
Abstract
Background:
Despite its risks associated with renal injury, intravenous contrast media increases diagnostic efficacy and hence the chance of early diagnosis and treatment, which leaves clinicians in a dilemma regarding its use in emergency settings.
Objective:
The aim of this study was to determine the risk and predictors of contrast-induced acute kidney injury following intravenous contrast media administration for computed tomography in the emergency department.
Methods:
All patients aged 18 years and older who had a basal creatinine measurement within the last 8 h before contrast-enhanced computed tomography and a second creatinine measurement within 48–72 h after computed tomography scan between 1 January 2015 and 31 December 2017 were included in the study. Characteristics of patients with and without contrast-induced acute kidney injury development were compared. Multivariate regression analysis was used to assess the predictors for contrast-induced acute kidney injury.
Results:
A total of 631 patients were included in the final statistical analysis. After contrast media administration, contrast-induced acute kidney injury developed in 4.9% (n = 31) of the patients. When the characteristics of patients are compared according to the development of contrast-induced acute kidney injury, significant differences were detected for age, initial creatinine, initial estimated glomerular filtration rate, and all acute illness severity indicators (hypotension, anemia, hypoalbuminemia, and need for intensive care unit admission). A multivariate logistic regression analysis was performed. The need for intensive care unit admission (odds ratio: 6.413 (95% confidence interval: 1.709–24.074)) and hypotension (odds ratio: 5.575 (95% confidence interval: 1.624–19.133)) were the main factors for contrast-induced acute kidney injury development.
Conclusion:
Our study results revealed that hypotension, need for intensive care, and advanced age were associated with acute kidney injury in patients receiving contrast media. Therefore, we believe that to perform contrast-enhanced computed tomography in emergency department should not be decided only by checking for renal function tests and that these predictors should be taken into consideration.
Introduction
Contrast-induced acute kidney injury (CI-AKI) is classically defined as a sudden decline of renal function secondary to contrast media exposure in the absence of other causes of renal failure.1,2 It was reported that CI-AKI, indicated as the third most common cause of in-hospital renal failure, may cause prolonged hospitalization and increased morbidity and/or mortality.3–5
Former studies in the literature have focused on CI-AKI development secondary to elective and interventional procedures, mainly coronary angiography.6,7 However, the frequency of using contrast-enhanced tests has been gradually increasing in emergency department (ED) where usually acute and critical cases are evaluated and making a rapid and accurate diagnosis is essential.8,9 Despite its risks associated with renal injury, intravenous contrast media increases diagnostic efficacy and hence the chance of early diagnosis and treatment, which leaves clinicians in a dilemma regarding its use in emergency settings. However, there are a limited number of publications in the literature focusing on this dilemma and investigating the development of CI-AKI after contrast media use in the ED.8,10–12
The primary aim of our study was to determine the risk and predictors of CI-AKI development following intravenous contrast media administration for computed tomography (CT) in the ED. We also aimed to investigate the effects of nephroprotective protocols administered in the ED on renal function tests.
