
Abstract
Introduction:
Minor head traumas constitute a significant part of childhood injuries. The incidence of intracranial pathologies in children with minor head trauma varies in the range of 3%–5%, but it is higher among younger infants. The criteria of the Pediatric Emergency Care Applied Research Network, Canadian Assessment of Tomography for Childhood Head Injury, and Children’s Head Injury Algorithm for the Prediction of Important Clinical Events are the most frequently accepted clinical decision-making criteria that were developed for selective computerized tomography requests. This study was conducted to assess the diagnostic performances of the Pediatric Emergency Care Applied Research Network, Canadian Assessment of Tomography for Childhood Head Injury, and Children’s Head Injury Algorithm for the Prediction of Important Clinical Events criteria in Turkish society, determine their validity, and find the most suitable algorithm for cranial imaging in children with minor head trauma.
Methods:
This study retrospectively examined the data of patients under the age of 18 years who were admitted to the Emergency Medicine Department of Uludağ University Medical Faculty due to minor head trauma; 530 patients were included as they complied with the criteria. The exclusion criteria were being any trauma patients above the age of 18 years, Glasgow Coma Scale <13, pregnant patients, hemorrhagic diathesis, using anticoagulants, patients with penetrant trauma, patients with priorly known brain tumor, and patients with neurological diseases. The patients were divided into group based on the Pediatric Emergency Care Applied Research Network, Canadian Assessment of Tomography for Childhood Head Injury, and Children’s Head Injury Algorithm for the Prediction of Important Clinical Events Criteria.
Results:
Among all patients, 37.40% were female and 62.60% were male. Abnormal computed tomography findings such as epidural bleeding, subdural bleeding, and skull fractures were detected in 44 of the patients. The sensitivity of the Pediatric Emergency Care Applied Research Network criteria was 72.4%, the specificity was 54.5%, the sensitivity of the Canadian Assessment of Tomography for Childhood Head Injury criteria was 57.8%, the specificity was 50%, the sensitivity of the Children’s Head Injury Algorithm for the Prediction of Important Clinical Events criteria was 87.7%, and the specificity was 20%.
Conclusion:
Given the populations to which the rules apply, it is understood that the Children’s Head Injury Algorithm for the Prediction of Important Clinical Events criteria is more determinative in detecting pathological computed tomography outcomes compared to Pediatric Emergency Care Applied Research Network and Canadian Assessment of Tomography for Childhood Head Injury.
Introduction
Minor head traumas (MHTs) constitute a significant part of childhood injuries.1,2 While trauma mechanisms may vary, especially falling from a height is encountered very frequently under 2 years of age. The incidence of intracranial pathologies in children with MHT varies in the range of 3%–5%, but it is higher among younger infants.3–7 However, these pathologies rarely require surgical intervention, and appropriate management of these patients is still an issue that is under debate.7–9
Computerized brain tomography (CBT) has become the gold standard in detecting intracranial injuries in patients who are admitted with MHT, but its prevalent and unnecessary usage leads to increases in medical costs. 10 The criteria of the Pediatric Emergency Care Applied Research Network (PECARN), Canadian Assessment of Tomography for Childhood Head Injury (CATCH), and Children’s Head Injury Algorithm for the Prediction of Important Clinical Events (CHALICE) are the most frequently accepted clinical decision-making criteria that were developed for selective computed tomography (CT) requests. 11
This study compared the PECARN, CATCH, and CHALICE criteria, which are three recent algorithms that are used in clinical decision-making in children with MHT to avoid unnecessary exposure to radiation. The objective was to assess the diagnostic performances of the PECARN, CATCH, and CHALICE criteria in Turkish society; determine their validity; and find the most suitable algorithm for cranial imaging in children with MHT.
Methods
This study retrospectively examined the data of patients under the age of 18 years who were admitted to the Emergency Medicine Department of Uludag University Medical Faculty due to MHT (Glasgow Coma Scale [GCS] ⩾ 13) between the dates of 02 January 2014 and 12 December 2017 and subjected to CBT imaging. The ethical approval was taken from Ethical Committee of the University. The data were obtained through the patient’s files and the hospital’s automation system. A total of 3248 patients were screened retrospectively during this study and 530 of them were included as they complied with the criteria. These criteria were MHT patients younger than 18, GCS ⩾ 13, and MHT patients younger than 18 with blunt head trauma.
