving the VL view for ETI concurrently. The DuCanto suction catheter, a newly designed catheter dedicated for complementary use with the SALAD techniques, is also introduced. It differs from the conventional Yankauer suction catheter that it has a larger internal diameter to prevent clogging, a hyper-curved shape fitting the oropharyngeal anatomy for positioning and has no thumb port, which allows continuous suctioning (Figure 1(a) to (c)).
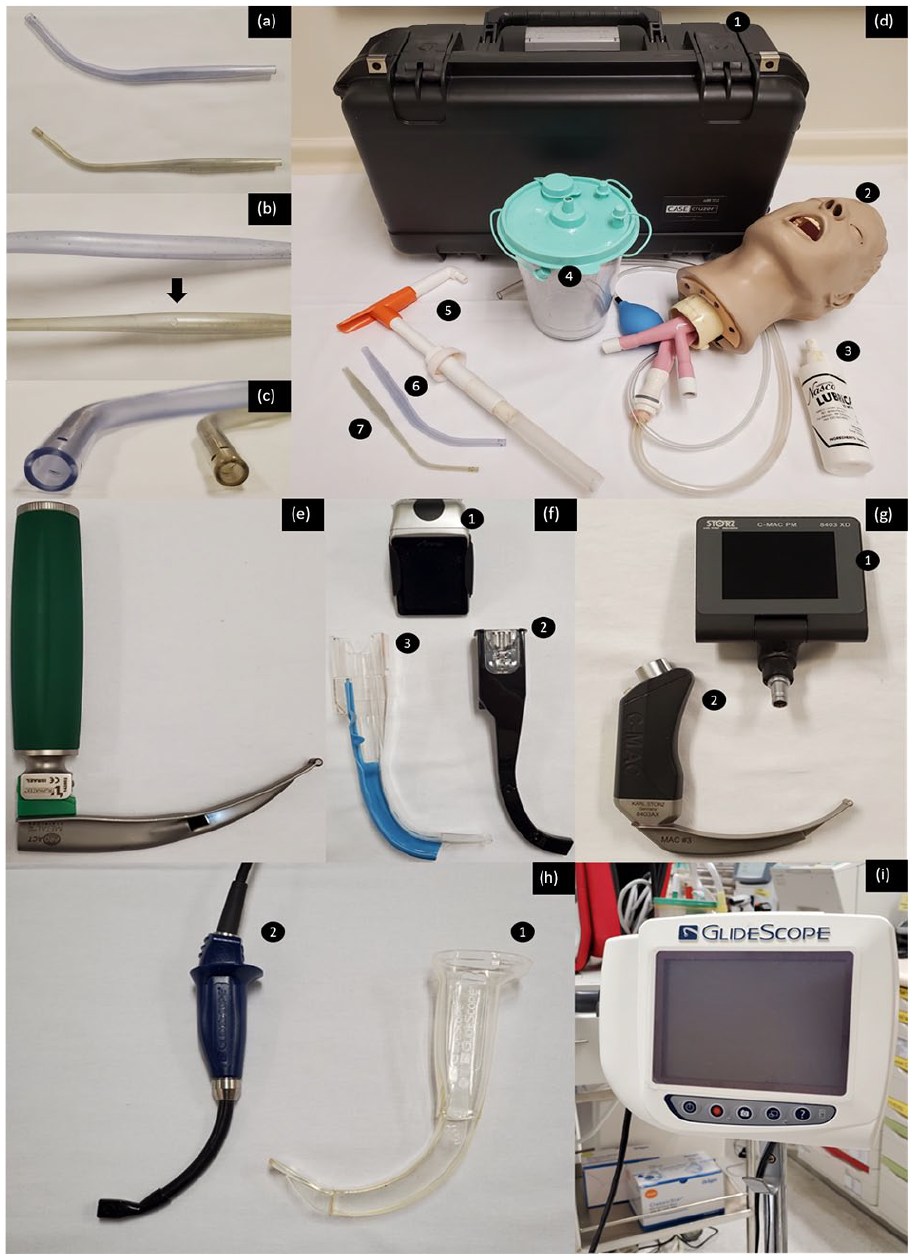
Differences between the Yankauer and the DuCanto suction catheter. (a) The DuCanto suction catheter is hyper curved in shape for better fitting of the oropharyngeal anatomy (upper: DuCanto suction catheter and lower: Yankauer suction catheter). (b) Note the absence of thumb port in the DuCanto catheter. The thumb port of the Yankauer suction catheter is indicated by the black arrow (upper: DuCanto suction catheter and lower: Yankauer suction catheter). (c) The DuCanto suction catheter has a larger internal diameter than the Yankauer suction catheter (left: DuCanto suction catheter and right: Yankauer suction catheter). (d) Components of the Nasco airway decontamination simulator include (1) case, (2) adult airway management trainer head, (3) pump spray lubricant, (4) suction canister, (5) hand pump and (6 and 7) suction catheters. (e) Conventional Macintosh blade for direct laryngoscopy. (f) The Airtraq® with (1) the video composite unit, (2) reusable optic device and (3) disposable blade. (g) The C-MAC® with (1) portable pocket monitor and (2) standard C-MAC® blade. (h) The GlideScope® with (1) disposable clear plastic protective blade and (2) flexible video baton. (i) The GlideScope® monitor.
A pilot manikin study evaluating the performance of 30 emergency doctors using the SALAD techniques to assist ETI by GlideScope® was done in our department. Two different suction catheters, the Yankauer suction catheter and the DuCanto suction catheter, were also compared. 10 The Nasco airway decontamination simulator, a novel airway training tool for simulating massive emesis, 9 was used to stimulate a patient with massive haematemesis. It was shown that the SALAD level-1 technique with the DuCanto suction catheter had superior performance with lower failed ETI rate, higher first attempt success rate and smaller amount of aspiration. However, in this pilot study, only GlideScope® was used. The usage of other VLs with different designs had not been studied. In fact, it was shown in previous studies that there might be other more favourable alternatives than GlideScope®. In a manikin study comparing the performances of ETI by medical students using the Airtraq®, the C-Mac® and the GlideScope®, the Airtraq® was found to be better than other two VLs regarding the intubation time and the ease of ETI. 11 In another manikin study comparing the usefulness of the C-MAC®, the GlideScope® and the Airtraq® in ETI by experienced anaesthetists, the C-MAC® demonstrated the shortest tracheal intubation time in difficult laryngoscopy scenarios and was rated as the easiest VL to use. GlideScope® in fact performed less well in both easy and difficulty scenarios. 12 Further studies are necessary to evaluate the performance of different VLs. The purpose of this study is to compare the performance of the GlideScope®, the Airtraq® and the C-MAC® in ETI using the SALAD techniques in a manikin simulating massive haematemesis.
