
Abstract
Backround:
High rates in trauma-related mortality pose a major health problem and increase every day. Early diagnosis and treatment can be lifesavers for this patient group in the emergency departments, which serve as the first place to admit trauma patients in a hospital.
Objectives:
We aim to determine high-risk criteria to indicate trauma patients getting the most use from whole-body tomography in patients with multiple traumas and reduce unnecessary computed tomography.
Methods:
We examined retrospectively all electronic files and computed tomography results of patients, who had been admitted to emergency department due to trauma, and who had undergone whole-body computed tomography.
Results:
We found that possibility of multiple injuries increased by 5.9 times in patients requiring mechanical ventilation. Possibility of multiple injuries in patients with free fluid in the Focused Assessment with Sonography for Trauma increased by 5.6 times. We also observed that possibility of multiple injuries in patients with Glasgow Coma Score < 13 increased by 4.3 times. Possibility of multiple injuries in hypoxic patients increased by 3.2 times. Possibility of multiple injuries in patients with a pulse ≥ 120/min increased by 1.8 times. Possibility of multiple injuries in patients with shock index ≥ 0.9 increased by 1.7 times.
Conclusion:
High-risk group in terms of multiple traumas involves mechanical ventilation need in trauma patients, positive Focused Assessment with Sonography for Trauma, Glasgow Coma Score being under 13, hypoxia, tachycardia, positive shock index, and extravehicular traffic accidents. Whole-body computed tomography should be performed in this patient group.
Introduction
High rates in trauma-related mortality pose a major health problem and increase every day. Early diagnosis and treatment can be lifesavers for this patient group in the emergency departments, which serve as the first place to admit trauma patients in a hospital. Therefore, all the interventions aiming at diagnosis in trauma patients are very significant and various studies have been more conducted on this subject. Particularly, on the initial assessment of trauma patients, the use of computed tomography (CT) has gradually increased in the recent years.1–4 A substantial increase in the utilization of CT has been noted in the emergency department, which ranged from an increase of 51% to 463%, depending on the anatomic regions imaged. 4 Traditionally, CT scans have been used to further define injuries found or suspected during the primary and secondary surveys; however, today it is being progressively used as a primary imaging tool for every trauma patient who does not present even any extremity injuries.5–7 Whole-body CT is remarkable with regard to its capacity in detecting injuries that might be disregarded in trauma patients and shortening the delays in patient administration.1,3,5,8
In a recent study from the United Kingdom, the trauma pan-scan detected 17 unanticipated injuries in 138 patients, posing immediate therapeutic consequences in three cases (two laparotomies and one chest tube). 1 Whole-body CT scans are able to detect injuries more; however, the impact of these injuries on clinical outcomes is disputable. Some researchers argue that hidden injuries that are detected by the CT scans may have very little effects on patient management or prognosis.7,8 Primer could not find any statistical difference in terms of survival in the meta-analysis of studies comparing mortality rates between whole-body CT scans and more selective CT scanning protocols.8,9 Moreover, the possibility of unnecessary scans may increase when whole-body CT scans are given to every patient and thereby the risk of radiation emerges as another problem. 7
Instead, liberal use of whole-body CT is likely to increase the number of unnecessary scans. 7 And despite the advances in imaging techniques, whole-body CT is still associated with significant radiation exposure. Estimated radiation for whole-body CT is approximately 20 mSv, which is significantly higher than the average 9.2 mSv for conventional workup with plain film radiography and selective CT.10,11 Exposure to greater than 20 mSv carries a cancer risk of more than 1 in 1000 based on theoretical population-weighted estimates. 12
Therefore, considering all the discussions, it is noted that more specific criteria are required in determining trauma patients who will benefit the most from the whole-body CT scans in order to eliminate unnecessary CT scan rates.1,5,8,13 Our aim in this particular study is to determine trauma patients who will benefit the most from whole-body CT scans in the emergency department.