The exclusion criteria were being any trauma patients above the age of 18 years, GCS < 13, pregnant patients, hemorrhagic diathesis, using anticoagulants, patients with penetrant trauma, patients with priorly known brain tumor, and patients with neurological diseases.
Using the patient files on the patients who were included in the study and the hospital’s automation system, information was collected on age, sex, loss of consciousness, headache, vomiting, abnormal behaviors toward parents, amnesia, episodes, concerns of non-accident trauma, trauma mechanism, abnormal mental state, cranial fracture findings, GCS, neurological deficit, monitoring, and CBT results in the patients. Abnormal CBT findings such as epidural bleeding, subdural bleeding, and all types of skull fractures were recorded as one group named “abnormal CT” group. The patients were divided into groups based on the PECARN, CATCH, and CHALICE criteria.
Data analysis
The data of the study were analyzed by using SPSS 23.00. Kolmogorov–Smirnov test was used to test the normal distribution of the continuous variables. The descriptive statistics for the continuous variables are presented in the form of mean ± standard deviation. The categorical variables as shown as frequency of cases (n) and percentage (%). Student’s t-test was used to examine the significance of the differences between the mean values of the groups. The categorical variables were analyzed by McNemar test or Fisher’s Exact test. Moreover, sensitivity, specificity, positive, and negative predicted values were calculated for all three sets of rules. All results were assessed in a 95% confidence interval and 5% level of significance. A sample size of 500 pairs achieves 80% power to detect an odds ratio of 2 using a two-sided McNemar test with a significance level of 0.05.
Results
The mean age of the patients who were included was 5.89 ± 4.89. Among all patients, 37.40% were female and 62.60% were male. Male/female ratio in our study was 1.67:1.
The mean age of the female children was 5.94 ± 5.29 years, while the male children had a mean age of 5.86 ± 4.64 years; 28.49% of the patients were under the age of 2 years. There was no difference in gender ratio among different age groups (p = 0.8556).
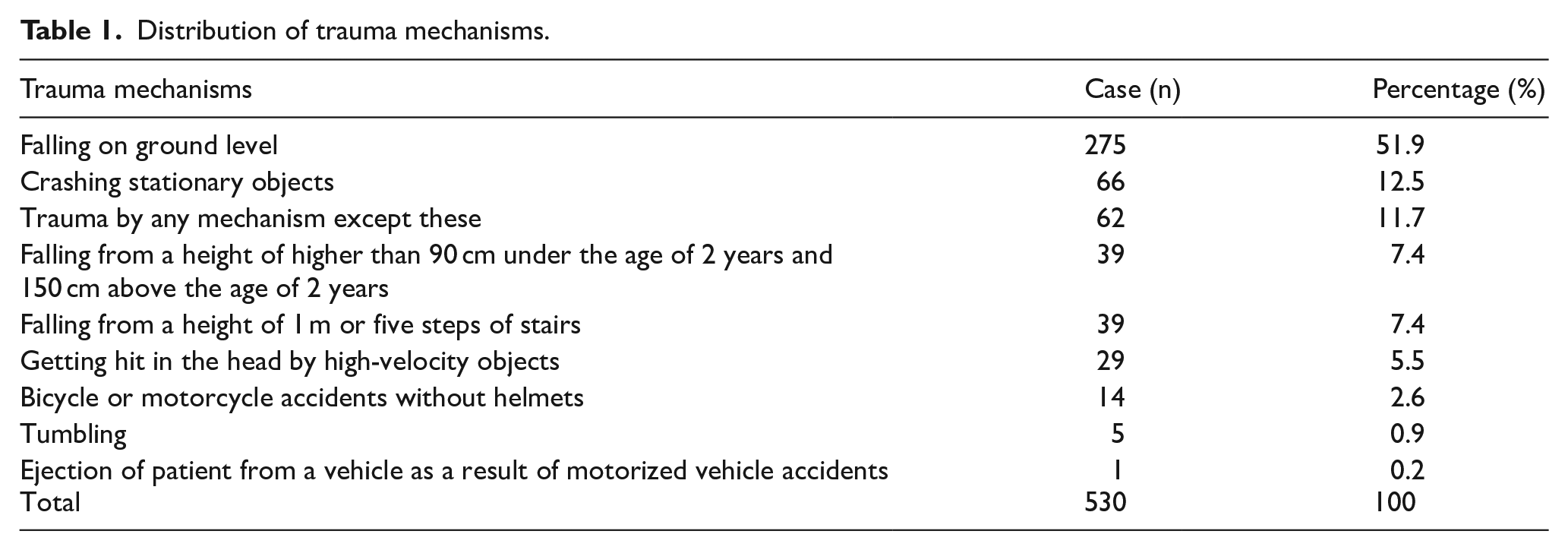
Table 1 shows the children’s distribution based on their trauma mechanisms.