Methods
This study was a manikin study with randomized sequence of ETI with different methods. The performance of ETI by emergency doctors using the GlideScope®, the Airtraq® and the C-MAC® with the two SALAD techniques and the conventional suction technique in a manikin simulating massive haematemesis was assessed and compared.
The participants were instructed to perform ETI using the conventional, the SALAD-1 and the SALAD-2 techniques on the Nasco airway decontamination simulator. It was a specially designed airway training manikin in which a clear vinyl tubing was attached to its oesophagus. The tubing was then connected to a reservoir which contained simulated airway contaminant (SAC). The SAC was then pumped from the reservoir into the airway to simulate massive haematemesis 9 (Figure 1(d)).
The SAC was prepared in a similar fashion as in our previous pilot study. 10 0.5 L of white vinegar was mixed with half a cup of xanthan gum powder in 1 L of water. To simulate blood in haematemesis, red food colouring was added to the mixture. The investigator pressed on the hand pump every 6 s to control the flow of the SAC. The ‘aspirated’ SAC was then collected in plastic bags, and the amount was measured after each successful ETI.
Before the study, each participant was trained to familiarize with the SALAD techniques. The standardized training consisted of 5-min demonstrations and instructions of the two SALAD (SALAD-1 and SALAD-2) techniques by a pre-taped video. The participants were then allowed 30 min to practise ETI using the GlideScope®, the Airtraq® and the C-MAC® on the Nasco airway decontamination manikin with constructive feedback from the investigators.
In the SALAD level-1 technique, the oropharynx was first suctioned for oral decontamination. The laryngoscope blade was then inserted, hugging the anterior surface of the tongue to prevent the optical part from dipping into the blood and vomitus (Figure 2(a) and (b)). The suction catheter was also simultaneously used as a tongue lifter to adjust the optimal position of the laryngoscope (Figure 2(c)). Further decontamination of the hypopharynx, the larynx and the proximal oesophagus was performed. The suction catheter was then repositioned to the left corner of the patient’s mouth (the left park) (Figure 2(d)) with its tip inserting into the proximal oesophagus to provide continuous suction (Figure 2(e)). The laryngoscope blade was then slightly rotated 30° towards the left to open a channel on the right corner of the mouth for ETT passage (Figure 2(f) to (h)). After inflation of the ETT cuff, suctioning of the tracheal tube was performed before connecting to the ventilator.
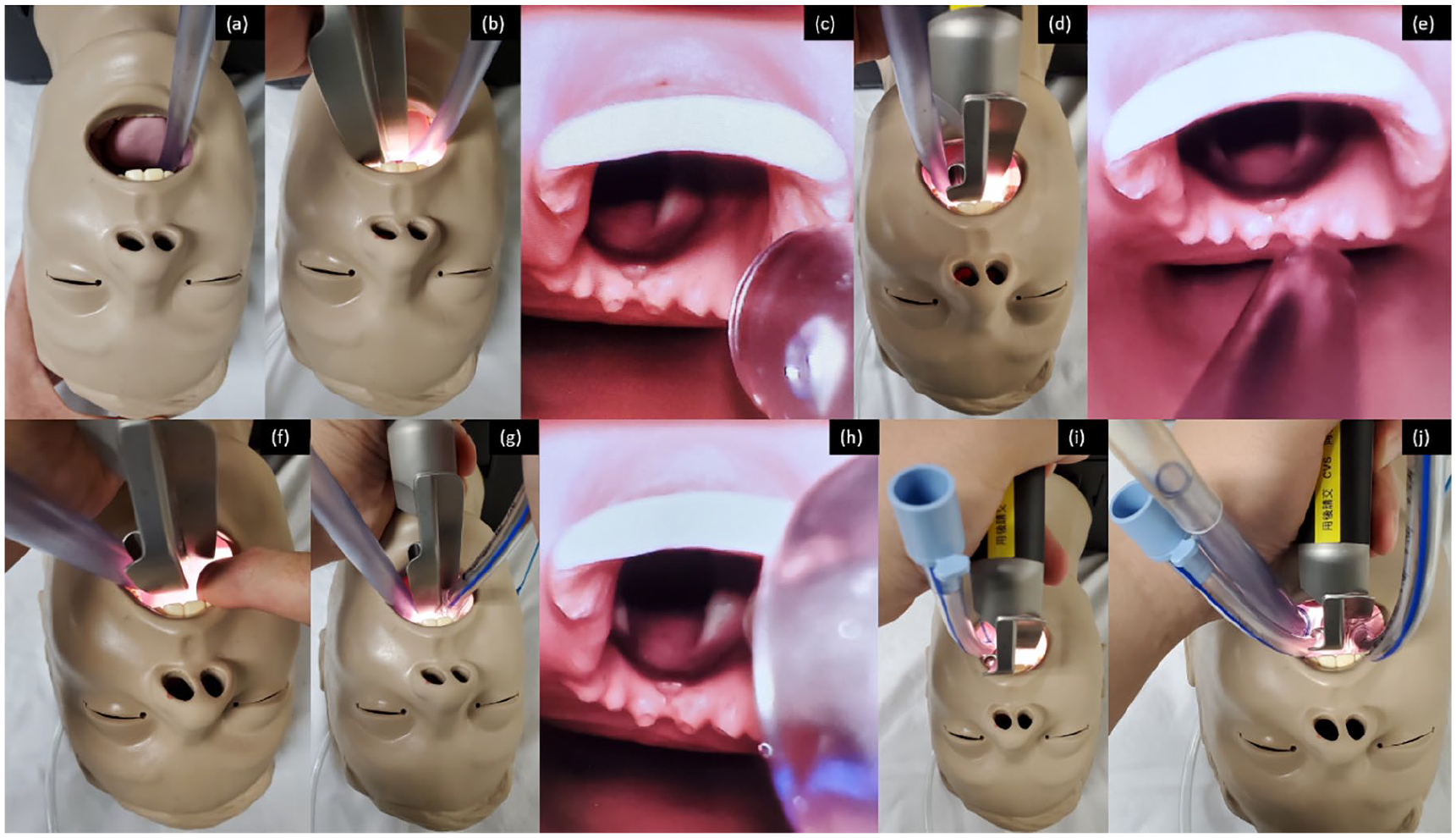
The SALAD-1 technique demonstrated with the C-MAC®. (a) The oropharynx was first suctioned for oral decontamination. (b) The laryngoscope blade was inserted hugging the anterior surface of the tongue. (c) The suction catheter functioned as a tongue lifter to adjust the optimal position of the laryngoscope. (d) The suction catheter was then repositioned to the left corner of the mouth (the left park). (e) The tip of the suction catheter was inserted into the proximal oesophagus to provide continuous suctioning. (f–h) The laryngoscopy blade was slightly rotated 30° to the left for opening up a channel at the right corner of the mouth for passage of the ETT. (i) The SALAD-2 technique started with deliberate insertion of ETT into the oesophagus for additional oesophageal diversion. (j) ETT was performed using the SALAD-2 technique procedures afterwards.