Methods
Study setting and population
This single-center retrospective study was conducted in an ED with 250,000 admissions per year. This study was approved by the local ethics committee. All patients older than 18 years who underwent CT in the ED between 1 January 2015 and 31 December 2017 were included in the study. In our institute, whether to use contrast media during CT scan is decided by emergency physician responsible for the patient by evaluating the patient’s clinical and laboratory findings in accordance with the preliminary diagnoses. Abdominal and pelvic contrast-enhanced CT are preferred in the presence of acute abdomen and trauma, and contrast-enhanced CT angiography is performed for vascular pathologies (embolism, thrombosis, dissection, etc.) in thorax, abdomen, and pelvis. The study group was formed through hospital automation system and consisted of patients who had a basal creatinine measurement within the last 8 h before contrast-enhanced CT and a second creatinine measurement within 48–72 h after CT scan. Patients who had a basal creatinine level of 4 mg/dL or above (acute kidney injury (AKI) work group criteria stage 3: 13 patients who already developed severe AKI), those with a history of renal transplant or hemodialysis, and pregnant women were excluded. Since the required proportional creatinine increase (25%) for the diagnosis of CI-AKI is less than 0.1 mg/dL (i.e. <1 unit of measure for the parameter of creatinine), patients with basal creatinine level less than 0.4 mg/dL may easily be misdiagnosed as CI-AKI due to causes unrelated to acute kidney injury such as activity, diet, or simple laboratory errors. Therefore, patients with initial creatinine level <0.4 mg/dL were also excluded from the study in order to minimize enrolling patients who might be erroneously diagnosed with acute renal injury and to avoid selection bias. The patients’ demographic data, comorbid disorders, pre- and post-CT serum creatinine/estimated glomerular filtration rate (eGFR) values, presence of “acute-illnesses severity indicators” 14 (hypotension, anemia, hypoalbuminemia, and need for intensive care unit (ICU) admission determined by emergency physician), and nephroprotective treatments were retrospectively reviewed through hospital automation system. Systolic blood pressure lower than 90 mmHg and serum albumin level lower than 3.5 g/dL were accepted as hypotension and hypoalbuminemia, respectively. Anemia was defined as a hematocrit level of less than 39% for men and 36% for women. If an intensive care consultation was requested for admission to ICU by the emergency physician responsible for the patient, it was accepted that there was “need for ICU admission” for that patient. Contrast-enhanced CT scans for more than one anatomic site were considered as a single contrast-enhanced CT scan in a single patient. In our institute, the primary physician, who is responsible for the patient, assesses the need for nephroprotective treatment before contrast-enhanced CT and then selects one of three standard regimens to be administered within 1 h prior to CT scan: intravenous (IV) infusion of 1000 mL normal saline (NS), IV infusion of 1200 mg N-acetyl cysteine (NAC) + 1000 mL NS, or IV infusion of 40 mEq 8.4% NaHCO3 + 1000 mL NS. In our study group, patients who received 1000 mL NS infusion within 1 h before contrast-enhanced CT scan were considered to have received NS as nephroprotective treatment. A volume of 100 mL of non-ionic low-osmolar lohexol (300 mg iodine/mL; Omnipaque™) was used for all contrast-enhanced CT scans. Patients with missing data were excluded.
Outcome measure
The study outcome was CI-AKI development in patients undergoing contrast-enhanced CT. CI-AKI was defined as an increase in second creatinine level 0.5 mg/dL or 25% increase over baseline creatinine level at 48–72 h after CT scan.
Statistical analysis
Data analysis was performed using SPSS for Windows 16.0 (Chicago, IL, USA) software package. The normality of discrete and continuous variables was tested with Kolmogorov–Smirnov test. Descriptive statistics were expressed as mean ± standard deviation (SD) or median (interquartile range (IQR 25%–75%)) for continuous variables, and number and percentage for categoric data. Categoric variables were compared with chi-square test and the continuous variables with Mann–Whitney’s U test. The predictive role of the variables was tested with multivariate regression analysis. Prior to this, a univariate analysis was performed, and variables with a p-value less than 0.2 were included in the multivariate model. Spearman’s test was used to test inter-variable correlations; one (baseline creatinine) of the inter-related variables (baseline creatinine and baseline eGFR) was removed from the regression model. Fitness of the model was tested with Hosmer–Lemeshow test, and p-value less than 0.05 was considered statistically significant.
Results
During the study period, a total of 5980 patients underwent CT procedure. There was a total of 996 patients whose pre- and post-CT creatinine levels were available at appropriate time intervals and who were thus suitable for enrollment. However, 118 patients were excluded due to missing data. A total of 631 patients who underwent contrast-enhanced CT during the study period were included in the final statistical analysis (Figure 1, study flowchart). The median age was 52 (interquartile range (IQR 25%–75%): 38–67) years. The most common acute illness severity indicator found was hypoalbuminemia. Demographics and some laboratory results of all patients are shown in Table 1.