Distribution of trauma mechanisms.
The GCS was 14 in 1.1% of all patients, while it was 15 in 98.9%. There were abnormal findings in the CBT results of 8.3% of the cases. The CBT results were abnormal among 33.3% of the patients with GCS = 14% and 8% of the patients with GCS = 15. In addition to this, the CBT results did not significantly differ based on GCS (p > 0.05). The results are presented in Table 2.
Distribution of CBT results based on GCS.
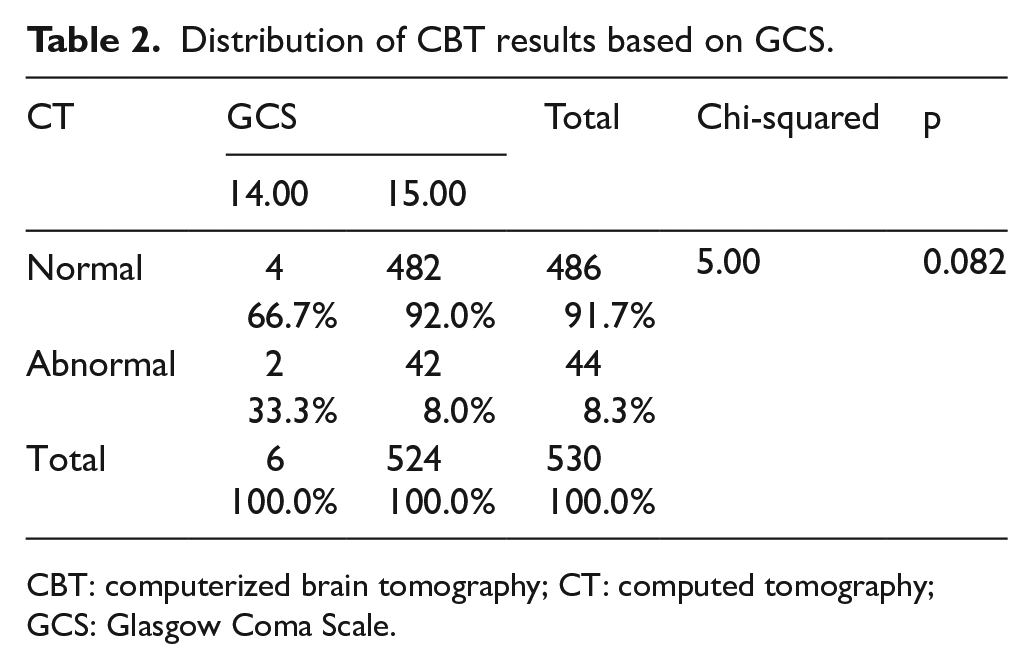
CBT: computerized brain tomography; CT: computed tomography; GCS: Glasgow Coma Scale.
The patients were examined under four groups including those where the PECARN rules could be applied, those where the CATCH rules could be applied, those where the CHALICE rules could be applied, and those named as “Other” where none of the 3 sets of rules could be applied. Among all patients, 29.8% were in the PECARN group, 31.9% were in the CATCH group, and 13% were in the CHALICE group, while there were also patients on whom two or three sets of rules were applicable.
The mean age was calculated as 6.72 ± 5.18 years in the PECARN group, 5.65 ± 5.04 years in the CATCH group, 5.17 ± 4.33 years in the CHALICE group, and 5.97 ± 4.88 years in the other group.
