
Abstract
Objective
To determine whether intubation education using the Pentax Airway Scope (AWS) in normal airways is more useful than direct laryngoscopy (Macintosh laryngoscope) in novice personnel.
Methods
Eleven intern doctors without intubation experience performed 60 sequential intubations with each device on a manikin and 10 sequential intubations in adult patients. The time required for successful intubation, percentage of glottic opening (POGO) score, number of intubation attempts, and number of dental injuries were analyzed for each intubation technique.
Results
The mean (standard deviation) time required for successful intubation decreased as the number of intubations increased and was significantly shorter with the Pentax AWS than direct laryngoscope [22.6 (7.3) vs. 29.6 (10.0) and 33.0 (8.0) vs. 44.7 (5.6) s, respectively] in both the manikin and clinical studies. The Pentax AWS was also associated with higher POGO scores than the direct laryngoscope [81.7 (8.9) vs. 55.1 (13.2) and 80.9 (9.7) vs. 49.6 (16.5), respectively] and fewer intubation attempts. Fewer dental injuries occurred with the Pentax AWS in the manikin study.
Conclusions
Novices performed intubation more rapidly and easily with an improved laryngeal view using the Pentax AWS. We suggest that intubation education with video laryngoscopy should be mandatory along with direct laryngoscope training.
Keywords
Introduction
Endotracheal intubation is an essential technique for adequate ventilation via maintenance of airway patency. Although the use of direct laryngoscopy is a fundamental method for endotracheal intubation, this technique is regarded as a difficult procedure with a high failure rate; in fact, the initial success rate reportedly ranges from 51% to 65%.1–3 Because repeated laryngoscopic attempts and errant intubations are associated with morbidity and mortality due to hypoxemia, aspiration, and cardiac arrest,4,5 intubation can be a stressful situation for even well-trained medical staff. Therefore, many devices have been developed for easy and simple intubation with high success rates. The Pentax Airway Scope (AWS) (Pentax Corporation, Tokyo, Japan) is an advanced device that implements a video-assisted technique. Since the first clinical application of the Pentax AWS was introduced in 2006, the advantages of this device have been reported in the clinical setting, including an improved laryngeal view, reduced intubation time, and increased success rate.6–10 In addition, unlike other video-assisted laryngoscopes, such as the GlideScope (Verathon, Bothell, WA, USA),11,12 locating the tube tip is more convenient using the Pentax AWS because the target symbol on the screen and Pentax introducer (Intlock blade) are used to guide the loaded endotracheal tube toward the trachea. 6 Thus, technical mastery of endotracheal intubation might be more easily achieved with the Pentax AWS than with direct laryngoscopy.
Nevertheless, direct laryngoscopy tends to be used for the education of endotracheal intubation. The reason for this seems to be the limited supply of video-assisted laryngoscopes because of their high cost. 13 Additionally, experienced medical staff members often prefer to use direct laryngoscopy because they were originally trained using this method. However, many novel laryngoscopes have since been developed, and establishment of better intubation techniques for novices is imperative. Although several comparative studies of intubation with the Pentax AWS versus direct laryngoscopes by novices have been conducted using manikins,9,14–16 few such clinical studies have been reported.17,18 Thus, we designed this prospective randomized controlled trial to evaluate the effectiveness of each laryngoscope and determine the differences in technical mastery of intubation by novice personnel when learning with a direct laryngoscope versus the Pentax AWS. The main purpose of this study was to determine the relative efficacy of the Pentax AWS versus a direct laryngoscope by evaluating the successful intubation time and percentage of glottic opening (POGO) score in novice personnel. Additionally, we sought to determine whether intubation education with the Pentax AWS would be useful for novices and whether the results of a manikin study would be consistent with those of a clinical study.
Patients and methods
This study was conducted at Hanyang University Hospital, Seoul, Korea. After approval by the institutional review board of Hanyang University Hospital, this study was registered at http://cris.nih.go.kr (Clinical Research Information Service, registration number: KCT0001334). Novice personnel and adult patients requiring general anesthesia were included in this randomized controlled trial following obtainment of written informed consent. We defined novices as intern doctors who had no intubation experience before the study. All intern doctors were severely restricted from performing intubations in other medical situations during the study period.