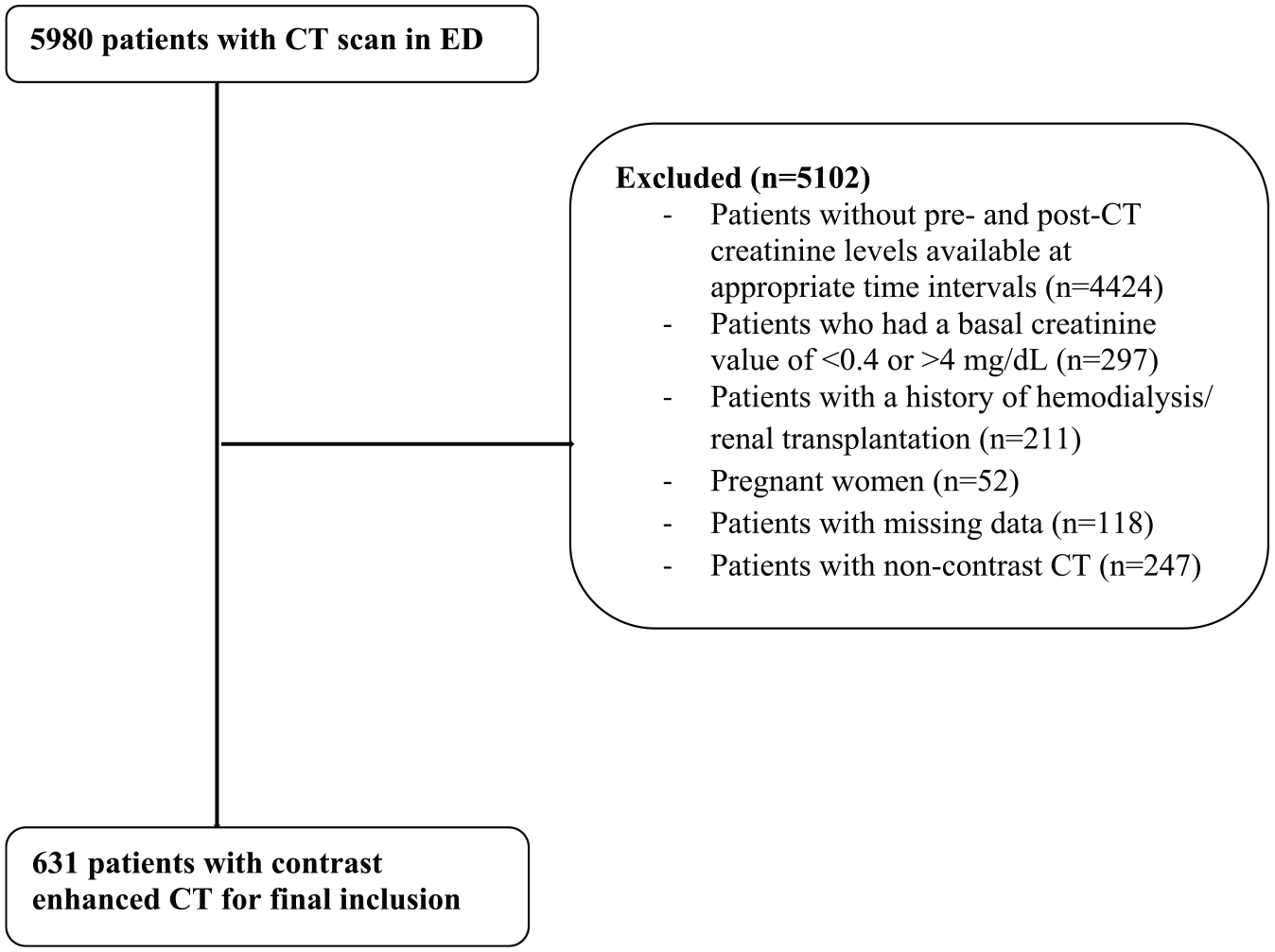
Study flowchart.
Demographics and clinical characteristics of patients who performed CT with contrast media.