In the PECARN group, 57.6% were male, and 43.4% were female, while these values were, respectively, 60.4% and 39.6% in the CATCH group, 65.2% and 34.8% in the CHALICE group, and 64.4% and 35.6% in the other group. The intergroup distributions based on patient anamneses are shown in Table 3.
Distributions based on patient anamneses.
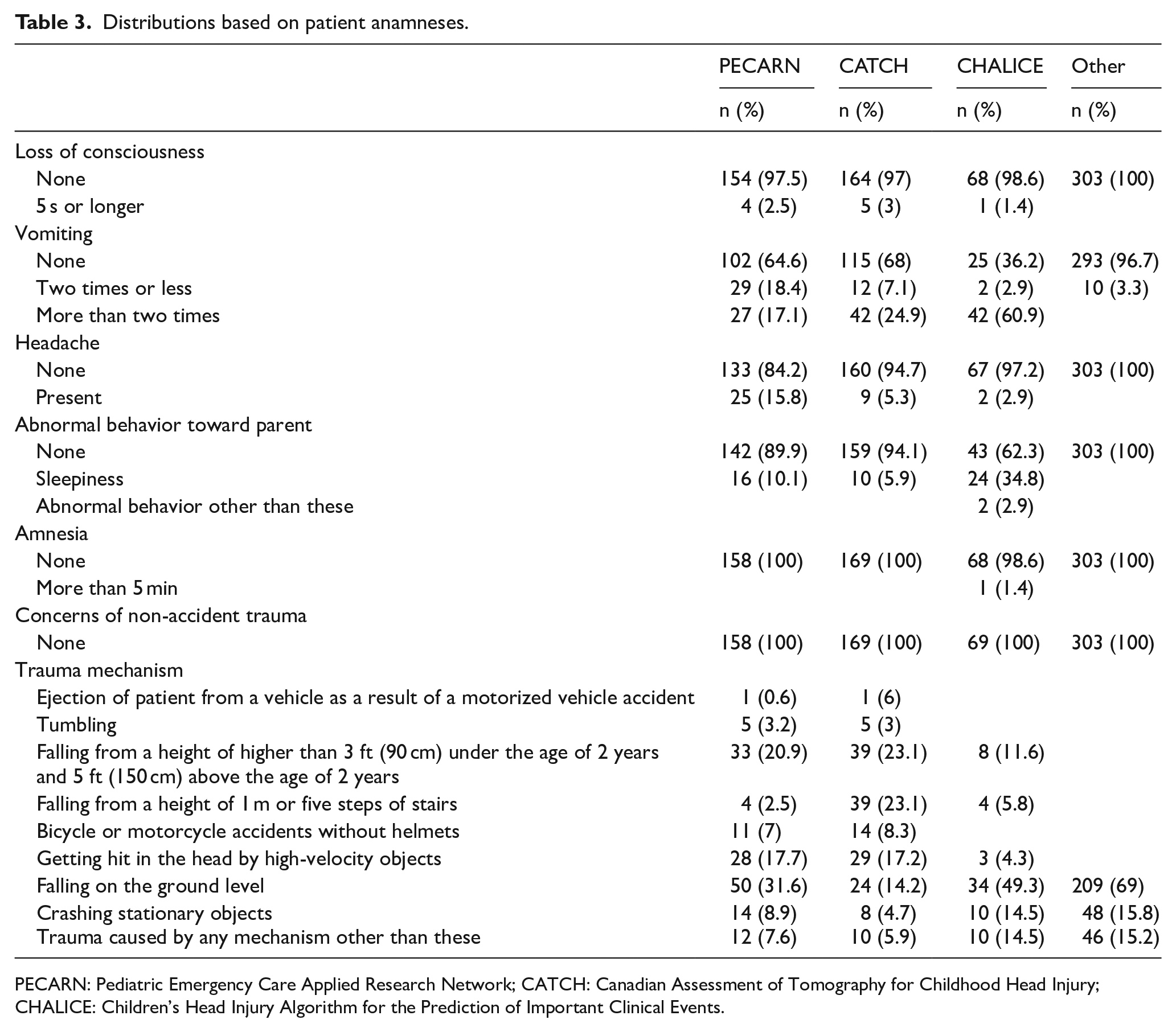
PECARN: Pediatric Emergency Care Applied Research Network; CATCH: Canadian Assessment of Tomography for Childhood Head Injury; CHALICE: Children’s Head Injury Algorithm for the Prediction of Important Clinical Events.