In the SALAD level-2 technique, an additional oesophageal diversion procedure was first performed by deliberate insertion of a 7.0-mm cuffed ETT into the oesophagus. The ETT cuff was then inflated to prevent blood and vomitus from entering the oropharynx (Figure 2(i)). The objective of this partial diversion was to maximize the effectiveness of the SALAD techniques. ETI was then performed following the SALAD level-1 technique procedures (Figure 2(j)).
During the study, the participants were randomly assigned the sequence of ETI by different techniques (conventional suction technique, the SALAD-1 technique and the SALAD-2 technique) using the GlideScope® (GVL 3 Stat, Figure 1(i) and (j)), the Airtraq® (Regular Size 3 blade, Figure 1(f)) and the C-MAC®(Macintosh #3 blade, Figure 1(g)) with the DuCanto suction catheter. An ETI attempt using traditional DL (Macintosh Size 3 blade, Figure 1(e)) with the conventional Yankauer suction catheter was also included to serve as a control. All intubations were performed using a 7.5-mm cuffed ETT.
The primary outcome measures in this study were the time for intubation, number of attempts and rate of failed ETI. The secondary outcomes were the amount of aspirated fluid in the lungs. The participants were also asked to rate their subjective ease of successful ETI attempts using different devices and techniques on a Likert-type scale (from 1 to 5) at the end of the study. The time required for successful ETI was defined as the time (in seconds) from touching the laryngoscope to passage of vocal cords with balloon inflation. An attempt was defined as a withdrawal of the intubating device from the mouth followed by repositioning. A failed intubation was defined as wrong ETT position, failure to intubate in less than 180 s, or if more than three attempts were required. Any open comments from the participants were also collected.
The Statistical Package for Social Sciences (SPSS) version 20.0 for Windows was used for analysis. The performance of the control (using DL), the two SALAD techniques and the conventional suction technique using the GlideScope®, the Airtraq® and the C-MAC® were compared. The time for ETI and the amount of aspirated fluid were compared using the one-way analysis of variance (ANOVA). For post hoc multiple comparisons, Tukey’s method was used. The number of attempts (three attempts vs more than three attempts) and the rate of failed ETI were analysed using the chi-square test or Fisher’s exact test if appropriate. The subjective ease of ETI using different devices and methods was shown in bar chart and was compared by the Kruskal–Wallis test. The Mann–Whitney U test was used for post hoc comparisons by the Bonferroni correction. For all statistical analyses, a p-value of less than 0.05 was considered significant.
The sample size estimation was based on the duration of successful ETI attempt. From the results of our pilot study, 10 the duration of ETI attempt by the SALAD level-2 technique using the GlideScope® and the DuCanto suction catheter was 66.5 s with standard deviation of 39.4 s. In a previous manikin study of ETI in easy laryngoscopy scenario by experienced anaesthetists, the mean durations of first ETI attempt by the C-MAC®, the Airtraq® and the GlideScope® were 16, 22 and 33 s, respectively. 12 We considered the effect size to be 33% reduction of the ETI time, that is, the differences in the mean durations of first ETI by the C-MAC®, the Airtraq® and the GlideScope® in the previous study, with α = 0.05 and β = 0.2. Therefore, we estimated that a sample size of 48 was required.
Results
A total of 48 emergency doctors working in our department were recruited in this study. This included doctors rotating from the Princess Margaret Hospital, a major acute general hospital.