Each intern received standardized training by an anesthesiologist (K.N.K.). This training included oral instructions about the use of each device and demonstrations of the each intubation technique. Thereafter, each participant performed one practice intubation with each device. This study included two groups: a Macintosh laryngoscope with a size 3 blade was used in the M group, and the Pentax AWS was used with the Pentax introducer (Intlock blade) in the P group. First, each intern performed intubation using each device on a manikin (manikin study). Intubations were then performed in patients requiring general anesthesia (clinical study).
Manikin study
Each novice performed 60 intubations with each device. The number of implementations was limited to 10 per day in each group, and the sequence of procedures was determined by opening sealed envelopes immediately before performing the intubation. These envelopes contained a value from 1 to 20, and one of the authors (K.N.K.) randomly assigned the participants into two groups using the random number generator of the Excel program. There was a 3-minute break between each procedure. Intubation was performed using a Laerdal Airway Management Trainer (Laerdal Medial, Stavanger, Norway) with an intraluminal 7.5-mm cuffed endotracheal tube (ET). The ET was lubricated before every intubation attempt.
The primary endpoints were the duration of time required for successful intubation and the POGO score. The time required for successful intubation was defined as the time taken from insertion of the blade tip between the teeth to verification of the location of the ET by confirming the presence of bilateral lung inflation. The POGO score, which is considered to be a better parameter for assessing the difference between intubation techniques, was defined as the percentage of visualized glottis. 19 The POGO score ranged from 0% (no glottis can be seen) to 100% (the entire glottis can be seen between the anterior commissure of the vocal cords and the interarytenoid notch). Additional endpoints were the number of intubation attempts, the rate of successful intubation, and the number of dental injuries. Dental injuries were measured by the number of audible teeth clicks, and failure of intubation was defined as a ≥90-second duration of attempted intubation or more than four intubation attempts. All data were obtained at the 1st, 10th, 20th, 30th, 40th, 50th, and 60th procedures. The POGO scores were recorded as presented by each participant, and the other data were measured by one of the authors.
Clinical study
After the manikin study, the clinical study was conducted on adult patients aged 20 to 65 years requiring general anesthesia. Patients were excluded if they met the following criteria: (1) American Society of Anesthesiologists physical status of III or IV, (2) damaged teeth and predicted dental trauma, (3) a history of previous difficult intubation or cervical spine instability, (4) body mass index of >30 kg/m2, (5) Mallampati classification of III or IV, (6) thyromental distance of <7 cm, (7) cervical movement of <45º, and (8) mouth opening of <3 cm. The Mallampati classification, thyromental distance, cervical movement, and mouth opening were measured on the day before surgery.
Each intern performed 10 intubations with each device. The number of implementations was limited to two times per day to prevent excessive acquisition of the intubation technique by repetition. The sequence of the procedures was allocated by opening the sealed envelopes before monitoring the patients. These envelopes contained a value from 1 to 4 indicating the intubation order and the name of the group that one of the authors (K.N.K.) had randomly assigned using the random number generator of the Excel program.
General anesthesia was conducted using the same predefined protocol without premedication. After spontaneous ventilation was performed for 3 minutes with a fraction of inspired oxygen of 1.0 to ensure oxygenation, anesthesia was induced with propofol at 1.5 mg/kg, rocuronium at 0.6 mg/kg, and remifentanil at 0.1 µg/kg/min. After manual ventilation for 3 minutes with an oxygen flow of 8 L/min and sevoflurane at 3.0 vol%, intubation was performed. Procedures such as the backward, upward, rightward pressure maneuver around the cricoid cartilage were not applied.
In both groups, the size of the ET was adjusted according to the patient (internal diameter of 7.5 and 7.0 mm for men and women, respectively). If the intubation attempt failed, the patients received manual ventilation with 8 L/min of oxygen until the next intubation attempt to ensure adequate oxygenation. All of these procedures were conducted under the supervision of a staff anesthesiologist (K.N.K. or M.A.J.). When risks such as severe dental injuries were predicted, the procedures were interrupted immediately.