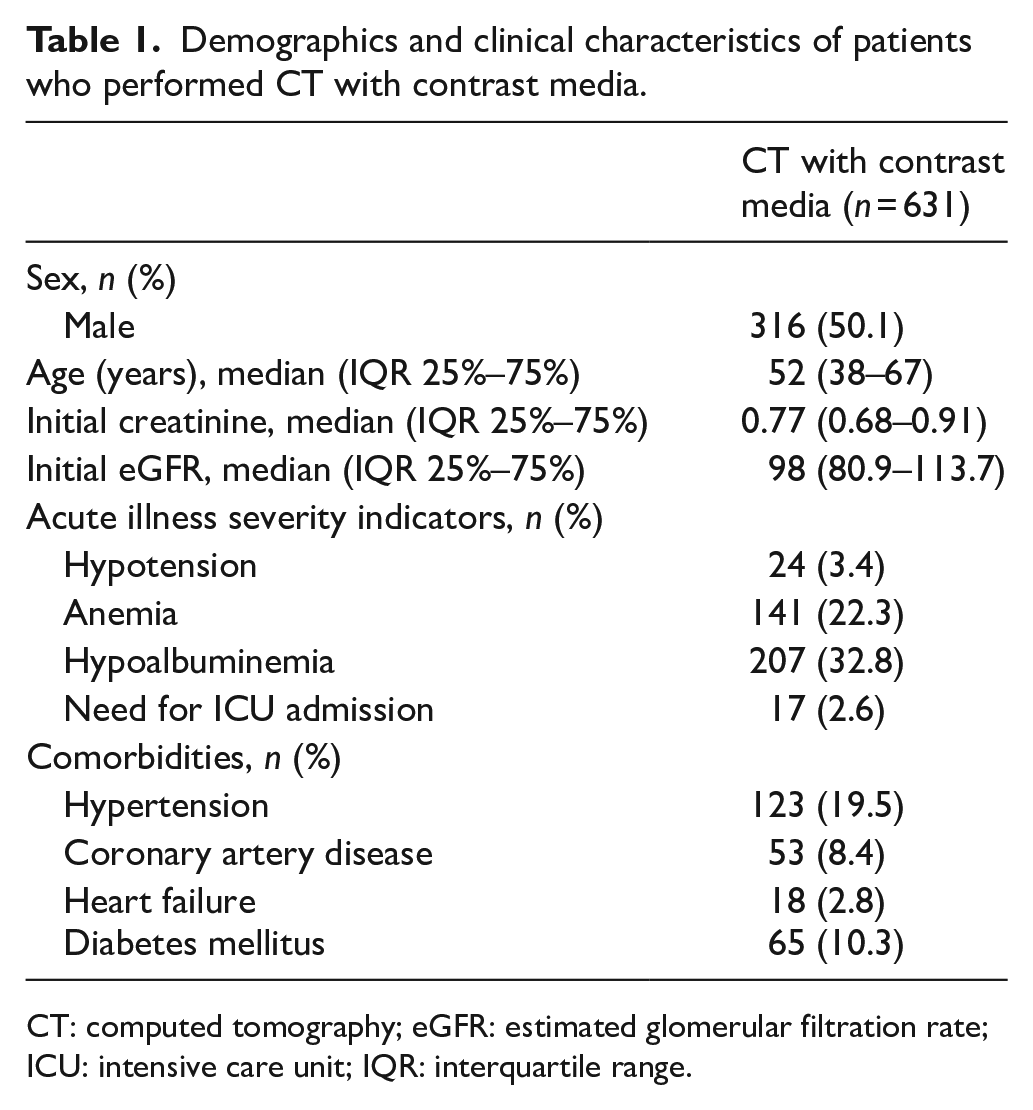
CT: computed tomography; eGFR: estimated glomerular filtration rate; ICU: intensive care unit; IQR: interquartile range.
After contrast media administration, CI-AKI developed in 4.9% (n = 31) of the patients. Only one patient received hemodialysis. Renal functions improved after two sessions of hemodialysis and permanent renal failure did not develop in this patient. None of the 31 patients who met the CI-AKI criteria died within 30 days. When the characteristics of patients are compared according to the development of CI-AKI, significant differences were detected for age, initial creatinine, initial eGFR, and all acute illness severity indicators (hypotension, anemia, hypoalbuminemia, and need for ICU admission) (p < 0.05 for all; Table 2).
Characteristics of patients who did or did not develop CI-AKI.