Comparison of the intubation time
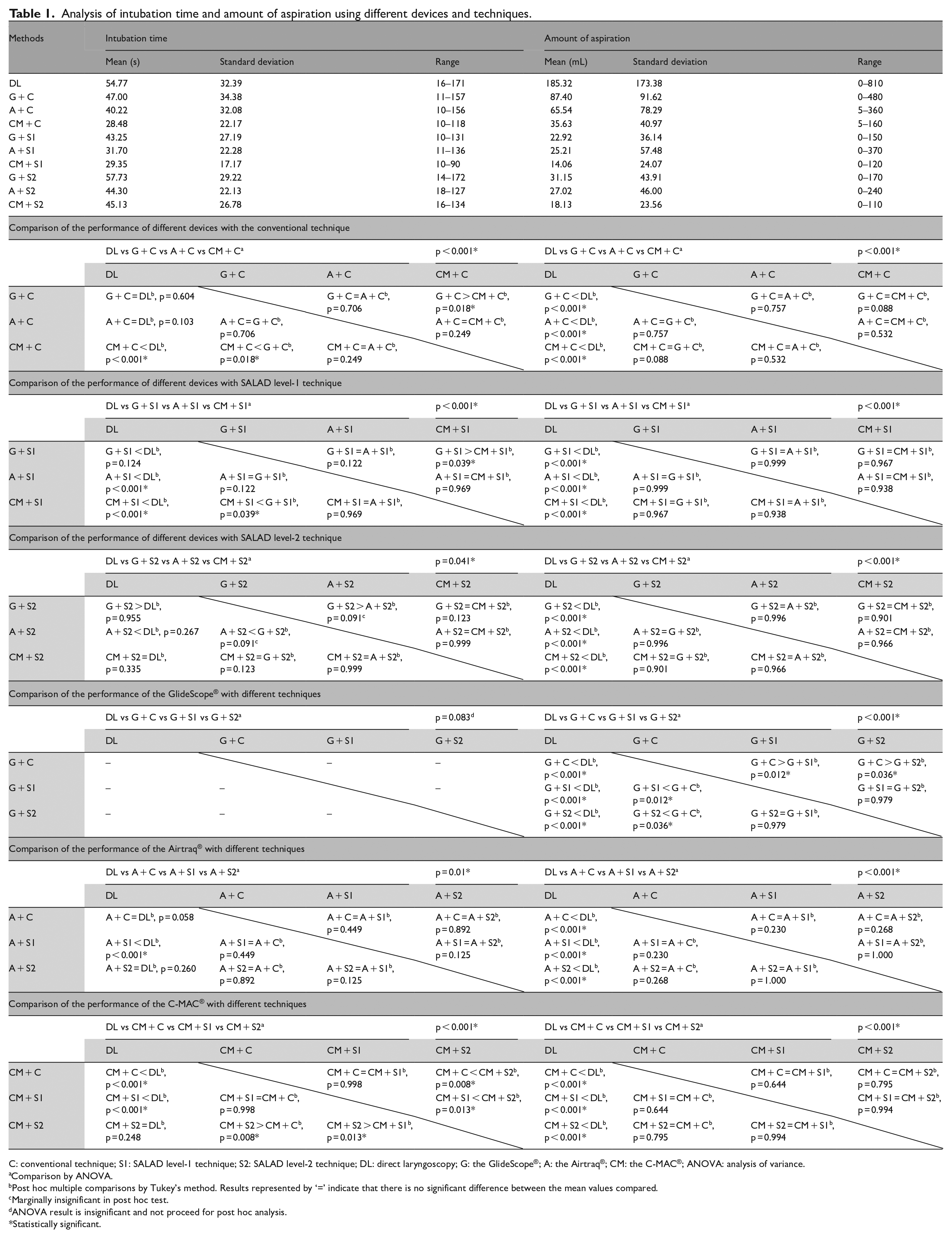
When using the conventional method for ETI, the C-MAC® had the shortest mean intubation time (28.48 s) (Table 1). Comparing the traditional DL with different VLs, the traditional DL required significantly longer time for intubation than the C-MAC® (mean intubation time: 54.77 vs 28.48 s, p < 0.001). There were no significant differences in the intubation time between DL and the GlideScope® and between DL and the Airtraq®. Comparing the performance of different VLs, the C-MAC® performed significantly better than the GlideScope® (mean intubation time: 28.48 vs 47.00 s, p = 0.018). However, there were no significant differences in the intubation time between the C-MAC® and the Airtraq® and between the GlideScope® and the Airtraq®.
Analysis of intubation time and amount of aspiration using different devices and techniques.
C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; DL: direct laryngoscopy; G: the GlideScope®; A: the Airtraq®; CM: the C-MAC®; ANOVA: analysis of variance.
Comparison by ANOVA.
Post hoc multiple comparisons by Tukey’s method. Results represented by ‘=’ indicate that there is no significant difference between the mean values compared.
Marginally insignificant in post hoc test.
ANOVA result is insignificant and not proceed for post hoc analysis.
Statistically significant.
In using the SALAD-1 technique, the C-MAC® still had the shortest mean intubation time (29.35 s). Comparing the traditional DL with different VLs, the traditional DL required significantly longer time for intubation than the C-MAC® (mean intubation time: 54.77 vs 29.35 s, p < 0.001) and the Airtraq® (mean intubation time: 54.77 vs 31.70 s, p < 0.001). There was no significant difference in the intubation time between DL and the GlideScope®. Comparing the performance between different VLs, the C-MAC® performed better than GlideScope® (mean intubation time: 29.35 vs 43.25 s, p = 0.039). However, there were no significant differences between the C-MAC® and the Airtraq® and between the GlideScope® and the Airtraq®.
For the SALAD-2 technique, the Airtraq® had the shortest mean intubation time (44.30 s). There were no significant differences in the intubation time when comparing DL with the three different VLs. ANOVA analysis showed statistically significant difference in the time for intubation using different devices (p = 0.041). However, only a marginally insignificant longer time was noted in post hoc tests by Tukey’s method when comparing the GlideScope® with the Airtraq® (mean intubation time: 57.73 vs 44.30 s, p = 0.091).
Concerning the performance of individual VL with different intubation methods, the time spent for ETI with the three intubation methods was similar for the GlideScope® and the Airtraq®. For the C-MAC®, the SALAD-2 technique was more time-consuming than the conventional technique (mean intubation time: 45.13 vs 28.48 s, p = 0.008) and the SALAD-1 technique (mean intubation time: 45.13 vs 29.35 s, p = 0.013).