The primary endpoints were the duration of time required for successful intubation and the POGO score. The time required for successful intubation was the time from insertion of the blade tip between the teeth to verification of the location of the ET by confirming the end-tidal carbon dioxide. Additional endpoints were the number of intubation attempts, number of dental injuries, rate of successful intubation, hemodynamic changes during the intubation period, and incidence of postoperative hoarseness and sore throat. Dental injuries were defined as any notable injuries to the teeth, lip, tongue, or mouth according to the patient’s postoperative report. The blood pressure and heart rate were recorded at the following times: (1) before the induction of anesthesia, (2) immediately before intubation, (3) 1 minute after intubation, and (4) 5 minutes after intubation. Patients were evaluated for postoperative hoarseness and sore throat in the postanesthesia care unit. POGO scores were recorded as presented by each intern. Another anesthesiologist who was blinded to the group assignment recorded the hemodynamic change and occurrence of postoperative hoarseness and sore throat.
Justification of sample size and statistical analysis
In the manikin study, 11 interns performed 60 intubations with each device based on reports that the intubation success rate reaches around 90% after 56 performances. 20 In the clinical study, the duration of intubation with the Macintosh laryngoscope was 71 s with a standard deviation of 44 s according to a previous study. 17 We considered 20 s to be a meaningful difference, and the calculated sample size was 103 patients in each group with an assumed α error of 5% and ß error of 10%. Accounting for a dropout rate of 5%, 110 patients were allocated to each group.
Categorical data are expressed as the number of patients (percentage as appropriate) and were compared using Pearson’s chi-square test or Fisher’s exact test. Continuous data are expressed as mean (standard deviation). After a p value of <0.05 was obtained in the Shapiro-Wilk test for normality, continuous data were compared using Student’s t-test. The differences in the time required for successful intubation and the POGO score were compared between the two groups using repeated-measures analysis of variance. Intergroup differences were analyzed using the paired t-test, and p values were adjusted with Bonferroni’s correction. Statistical analysis was performed with SPSS software (version 21.0; IBM Corp., Armonk, NY, USA). A p value of <0.05 was considered statistically significant.
Results
Originally 19 interns were enrolled in this study. However, eight were excluded because of previous intubation experience. Among 298 patients who were assessed for eligibility, 67 patients did not meet inclusion criteria and 11 declined to participate in the study from October 2014 until May 2015. As a result, 220 patients were randomized by opening sealed envelopes which contained randomly assigned groups using a random number generator in the Excel program by author. All these 220 patients were included in analysis without follow-up loss (Figure 1). Patient demographic data and preoperative assessment of airways are summarized in Table 1. There were no differences in patient characteristics between the two groups.

Flow diagram of patient recruitment and reasons for exclusion from the clinical study. M group, intubation with Macintosh blade laryngoscope; P group, intubation with Pentax Airway Scope.
Patients’ demographic data and preoperative assessment of airway characteristics

Data are presented as number of patients (%), median (range), or mean (standard deviation).
There were no significant differences in patient characteristics between the two groups.
M group, intubation with Macintosh blade laryngoscope; P group, intubation with Pentax Airway Scope; ASA, American Society of Anesthesiologists.
Manikin study
The mean (standard deviation) duration required for successful intubation in the P and M groups was 22.6 (7.3) s and 29.6 (10.0) s, respectively. This duration of time was significantly shorter in the P group (p < 0.001) and decreased as the number of intubations increased (p < 0.001) (Figure 2(a)). The POGO scores increased as the number of intubations increased (p = 0.03), and higher POGO scores were observed in the P group than in the M group [81.7 (8.9) vs. 55.1 (13.2), respectively; p < 0.001] (Figure 2(b)). No difference was found in the rate of successful intubation, but an increased number of intubation attempts (p = 0.002) and dental injuries (p < 0.001) were observed in the M group (Table 2).