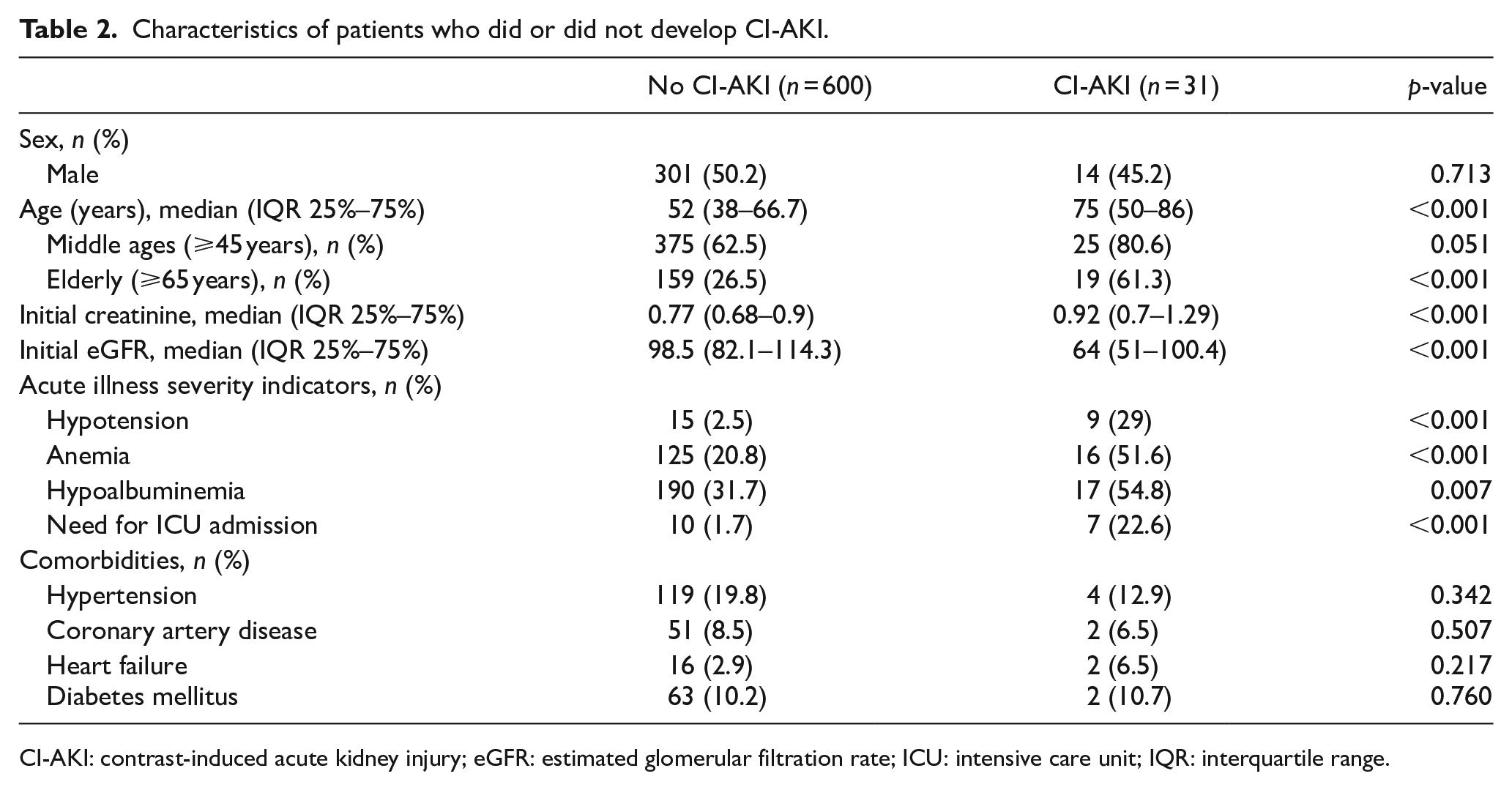
CI-AKI: contrast-induced acute kidney injury; eGFR: estimated glomerular filtration rate; ICU: intensive care unit; IQR: interquartile range.
A multivariate logistic regression analysis was performed to examine the effects of the variables given in Table 2 on CI-AKI development. Age, sex, initial creatinine, hypotension, anemia, hypoalbuminemia, and need for ICU admission were included in the model and the fitness of the model was tested using Hosmer–Lemeshow test. The need for ICU admission and hypotension were the most associated factors with CI-AKI development (OR: 6.413 (95% CI: 1.709–24.074) and OR: 5.575 (95% CI: 1.624–19.133), respectively) (Table 3).
Multivariate regression model to predict the development of CI-AKI.