Comparison of the number of attempts
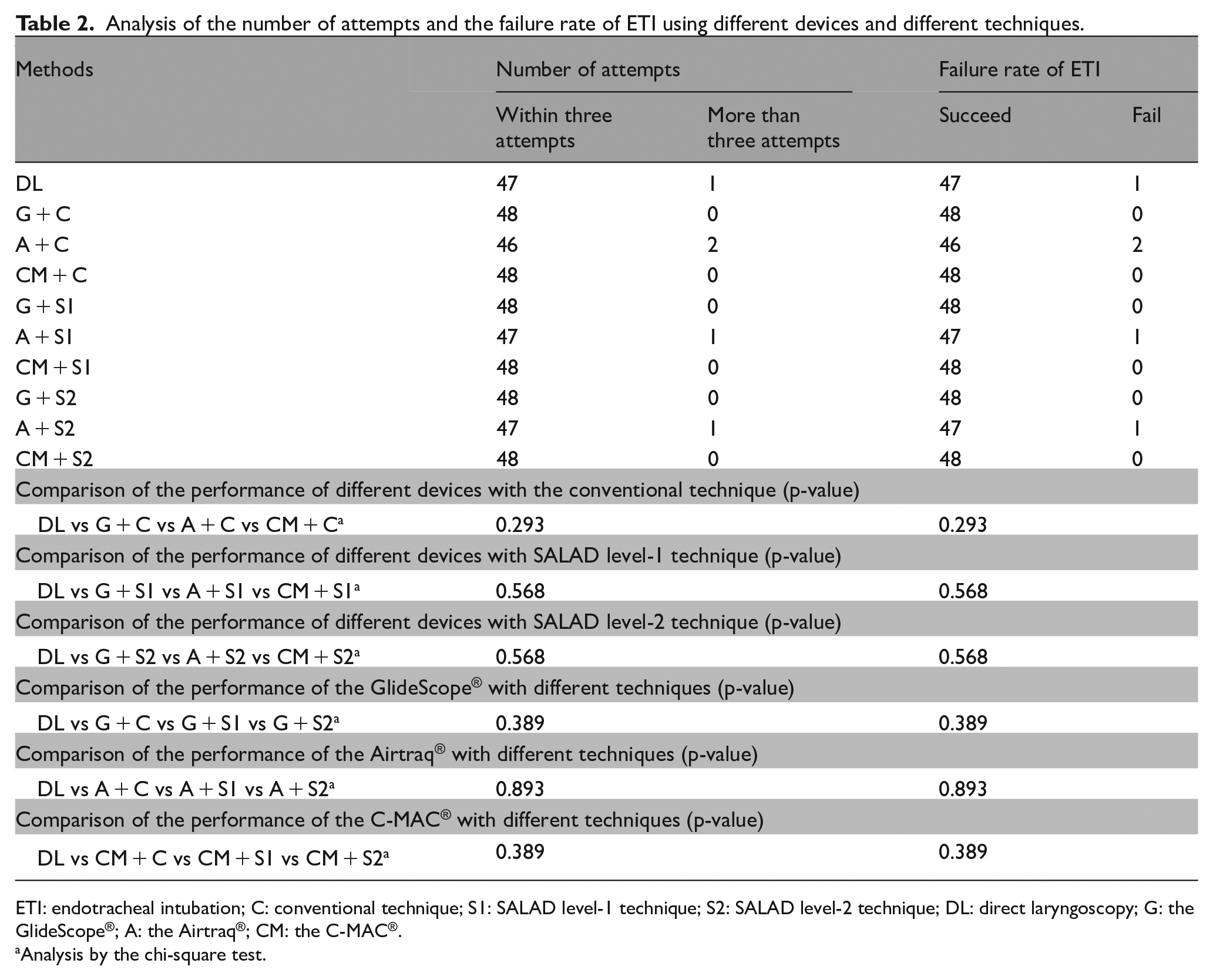
No statistically significant difference was detected when comparing whether participants could intubate within three attempts or required more than three attempts with different devices and different techniques (Table 2).
Analysis of the number of attempts and the failure rate of ETI using different devices and different techniques.
ETI: endotracheal intubation; C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; DL: direct laryngoscopy; G: the GlideScope®; A: the Airtraq®; CM: the C-MAC®.
Analysis by the chi-square test.
Comparison of ETI failure rate
Both the C-MAC® and GlideScope® managed to achieve zero failure rate with different techniques (Table 2). In using the Airtraq®, two participants failed ETI with the conventional method, one failed with the SALAD-1 technique and one failed with the SALAD-2 technique. One participant failed to intubate with the traditional DL technique. However, the differences were not statistically significant.
Comparison of amounts of aspiration
For the conventional method, ETI with DL yielded the largest amount of aspiration (mean amount aspiration: 185.32 mL) which was significantly larger comparing with different devices and different methods (p < 0.001) (Table 1).
Similar results were found when using either the SALAD-1 technique or the SALAD-2 technique for ETI. Although intubation with the C-MAC® resulted in the least mean amount of aspiration in all the conventional method (35.63 mL), SALAD-1 (14.06 mL) and SALAD-2 (18.13 mL) techniques, the results were not significantly different from those of the GlideScope® and the Airtraq®.
In using the GlideScope®, significantly larger amount of aspiration was resulted using the conventional technique when compared with both the SALAD-1 (mean amount aspiration: 87.40 vs 22.92 mL, p = 0.012) and SALAD-2 techniques (mean amount aspiration: 87.40 vs 31.15 mL, p = 0.036). For the Airtraq® and the C-MAC®, the amount aspirated was similar in all the conventional, SALAD-1 and SALAD-2 techniques.