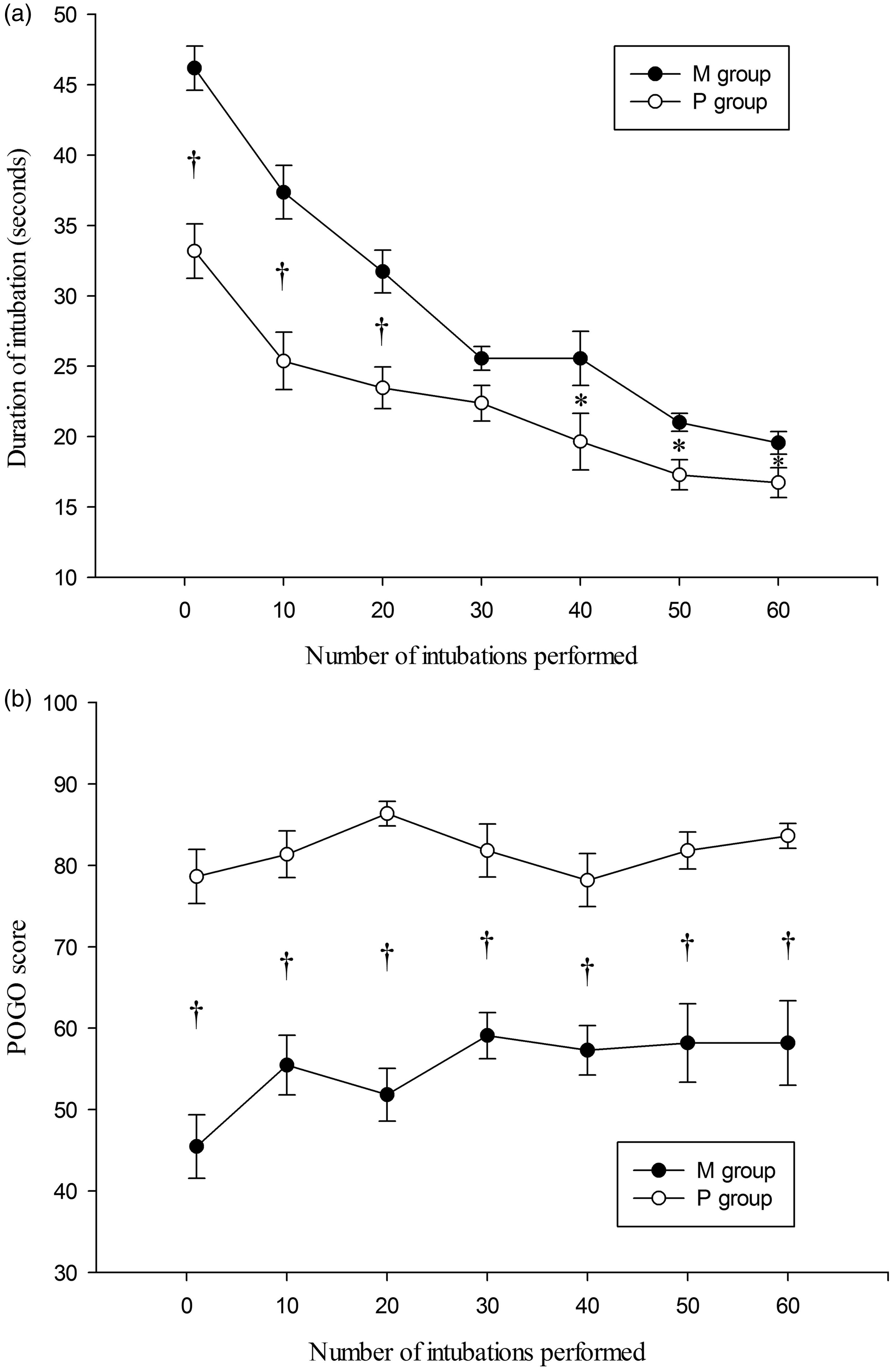
Results of the manikin study for each intubation attempt. (a) Duration of intubation. (b) POGO score. All data were obtained at the 1st, 10th, 20th, 30th, 40th, 50th, and 60th procedure. All data are presented as mean and standard error.
Comparison of variables between groups in manikin and clinical studies

Data are presented as n (%).
In the manikin study, each novice participant performed 60 intubations, and data were obtained at the 1st, 10th, 20th, 30th, 40th, 50th, and 60th procedures.