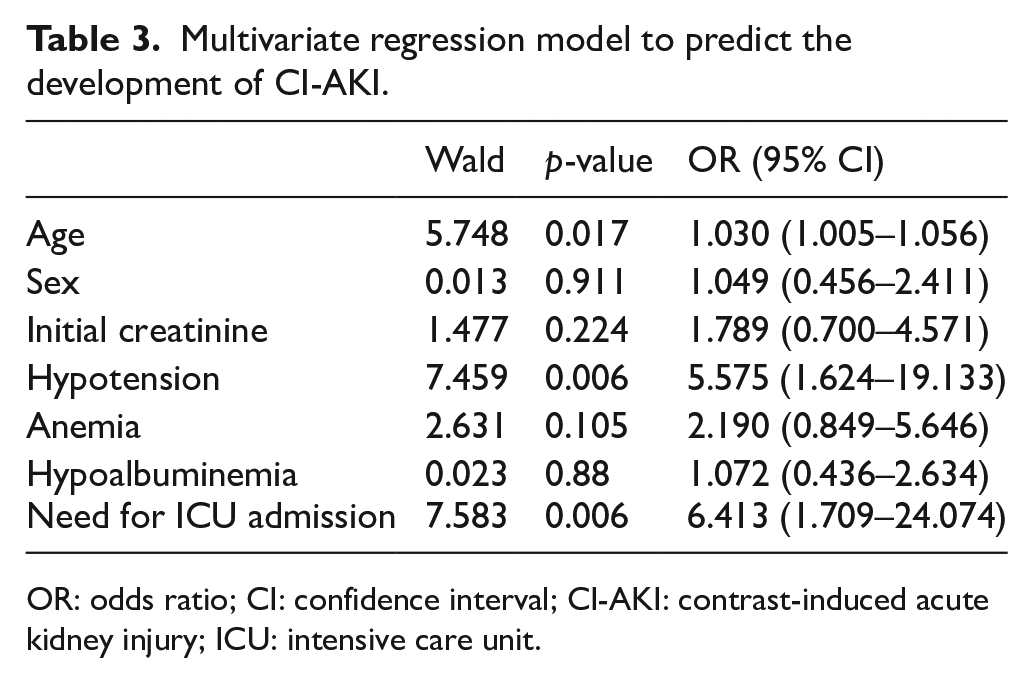
OR: odds ratio; CI: confidence interval; CI-AKI: contrast-induced acute kidney injury; ICU: intensive care unit.
A total of 131 patients receiving contrast media were administered nephroprotective treatment (NS, NAC, or NaHCO3). The most commonly preferred agent was NS. Although NaHCO3 was more preferred for patients with a lower baseline eGFR level, it was the agent that produced the least eGFR change (ΔeGFR
Comparison of nephroprotective therapy options for CI-AKI in contrast media administration.
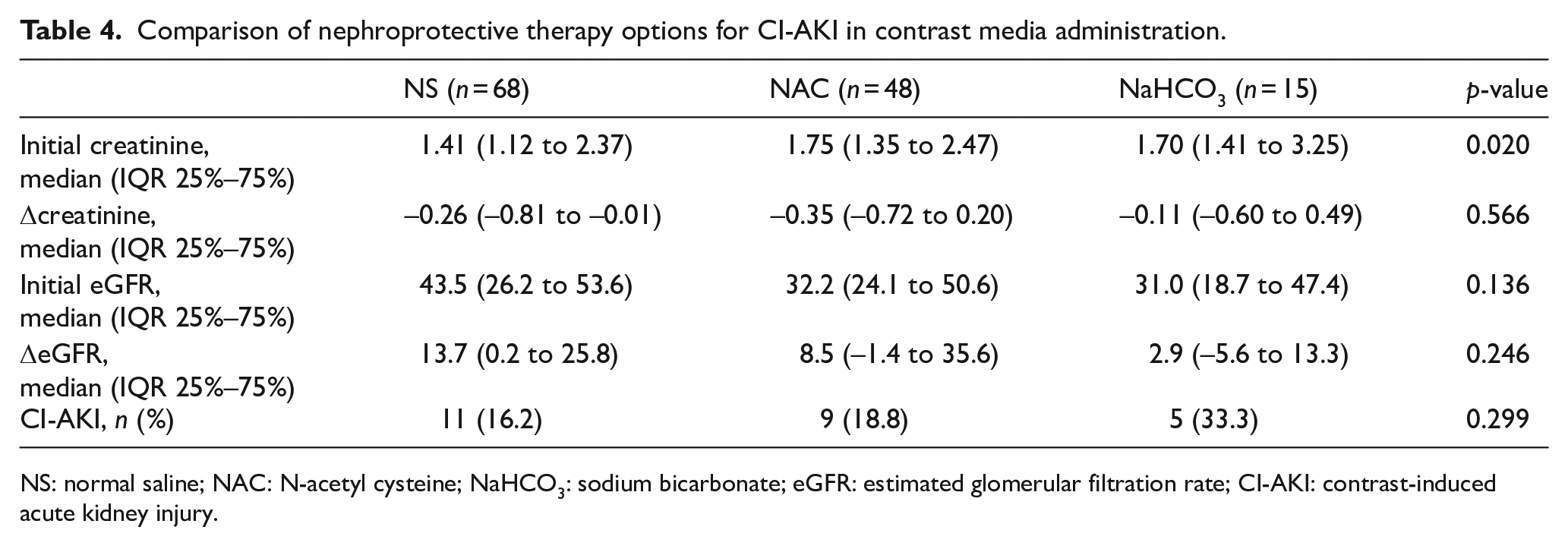
NS: normal saline; NAC: N-acetyl cysteine; NaHCO3: sodium bicarbonate; eGFR: estimated glomerular filtration rate; CI-AKI: contrast-induced acute kidney injury.
Discussion
In this study, where we aimed to assess the risk of CI-AKI development after intravenous contrast media administration for CT scan in the ED, we reached two important conclusions. First, we found that the need for ICU admission, hypotension, and advanced age were associated with CI-AKI development. We believe that in patients with hypotension and need for ICU admission, inadequate renal perfusion and failure of compensation mechanisms in a possible shock scenario may cause CI-AKI development. In the advanced age group with a relatively low cardiovascular reserve and possible vascular pathologies, however, possible increase in free radicals may have caused an increased CI-AKI rate. Second, a comparison of nephroprotective treatment regimens revealed no significant statistical difference between NS, NAC, and NaHCO3 for CI-AKI development. There is conflicting data in the literature about the usefulness of available treatment protocols. We think that the lack of a clear definition of pathophysiological processes underlying CI-AKI is the most possible reason of the inability to develop a clear treatment protocol.