Methods
We conducted our study in a single-centered, university-affiliated tertiary hospital with an annual in-patient admission of 140,000 on average. Trauma patients were average 11% (n = 15,000). We examined retrospectively electronic files and CT results of patients who were admitted to the emergency department and given the whole-body CT scans (plain craniocervical CT and CT Torso with IV contrast) due to trauma within a period of 9 months between 01 January 2014 and 30 September 2014. Whole-body CT scans were performed according to the criteria in Box 1 within a period of 9 months between 01 January 2014 and 30 September 2014. Positive CT findings were assessed as in Craniocervical CT: bleeding-fracture-contusion, cervical fracture dislocation; in Thorax CT: pneumothorax, hemothorax, contusion, rib fracture; in whole abdominal CT: free fluid, pelvic fracture, spinal fracture, solid organ injuries. Non-traumatic admissions and patients who were not given whole-body CT scans were excluded from the study. In our study period, there were 12,000 trauma patients admitted to our emergency department. Not all of them were multi-trauma patients. We could not give clear numbers about who were multi-trauma patient or not, because lack of our medical data system. So, our proportion of whole-body computed tomography (WBCT) patient was about 5%.
Whole-body CT scans criteria. 14
We made use of the results of the FAST (Focused Assessment with Sonography for Trauma) performed by emergency medicine physicians and finalized CT reports assessed by radiology physicians. Shock index (SI) of patients (pulse/systolic blood pressure) calculated as 0.9 or higher was indicated positive. Patients were assessed as multiple trauma patients if two or more body regions were affected.
Data were recorded and then analyzed via the SPSS program (version 15). Descriptive statistics (mean, minimum, and maximum), standard deviation, and frequency tables were used as the basic statistical analysis. The chi-square analysis was used to determine the significance between the two groups in the advanced statistical analysis, and continuous variables were analyzed using the Student’s t-test to determine the significance between the averages. A p-value < 0.05 was considered statistically significant.
Results