M group, intubation with Macintosh blade laryngoscope; P group, intubation with Pentax Airway Scope.
Clinical study
Similar to the results of the manikin study, the time required for successful intubation in the P group was significantly shorter than that in the M group [33.0 (8.0) s vs. 44.7 (5.6) s, respectively; p < 0.001] and decreased as the number of intubations increased (p = 0.03) (Figure 3(a)). Although there was no difference in the POGO score according to the number of intubations, the P group had higher POGO scores than the M group [80.9 (9.7) vs. 49.6 (16.5), respectively; p < 0.001] (Figure 3(b)). The number of intubation attempts in the M group was higher than that in the P group (p = 0.001), but the intubation success rates did not differ. No dental injuries occurred, and there were no differences in postoperative hoarseness or sore throat between the two groups (Table 2). We observed a lower mean arterial pressure in the P than M group at 1 minute after intubation (p = 0.03) and 5 minutes after intubation (p = 0.03) (Table 3). Although a lower mean arterial pressure was found, the small change (5-mmHg decrease in the mean arterial pressure) indicated that the clinical significance of this decrease is low.
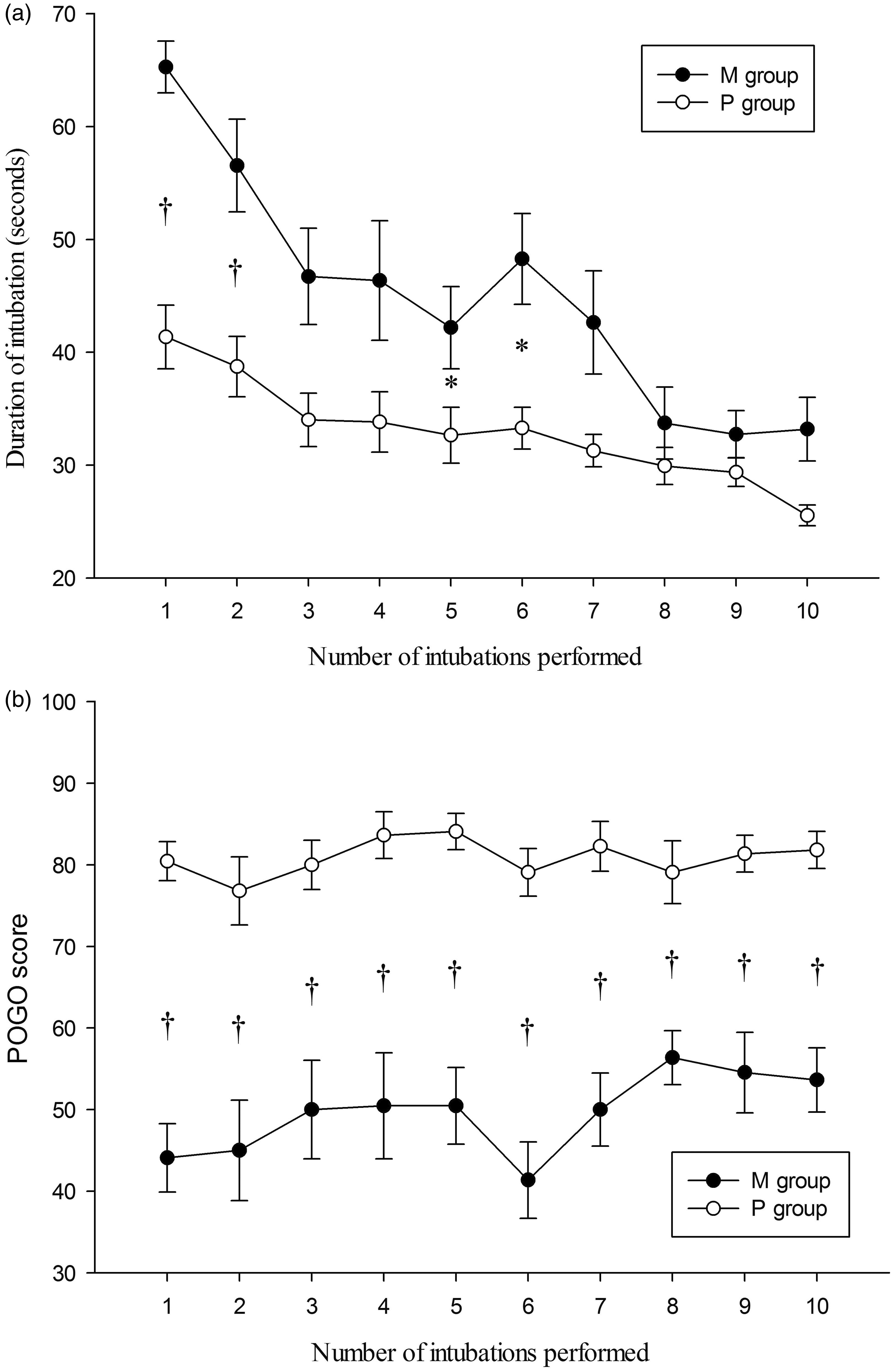
Results of the clinical study for each intubation attempt. (a) Duration of intubation. (b) POGO score. All data are presented as mean and standard error.