Distributions of the patients based on the results of their physical examinations are shown in Table 4.
Distributions based on the results of physical examinations.

PECARN: Pediatric Emergency Care Applied Research Network; CATCH: Canadian Assessment of Tomography for Childhood Head Injury; CHALICE: Children’s Head Injury Algorithm for the Prediction of Important Clinical Events; GCS: Glascow Coma Scale.
There were abnormal CBT findings in 15.2% of the patients in the PECARN group, 13% in the CATCH group, 13% in the CHALICE group, and 5% in the group of patients on whom none of these rules were applicable. The distribution of CBT results based on the groups is shown in Table 5. There was a significant difference between PECARN groups (p < 0.001), CATCH groups (p = 0.012), but not for CHALICE groups (p = 0.195) in terms of CT results (Table 5).
Distribution of CBT results based on groups.
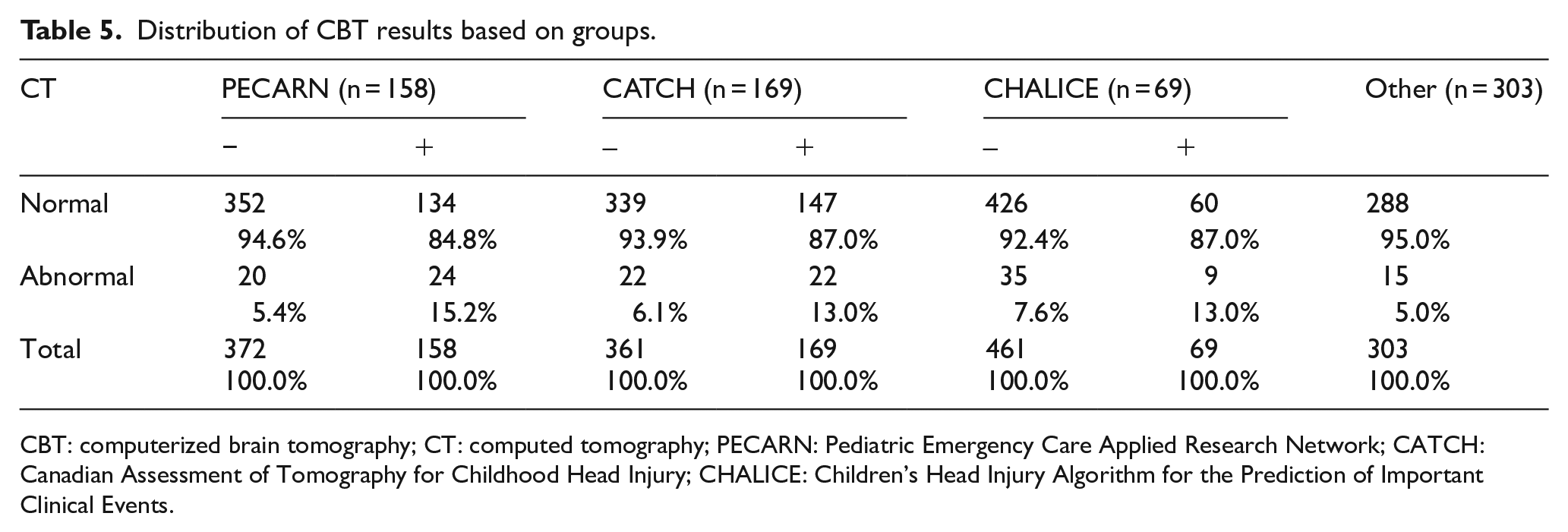
CBT: computerized brain tomography; CT: computed tomography; PECARN: Pediatric Emergency Care Applied Research Network; CATCH: Canadian Assessment of Tomography for Childhood Head Injury; CHALICE: Children’s Head Injury Algorithm for the Prediction of Important Clinical Events.