In the literature, the rate of CI-AKI has been reported 4% by Kim et al., 15 5.6% by Sinert et al., 16 7.3% by Traub et al., 10 12% by Mitchell et al., 17 and 27.5% by Lefel et al. 18 We found a rate of 4.9% in our study. As well as the heterogeneity of study populations, the type, and the amount of contrast media used; time interval for checking control renal function tests; and inconsistencies of CI-AKI definitions between different studies may explain the wide range of CI-AKI rates. As for the risk factors for CI-AKI development in contrast media exposed patients, Lefel et al. 18 reported low GFR, high intensive care scores, and low hemoglobin as the most important parameters. The main related factors of CI-AKI revealed in our study, however, were need for ICU admission, hypotension, and advanced age. In the literature, renal hypoxic–ischemic processes are the pathophysiological mechanisms still widely implicated for CI-AKI development. 19 Another potential mechanism has been shown as free radical formation in kidneys. 20 As age increases, the formation and possible damage of free oxygen radicals is expected to increase, while GFR decreases by around 10% per decade. 21 We believe that all these factors pave the way for CI-AKI development in patients with advanced age who have decompensated hemodynamic processes.
Osmolality and the amount of contrast media have been reported as important factors for CI-AKI development. Rudnick et al. 22 noted that high-osmolar contrast media had a greater risk for CI-AKI than low-osmolar ones. Although several studies reported no difference between iso-osmolar and low-osmolar contrast media for CI-AKI development, Aspelin et al. suggested that iso-osmolar contrast media was more suitable for high-risk patients undergoing interventional angiography.23–25 Despite these conflicting results, non-ionic low-osmolar contrast media is still the most preferred agent worldwide. Higher amounts of contrast media use have also been a well-documented CI-AKI risk factor. Nikolsky et al. 26 determined that each 100 mL increment in contrast volume leads to a 30% increase in the odds of CI-AKI. Relatively low doses of contrast media were considered to be 100 mL or less by Mehran et al. 2 In our study, relatively low dose (100 mL) of non-ionic low-osmolar lohexol was used for all contrast-enhanced CT scans.