Participants’ subjective ease
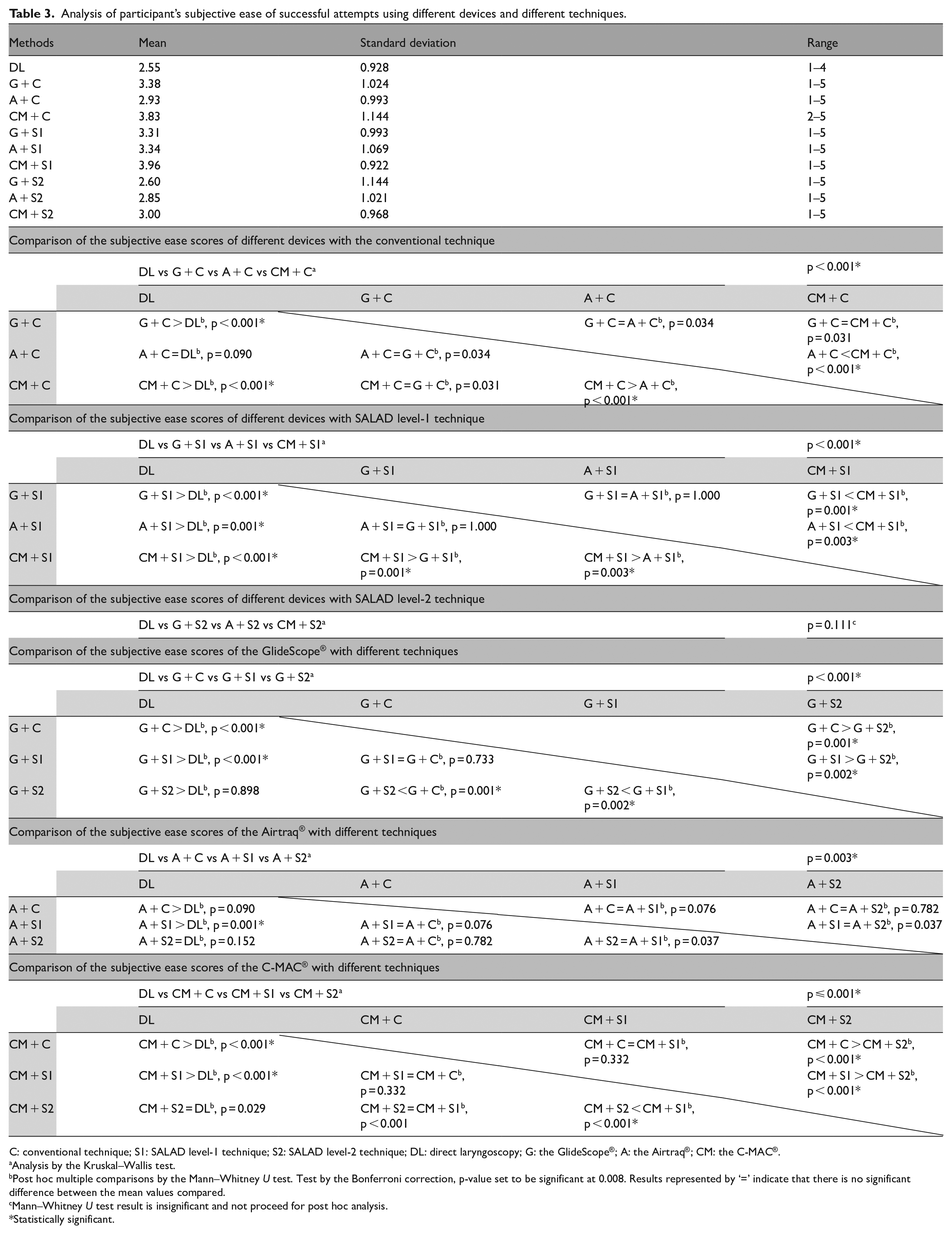
For the conventional method, participants found that the C-MAC® is the easiest to use (mean score: 3.83) (Table 3 and Figure 3). The score was significantly higher when compared to the Airtraq® (mean score: 3.83 vs 2.93, p < 0.001). Participants rated that DL was significantly more difficult for ETI than the GlideScope® (mean score: 2.55 vs 3.38, p < 0.001) and the C-MAC® (mean score: 2.55 vs 3.83, p < 0.001).
Analysis of participant’s subjective ease of successful attempts using different devices and different techniques.
C: conventional technique; S1: SALAD level-1 technique; S2: SALAD level-2 technique; DL: direct laryngoscopy; G: the GlideScope®; A: the Airtraq®; CM: the C-MAC®.
Analysis by the Kruskal–Wallis test.
Post hoc multiple comparisons by the Mann–Whitney U test. Test by the Bonferroni correction, p-value set to be significant at 0.008. Results represented by ‘=’ indicate that there is no significant difference between the mean values compared.
Mann–Whitney U test result is insignificant and not proceed for post hoc analysis.
Statistically significant.
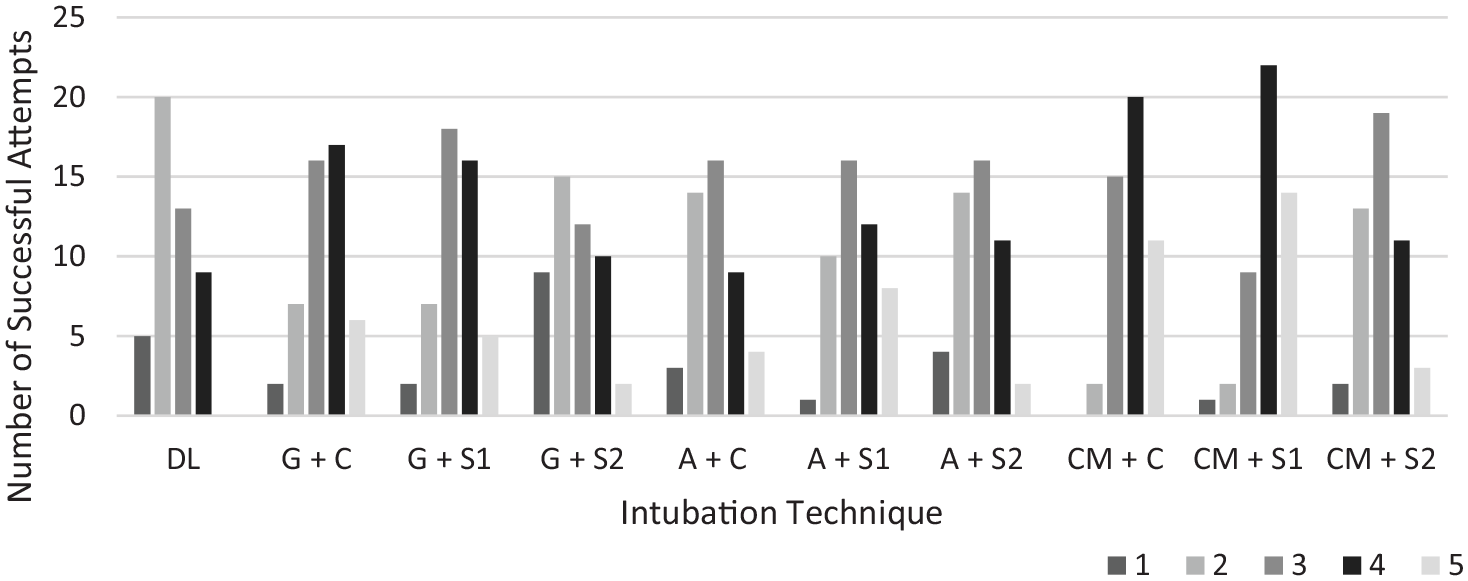
Bar chart of participants’ subjective ease.