In the patient group where the PECARN rule was applicable, the rule had a sensitivity of 72.4%, specificity of 54.5%, positive predicted value of 15.2%, and negative predicted value of 5.4%. In the patient group where the CATCH rule was applicable, the rule had a sensitivity of 57.8%, specificity of 50%, positive predicted value of 13%, and negative predicted value of 6.1%. In the patient group where the CHALICE rule was applicable, the rule had a sensitivity of 87.7%, specificity of 20%, positive predicted value of 13%, and negative predicted value of 12.4%. In the patient group where all three sets of rules were applicable, the PECARN, CATCH, and CHALICE rules had a compound sensitivity of 94.2%, specificity of 13.6%, positive predicted value of 17.6%, and negative predicted value of 7.7%.
Among the patients, 6.8% were referred to a service, 0.2% were hospitalized in the intensive care unit, 0.2% were referred to external centers, and 92.8% were discharged with recommendations.
Discussion and conclusion
Visits to pediatric emergency services due to head trauma are a prevalently encountered reason for hospital visits in Turkey as in the rest of the world. A large part of such visits consists of MHT. Studies have reported that male children are exposed to head traumas more frequently.12,13 Accordingly, it was considered to be in agreement with the literature that the male/female ratio in our study (1.67:1) was in favor of boys. The more frequent observation of childhood head traumas in boys may be explained by more adventurous and aggressive behaviors of boys.
The most frequently encountered causes of head trauma in our cases were falling in the first place and crashing stationary objects in the second place. This was the same in most similar studies.13–15
More than 80% of patients who visit emergency services due to head trauma are patients with MHT. As CBT started to be used frequently, various debates emerged on the approach on these patients. It is not appropriate to issue CBT scans for all patients as the numbers of patients are high, intracranial pathologies are detected in a very small portion of cases, it is costly for the country’s economy, and patients are exposed to radiation. In a multi-center study, CBT scans were issued for 14,969 (35.3%) among 42,414 children with head trauma due to their clinical findings, and no pathological finding could be found in 14,189 (94.8%) of these. 16 All 530 cases included in our study consisted of patients who had CBT scans, but pathological findings were found in only 44 (8.3%) among these. The finding in our study that a high ratio as 91.7% had normal CBT results supports the discussions in the literature on CBT scans (see Table 6).