As no definitive treatment exists for CI-AKI, most studies have focused on its prevention and prophylaxis. 6 The available treatment protocols are usually based on volume expansion and administering antioxidant treatment against free radicals.19,27 However, contradictory data have been reached in clinical studies regarding the efficacies of different treatment protocols, and no net superiority of one over the others has been shown.6–8,10,27,28 Our study aimed to evaluate the short-term nephroprotective treatments appropriate to the rapid patient circulation of ED in patients receiving contrast media only for emergency imaging purposes. The retrospective design of our study also allowed us to reflect the preferences of emergency physicians in nephroprotective treatment protocols in daily practice. In our study, while the most commonly administered nephroprotective treatment was NS, we noted that as eGFR dropped further, clinicians tried additional agents (NAC or NaHCO3) with the worry of increased CI-AKI risk. The most effective treatment on eGFR levels was NS; however, we found that none of the three treatment options had superiority over one another for preventing CI-AKI in patients receiving prophylaxis. This suggests that CI-AKI is a result of much more complicated processes beyond numeric deterioration of renal function tests. We believe that the inability to reveal these pathophysiological processes is the main obstacle in developing a precise treatment protocol.
Limitations
Our study has some limitations. After CT scan, creatinine levels might have increased in some of the patients secondary to underlying conditions, independent of initial creatinine level (normal or abnormal) or contrast exposure. However, these patients might have been mistakenly classified as CI-AKI cases. In contrast, we may have missed some patients with CI-AKI as we used a narrow time window for control renal function tests. Although several studies have assessed renal functions up to 7 days after contrast media exposure for diagnosing CI-AKI, we based our diagnosis on control creatinine level measured 48–72 h after tomography. 29 In addition, CI-AKI was diagnosed by assessing only creatinine levels in our study. Although urine output is another important parameter for the diagnosis of AKI, its use for the definition of CI-AKI has not been clarified in the literature. Despite the presence of indication, intravenous contrast media might have not been used in some of our patients due to contrast allergy. In addition, since prophylaxis was not administered in all patients who underwent contrast-enhanced CT and the number of patients who developed CI-AKI was not enough, the nephroprotective treatment parameter could not be included in the statistical analysis. The most important limitation of our study is the low number of patients developing CI-AKI in our contrast-administered patient population. Also, due to the retrospective nature of the study, clinical reflections of CI-AKI, such as acid–base status and potassium levels, and all clinical outcomes could not be reached in all patients. Our study is a single-center study. It is possible that some of the patients undergoing contrast-enhanced CT may have been admitted to other healthcare facilities after their discharge from our hospital.
Conclusion
According to the results of our study, hypotension, need for intensive care, and advanced age were the most associated factors with development of AKI in patients receiving contrast media. Therefore, we believe that clinicians should not only decide contrast media use solely by taking into account renal function tests in ED but also consider the presence of these predictors. In addition, none of the three nephroprotective agents most commonly used in daily practice showed superiority over the others. Therefore, we think that the most important step in CI-AKI prevention is accurately determining which patients are to be administered with the contrast media.
Footnotes
Authors’ note
The article has been presented as oral presentation in the 15th National Emergency Medicine Congress, 6th Intercontinental Emergency Medicine Congress, and 6th International Critical Care and Emergency Medicine Congress, 25–28 April 2019, Antalya, Turkey.
Author contributions
Study conception and design was done by S.D., E.E., and Y.Ç.; acquisition of data was done by S.D., Ş.K.Ç., Ö.Ö., and H.U.; formal analysis was carried out by Ş.K.Ç., E.E., S.D., and Ö.Ö.; writing original draft preparation was carried out by S.D. and E.E.; writing review and editing was performed by Ş.K.Ç., Y.Ç., and H.U.; and supervision was done by Y.Ç. and E.E.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The dataset generated and/or analyzed during this study is available from corresponding author.
Ethical approval
Ethical approval for this study was obtained from Kecioren Training and Research Hospital Ethics Committee (no. 2012-15/1579).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. This is a retrospective study and all human rights were well respected.
Informed consent
Written informed consent was not necessary. This is a retrospective study and no specific patient data have been included in the manuscript.