For the SALAD-1 technique, the C-MAC® scored the highest among different devices (mean score: 3.96). The score was significantly higher than those of the GlideScope® (mean score: 3.96 vs 3.31, p = 0.001) and the Airtraq® (mean score: 3.96 vs 3.34, p = 0.03). Using DL was significantly more difficult for ETI than the GlideScope® (mean score: 2.55 vs 3.31, p < 0.001), the Airtraq® (mean score: 2.55 vs 3.34, p < 0.001) and the C-MAC® (mean score 2.55 vs 3.96, p < 0.001).
For the SALAD-2 technique, the C-MAC® had the highest mean score of 3.00 for subjective ease. However, there was no significant difference in the scores of different devices.
In using the GlideScope®, ETI with the SALAD-2 technique was the most difficult with a significantly lower subjective ease score than the conventional method (mean score: 2.60 vs 3.38, p = 0.001) and the SALAD-1 technique (mean score: 2.60 vs 3.31, p = 0.002). There was no significant difference in the scores for the Airtraq® using the conventional, SALAD-1 and SALAD-2 techniques. For the C-MAC®, participants found that it was the most difficult in using the SALAD-2 technique with significant lower scores than the conventional method (mean score: 3.00 vs 3.83, p < 0.001) and the SALAD-1 technique (mean score: 3.00 vs 3.96, p < 0.001).
Discussion
ETI plays an important role in resuscitating the critically ill. The presence of blood and vomitus in the airway is undesirable for successful ETI.13,14 The SALAD techniques had been designed to facilitate ETI in patients with massive haematemesis or severe vomiting. 9 In our previous pilot study, the SALAD-1 technique outperformed the conventional suction method. SALAD-1 and the DuCanto suction catheter was the most preferred combination for ETI. 10 GlideScope® had been employed in this pilot study. When comparing the performance of SALAD-1 with GlideScope® and traditional DL, our results echoed the findings in pilot study in terms of a smaller amount of aspiration, comparable time to successful intubation and a higher operator ease score.
VL has been shown to improve laryngeal views and attain higher intubation success rates than traditional DL in studies involving predicted, simulated and genuine difficult airways. 15 As VLs come in with different designs and features, different VLs may have different performances. 10
In our study, we have demonstrated such differences exist among different VLs. GlideScope® in fact demonstrated a significantly longer intubation time than the C-MAC® for both the conventional and SALAD-1 techniques, and possibly significantly longer intubation time than the Airtraq® for the SALAD-2 technique.
The intrinsic differences in blade designs of different VLs may account for the results. GlideScope® has a hyper-angulated blade with a 60° curvature whereas the blade of the C-MAC® closely resembles a standard Macintosh blade. 16 The GlideScope® handle has to be tilted to a greater extent than the traditional Macintosh handle. 2 GlideScope® also requires the operator to insert the VL into the patient’s mouth along the midline with use of a specially designed stylet (which was provided to the participants in our study). 17 Despite prior standardized training provided to the participants, emergency doctors may be intuitively more familiar with the use of the C-MAC® as DL is the traditional method for intubation. In addition, a common problem was reported by the participants in using the GlideScope® was that despite the improved views, difficulty was encountered in sliding the ETT through the vocal cord. This issue was also reported in the literature.17 –19 The GlideScope® blade creates a sharp angle which may make the passage of the tube difficult. 18 Manoeuvring the tube and the stylet can help with the problem 2 at the possible expense of longer intubation time.
The C-MAC® achieved the shortest mean time numerically for successful intubation for the conventional and SALAD-1 techniques while the Airtraq® yielded a shorter mean time for the SALAD-2 technique. However, the differences were not statistically significant. The channelled design of the Airtraq® may be accountable for the SALAD-2 technique results. The Airtraq® has an anatomically shaped blade with a side channel where the ETT is ‘preloaded’. Once the vocal cord is visualized, the tube can be simply pushed along the channel. 2 In the SALAD-2 technique, the placement of a rigid suction catheter and diverting oesophageal intubation intrinsically limit the oropharyngeal space for intubation. The feature of the preloaded channel of the Airtraq® makes it more advantageous than other VL to for intubation with such technique. In addition, the relatively larger video monitor attached to the C-MAC® handle may be a hindrance especially in the crowded situation when using the SALAD-2 technique. The operator may take longer time to negotiate the ETT through the packed oral cavity. This may account for the significant longer time to use the C-MAC® to intubate with the SALAD-2 technique than with the conventional and SALAD-1 techniques. Despite the comparable performance of the C-MAC® and the Airtraq® in terms of intubation time, it is important to emphasize this relatively insignificant difference may not be totally irrelevant. Pieters et al. 3 pointed out that during intubation, ‘every second counts’ as the extra few seconds could result in oedema and trauma making future intubation attempts more difficult. Chan et al. 20 stated that a shorter intubation time could minimize risk of hypoxia during emergency intubations. Operators have to take this into consideration in choosing different VLs for intubation in different scenarios.
Multiple intubation attempts and failed ETI are associated with adverse outcomes such as cardiac arrhythmias, brain damage and mortality. 5 In our study, there was no significant difference in the number of attempts and ETI failure rate among different devices and different methods. The bulkier nature of the channelled VL may account for the insignificant number of failures with the Airtraq®. 15
Aspiration can result in aspiration pneumonia and is particularly a concern in airway management of patients with massive haematemesis. ETI using traditional DL with the conventional Yankauer suction catheter resulted in the largest amount of aspiration when compared with different VLs and different techniques. This finding concorded with our pilot study with the results that the rate of decontamination using the traditional technique was relatively limited. 10 For GlideScope®, there was significant less aspiration for both the SALAD-1 and SALAD-2 techniques than the conventional technique. No significant difference existed between the SALAD-1 and SALAD-2 techniques. Taking into consideration the significant shorter intubation time, the SALAD-1 technique is again the most favourable method for GlideScope® as illustrated in our pilot study. The C-MAC® yielded the least amount of aspiration for all the conventional, SALAD-1 and SALAD-2 techniques. However, this was not statistically significant.