Hemodynamic changes during intubation

Data are presented as mean (standard deviation).
M group, intubation with Macintosh blade laryngoscope; P group, intubation with Pentax Airway Scope.
Discussion
This prospective randomized controlled trial demonstrated that novices perform intubation more rapidly with an improved laryngeal view and a fewer number of attempts using the Pentax AWS in both manikin and clinical studies. The results of a previous study involving novices were consistent with ours in terms of the improved laryngeal view and shorter intubation time. 17 Additionally, our study revealed that technical mastery of intubation was easier with the Pentax AWS than the direct laryngoscope. In our study, the novices performed sequential intubations to assess mastery of the intubation technique in accordance with repetition. As a result, although the time interval between the two laryngoscopic techniques decreased as the number of intubations increased, consistently and significantly shorter intubation times after the first attempt and fewer intubation attempts in the P group imply that the intubation technique was more easily mastered using the Pentax AWS (Figure 2(a), 3(a)). After taking all of these findings into consideration, we conclude that intubation using the Pentax AWS is faster and easier than that using direct laryngoscopy for novices.
There are several possible reasons for this result. First, the Pentax Intlock blade was designed to fit the anatomical shape of the oropharyngeal region and obtain a sufficient view for endotracheal intubation with minimal neck extension.6,21 Compared with Macintosh laryngoscopy, the Pentax AWS decreased the cervical spine movement by more than 37% and atlanto-occipital distance movement by 42% on radiography. 22 In contrast, alignment of the oral, tracheal, and pharyngeal axes is required for correct positioning during tracheal intubation with direct laryngoscopy. Novices generally had difficulty with this process. In addition, exposure of the tongue was far easier using the Pentax AWS than direct laryngoscopy in our clinical study. This is because the Pentax AWS blade was inserted just along the tongue to locate the tip of the Pentax AWS beneath the epiglottis. 6
Another reason for our study result is the superior laryngeal view of the Pentax AWS. The improved laryngeal view of the Pentax AWS compared with direct laryngoscopy is the most prominent feature of the Pentax AWS regardless of study designs, such as manikin studies8,9 or studies using the normal airway, 23 difficult airway,24–26 or cervical spine immobilization.7,27,28 The fact that the lowest POGO score in the M group was obtained simultaneously with a significantly increased duration of intubation on the sixth attempt in our clinical study indicates that failure to obtain a sufficient laryngeal view impedes intubation (Figure 3).
Despite these advantages of the Pentax AWS, the use of video-assisted laryngoscopy is recommended only when adequate facemask ventilation is possible and the first attempt to intubate with direct laryngoscopy is unsuccessful according to practice guidelines for the management of difficult airways. 29 Fortunately, in the 2013 American Society of Anesthesiologists difficult airway algorithm, the initial approach of video-assisted laryngoscopy for intubation is introduced after consideration of the relative clinical merits and feasibility. 30 An unexpected difficult airway is correlated with morbidity and mortality, 31 and repeated laryngoscopic attempts aggravate this situation.4,5 In addition, when anesthesiologists proceeded to manage an unexpected difficult airway in the operation room, persistent use of direct laryngoscopy after a failed first attempt has a success rate of only 22%, and this rate increases if the anesthesiologists have an alternative method of advanced airway management. 32 Therefore, considering the merits of the Pentax AWS in patients with difficult airways25,26 and the easier technical mastery of intubation in our study, it is fairly reasonable that the Pentax AWS can replace direct laryngoscopy when management of a difficult airway is expected.