Logistic regression analysis on predictability of CBT results by the PECARN, CATCH, and CHALICE criteria.
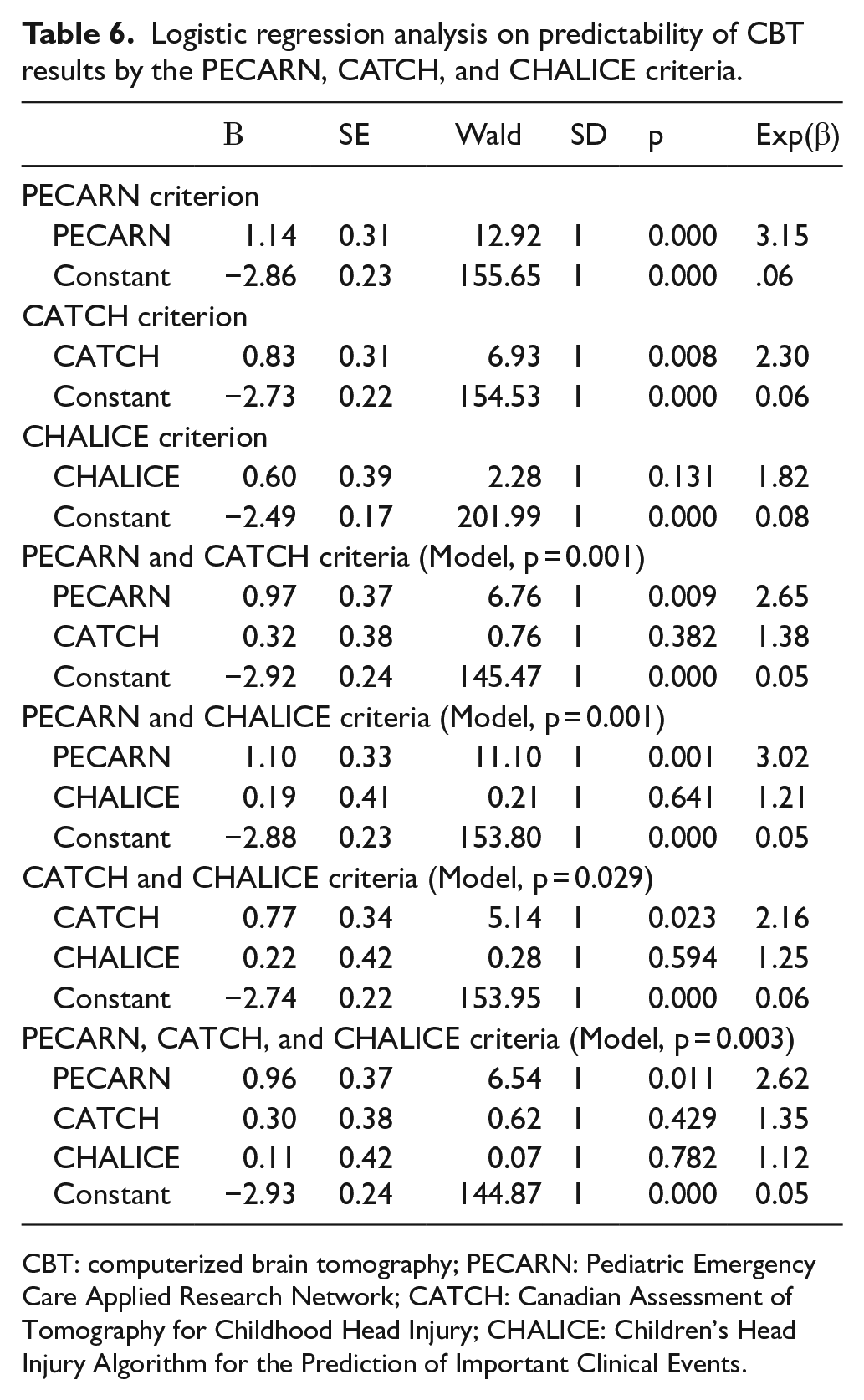
CBT: computerized brain tomography; PECARN: Pediatric Emergency Care Applied Research Network; CATCH: Canadian Assessment of Tomography for Childhood Head Injury; CHALICE: Children’s Head Injury Algorithm for the Prediction of Important Clinical Events.
Clinical decision-making rules have been developed to identify children with a high risk of head trauma, and they help clinicians minimize CBT scans while diagnosing all relevant injuries.17,18 Three sets of clinical decision-making criteria that have been developed at high methodological quality in multi-center studies with large samples are the PECARN, 16 the CATCH, 19 and the CHALICE. 20
In a study that was conducted to examine the sensitivity and specificity of the PECARN criterion, Atabaki et al. 21 compared the PECARN criteria and clinician opinions in terms of prediction of traumatic brain damage in children with MHTs. Accordingly, PECARN had a sensitivity of 100% and specificity of 53.6% for children under the age of 2 years, while it had a sensitivity of 96.8% and specificity of 58.2% for children at the age of 2 years or older. In addition to this, its positive predicted value was 2.4% and negative predictive value was 100% in children under the age of 2 years, while these values were, respectively, 2.2% and 99.95% for children at the age of 2 years or older. In another study that was carried out by Bozan et al., the PECARN and CATCH criteria were compared in 256 children with MHTs. For all cases, PECARN had a sensitivity of 48% and specificity of 83%. According to the results of the same study, the positive predicted value was 19%, while the negative predicted value was 95%. 22 Lorton et al. found among children under the age of 2 years that PECARN had a sensitivity of 100%, specificity of 64%, positive predicted value of 2%, and negative predicted value of 100%, while these values were, respectively, 100%, 72%, 2%, and 100% for children at the age of 2 years or older. For all cases, the sensitivity value was calculated as 100%, specificity was 70%, positive predicted value was 2%, and negative predicted value was 100%. 23 The issue that may be noticeable among all these studies was that the study by Bozan et al. 22 which was carried out on a Turkish sample had the highest level of similarity to our results.