The C-MAC® was the most preferred VL among the participants for the SALAD-1 technique. The mean score of the C-MAC® was also the highest for the conventional and SALAD-2 techniques although there was no statistical significance in the latter. The advantage of having a channel for loading the ETT may be offset by the bulkier nature of the Airtraq® in the conventional method, resulting in a significantly lower ease score than the C-MAC®. However, in the busy setting of the SALAD-2 technique, participants found it more difficult to use the C-MAC® for the SALAD-2 technique than the SALAD-1 possibly due to the reasons discussed earlier. Similar results were also shown for GlideScope® with the SALAD-2 technique rated as the most difficult probably for similar reasons.
In conclusion, the C-MAC® had comparable performance with the Airtraq® for the conventional, the SALAD-1 and SALAD-2 techniques in terms of intubation time. GlideScope® performed less well when compared with these two VLs. The C-MAC® was the most favourable VL for the SALAD-1 technique. However, there was no significant preference for different VLs in using the SALAD-2 technique. There was no significant difference in the number of attempts, failed ETI rate and amount of aspiration among different VLs in using both the SALAD-1 and SALAD-2 techniques. Different device requirements, device performance, individual preference and experience should be considered in choosing different laryngoscopes for different clinical situations.
Limitations
This study is a manikin study. As with other manikin studies, the demonstrated difference in performance may not be fully applicable to actual clinical scenarios. Manikins, such as the Nasco airway decontamination simulator in this study,9,10 can provide standardized conditions for evaluating the performance of different devices with different ETI methods. However, in daily clinical practice, other factors including the use of sedation and muscle relaxants, constant distractions and psychological stress 20 also pose obstacles in difficult airway management. Furthermore, intermittent pumping of the SAC in this study and the possible presence of food debris and blood clots clogging the suction catheter may make the real situation different from the study environment.
In this study, it is impossible to blind the investigators and participants. There is inevitably some potential for bias. Moreover, the Hawthorne effect 21 might affect the participants’ performance due to their awareness of being observed during ETI.
Carryover effect may possibly influence the results of this study. Previous intubation attempts may affect an individual’s performance in subsequent intubations. Randomization was done to minimize such effects. In addition, the VLs investigated in this study have different designs and different techniques are employed for ETI in different scenarios.
Another limitation was that only the conventional C-MAC® blade was used in this study. The C-MAC D-blade® is introduced to increase the potential to manage difficult airways and features a hyper-angulated tip. 22 As the Nasco airway decontamination simulator used in our study features an anatomically normal airway except for being able to simulate emesis, only the conventional blade was used with the C-MAC®. In a difficult airway manikin study comparing the conventional C-MAC® blade and D-blade®, the D-blade® yielded a better glottic view. 23 Given our results from GlideScope® which also features an angulated blade, there may be difference in ETI performance in using the D-blade® with the SALAD techniques when compared to the conventional C-MAC® blade. Further studies including the use of the C-MAC D-blade® are required to make the C-MAC® more comparative with the GlideScope®. In addition, difficult airway manikins simulating emesis may be useful to evaluate the performance of different VLs in subsequent studies.
Emergency doctors participated in this study have different levels of clinical experience in ETI and also different levels of skill in using different VLs. Although standardized training was provided for all participants, it is unavoidable that bias may be introduced as they may have different pre-existing levels of expertise in airway management. In addition, only emergency doctors were recruited in this study. This may limit the generalizability of the results. Further studies involving doctors from other specialties such as anaesthetists and intensivists are warranted.
Possible ETI complications such as dental injuries, airway and oropharyngeal trauma were not measured in this study. Dental injuries are a common complication in ETI. 24 In a simulator study, Nakanishi et al. 25 found that the use of the C-MAC® was associated with a higher maximum force applied on maxillary incisors during intubation attempt than DL and Airway Scope. In another manikin study, the GlideScope® resulted in significantly more dental injuries than the C-MAC® and the Airtraq®. 12 Complications with GlideScope® including perforation of the soft palate, palatopharyngeal arch and the palatoglossal arch have been reported. 2 Further evaluation of these complications is necessary before applying different devices and techniques on actual patients safely.
Finally, the sample size was calculated based on the differences of intubation time between the C-MAC®, the Airtraq® and the GlideScope® in a previous study. 12 As our study involved multiple comparisons of different VLs, a much larger sample size might be required to evaluate the difference in their performance in using the SALAD techniques.
Conclusion
The SALAD technique is potentially useful to facilitate ETI in patients with massive haematemesis.9,10 We have demonstrated that VL was a better alternative to conventional DL in such scenarios. Different VLs had varied performance in performing the SALAD techniques. The C-MAC® and the Airtraq® were better choices than the GlideScope® with shorter intubation time. Participants found that the C-MAC® is the easiest to use for the SALAD-1 techniques. The number of attempts, failed ETI rate and amount of aspiration were similar for different VLs. Further studies and clinical evaluation are necessary to validate the different performance of VL in ETI of real patients using the SALAD techniques.
Footnotes
Acknowledgements
The authors thank all the emergency doctors for participating in this study and Mr Lee Wing Chung, Secretary of Accident and Emergency Department, North Lantau Hospital for clerical support.
Author contributions
C.H.K.W., S.K. and O.F.W. developed the study concept and designed the study. C.H.K.W. conducted the study. C.H.K.W., S.K. and O.F.W. analysed the data. C.H.K.W. drafted the manuscript. S.K., O.F.W., H.M.M., C.H.A.L. and Y.N.S. revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
All participants’ identifications were removed before storage. The master data set was kept by the investigators in the computer and was password protected. Access to the data would be limited to the investigators and Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact the corresponding author for further information of data if required.
Informed consent
Written consent was obtained from the participants for their anonymized information to be published in this article.
Ethical approval
This study was approved by the Clinical Research Ethics Committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.