A meta-analysis of prehospital airway techniques demonstrated relatively low success rates of endotracheal intubation (86.3%) in prehospital emergency situations. 33 In addition, cervical spine trauma occurred in 2.4% to 3.5% of blunt traumas,34–36 and the corresponding mortality rate ranged from 5% to 6%.36,37 Stabilization of the neck during intubation may be needed to avoid more damage to the cervical spine. In such cases, use of the Pentax AWS can be a good alternative because of the aforementioned reduction in cervical spine movement. Many clinical studies have already revealed an improved glottis view, a higher success rate of intubation, and a shorter intubation time in patients with cervical spine immobilization.7,27,28,38 Nevertheless, although video-assisted laryngoscopes have started to be introduced in the prehospital setting, 39 they have not been used as an alternative airway device in prehospital emergency care except for a few cases.40–42 Considering the advantages of the Pentax AWS such as its ease of learning, improved laryngeal view, and increased safety for patients with cervical injury, education and practical use of the Pentax AWS should be conducted in the early stages of intubation training not only in hospital physicians, but in all emergency medical staff who may be presented with the opportunity to perform advanced airway management in a prehospital setting.
Our study has a few limitations. First, before the clinical study, 60 intubations were performed in the manikin study to avoid complications of unskilled intubation performed by novices. In actuality, the manikin study was designed because the institutional review board suggested it as a mechanism to ensure patient safety. Through the manikin study, the novices had an opportunity to learn the intubation technique, and the intubation duration indeed decreased as the number of intubations performed increased (Figure 2(a)). Hence, it may not be accurate to define these intern doctors, with experience involving 60 intubations in manikins, as novices. However, considering the similar results in both the manikin and clinical studies, such as the significant difference in the intubation duration between the early and later intubation attempts, our conclusion regarding the effectiveness of the Pentax AWS is still reasonable.
A second limitation is that we were unable to blind the investigators to the laryngoscopy device used. With the exception of dental injuries, hemodynamic changes, and postoperative hoarseness and sore throat, the data could not be collected in a blinded fashion in this study. However, the lack of blinding did not seem to be a serious problem because the endpoints were clearly defined, including the duration of time required for successful intubation, number of intubation attempts, and rate of successful intubation. The POGO scores were simply recorded as presented by each intern doctor to remove the intention of the authors. Because participating interns did not know the purpose of this study, there was no potential for bias.
Finally, this study included only patients with a normal airway following preoperative airway assessment. This is why our rate of successful intubation was 100% in contrast to the results from a previous study showing that 57 intubation attempts were necessary to achieve a success rate of 90%. 20 Moreover, our rate of technical mastery of intubation may be exaggerated because of the relative ease of intubation. Assessing the effect of laryngoscopy performed by novices in patients with difficult airways is still an important issue. Although reduced difficulty of tracheal intubation with the Pentax AWS has been reported in several studies,24,26 no studies have compared the Pentax AWS and direct laryngoscopy performed by novices in patients with difficult airways. Therefore, well-controlled randomized studies that compare the effectiveness of the Pentax AWS versus direct laryngoscopy performed by novices in patients with difficult airways are needed.
Conclusions
Novices performed intubation more rapidly with an improved laryngeal view using the Pentax AWS. Additionally, compared with the direct laryngoscope, mastery of the intubation technique was easier using the Pentax-AWS than direct laryngoscope in patients with a normal airway. Therefore, although training in direct laryngoscopy must still be the primary technique, we suggest the mandatory inclusion of intubation education with a video laryngoscope such as the Pentax AWS in addition to direct laryngoscope training.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.