Osmond et al.’s study on the CATCH criteria determined two separate methods consisting of four criteria and seven criteria. The CATCH consisting of four criteria had a sensitivity of 100% and specificity of 70.2%. The CATCH consisting of seven criteria had a sensitivity of 98.1% and specificity of 50.1%. 19 In another study, Klement et al. 24 compared CATCH criteria and Naïve Bayes criteria. In the study which included a total of 134 children with head traumas, it was calculated that the CATCH criteria had a sensitivity of 98.1% and specificity of 74.4%. Bozan et al. 22 compared the performances of the PECARN and CATCH criteria, and they calculated sensitivity as 48% and specificity as 83% for the CATCH criteria. The same study found a positive predicted value of 2.5% and a negative predicted value of 0.63%. The fact that our results were more similar to those found by Bozan et al. 22 regarding the CATCH criteria, as in the case of the PECARN criteria, supports the idea that the criteria that are used show different performances based on different societies.
It was seen that the number of studies in the literature that investigated the sensitivity and specificity of the CHALICE criteria was very limited. It may be stated that our findings were in parallel to those in the study conducted by Dunning et al., 20 where the CHALICE criteria were proposed. Their study examined 22,772 children with MHT. Accordingly, the CHALICE criteria had a sensitivity of 98.6% and specificity of 86.9%. The same study reported a positive predicted value of 8.63% and a negative predicted value of 99.9%. In our study, when we compared the sensitivity values of the PECARN, CATCH, and CHALICE criteria, we found the highest sensitivity value for CHALICE. There are some studies in the literature where these three criteria were compared to each other. Among these, the cohort-type study that was carried out by Babl et al. 25 examined 20,137 children and adolescents under the age of 18 years who visited hospitals in Australia and New Zealand in the period of 2011–2014 with complaints of MHT. In the study, the PECARN criteria had a sensitivity of 100% and specificity of 53.8% in children under the age of 2 years, while it had a sensitivity of 99% and specificity of 45.8% for those at the age of 2 years or older. The four-criteria model of the CATCH had a sensitivity of 95.2% and specificity of 84.2%, while these values were, respectively, 88.7% and 56.4% for the seven-criterion model. Finally, the authors determined that the CHALICE criteria had a sensitivity of 92.3% and specificity of 78.1%. Lyttle et al. 17 investigated 33,874 cases and found that PECARN had a sensitivity of 98.6% and specificity of 53.7% for children under the age of 2 years, while these values were, respectively, 96.7% and 58.5% for children at the age of 2 years or older. The same study found that the CHALICE criteria had a sensitivity of 97.6% and specificity of 87.3%, while the CATCH criteria had a sensitivity of 98.1% and specificity of 50.1%. 17 Another comparative study by Easter et al. 26 included 1009 cases. The sensitivity and specificity values in their study were found, respectively, as 95% and 63% for PECARN, 91% and 44% for CATCH, and 86% and 78% for CHALICE. As opposed to the case in our study, all these results reported in other studies revealed that PECARN had the highest sensitivity.
Consequently, our findings showed the effectiveness of the PECARN, CATCH, and CHALICE criteria in decision-making for CBT scans in children with MHT and made us think that unnecessary CBT scans could be avoided by using these criteria. Hence, this will clearly not only reduce exposure to radiation but also have economic contributions as a result of conducting fewer CBT scans.
Footnotes
Acknowledgements
All authors contributed to the development of the study protocol. Gizem Gizli and Vahide Aslihan Durak were responsible for obtaining ethical approval for the study and collected all data for analysis. Gizem Gizli undertook the data analysis. Ozlem Koksal, Vahide Aslihan Durak, and Gizem Gzili contributed to preparation of the manuscript and all take responsibility for its contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
All materials taken from other sources (including our own published writing) were clearly cited.
Informed consent
Written informed consent was obtained from all the patients for their anonymized information to be published in this article.
Ethical approval
This study was initiated in the ED of a university hospital following ethics committee approval.
Human rights
Our work does not infringe on any rights of others, including privacy rights and intellectual property rights. There is no human rights violation in our manuscript.