In total, 546 patients were underwent whole-body CT during the study period. It was noted that 29% (n = 158) of the patients were admitted due to falls from height > 3 m, 25% (n = 135) due to in-vehicle traffic injuries, and 23% (n = 123) due to motorcycle crash.
Positive findings of patients in terms of tomographic results and clinical severity are displayed in Table 1.
Comparative analysis of whole-body CT results with independent factors in the study.
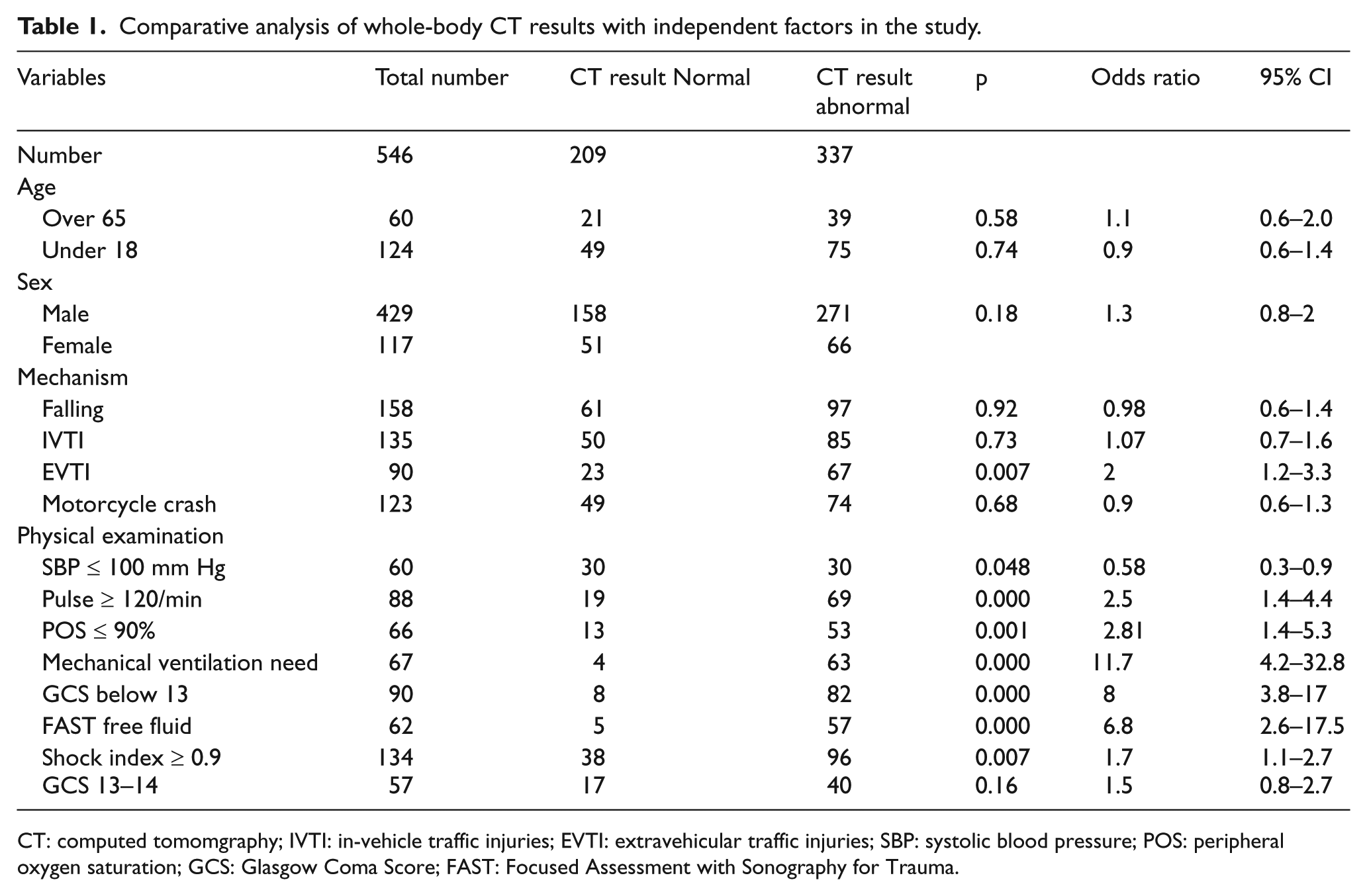
CT: computed tomomgraphy; IVTI: in-vehicle traffic injuries; EVTI: extravehicular traffic injuries; SBP: systolic blood pressure; POS: peripheral oxygen saturation; GCS: Glasgow Coma Score; FAST: Focused Assessment with Sonography for Trauma.
About 62% (n = 337) of the whole-body CT results of the patients were found abnormal. Multiple trauma was observed in 27% (n = 148) of the patients. While injuries involving two regions rate was measured as 21% (n = 116), injuries involving three regions rate was found 6% (n = 32) in our study. We indicated the most observed findings as: intracranial bleeding with a rate of 23% in central nervous system, rib fracture with a rate of 28% in respiratory system, and vertebral fracture with a rate of 14% in abdominal tomography examinations (Table 2).
Abnormal findings in whole-body CT.

When whole-body CT findings were examined in terms of independent variables (age, sex, trauma mechanism, vital values, mechanical ventilation need of the patient (all intubated patients managed with mechanical ventilation with intermittent positive-pressure ventilation (IPPV)), the FAST finding, and Glasgow Coma Score (GCS) value) used in the study, at least one positive finding was found in 337 patients. It was also indicated that the possibility of multiple injuries in patients requiring mechanical ventilation increased by 5.9 times (Table 4) and the possibility of a positive finding in whole-body CT scans increased by 11.7 times compared to the patients who do not require mechanical ventilation. The possibility of a positive finding in patients requiring mechanical ventilation was 7.4 times more in craniocervical CT, 3.7 times more in thorax CT, and 2.5 times more in whole abdominal CT (Tables 1 to 3).
Comparison of CT results of the systems with regard to independent variables.
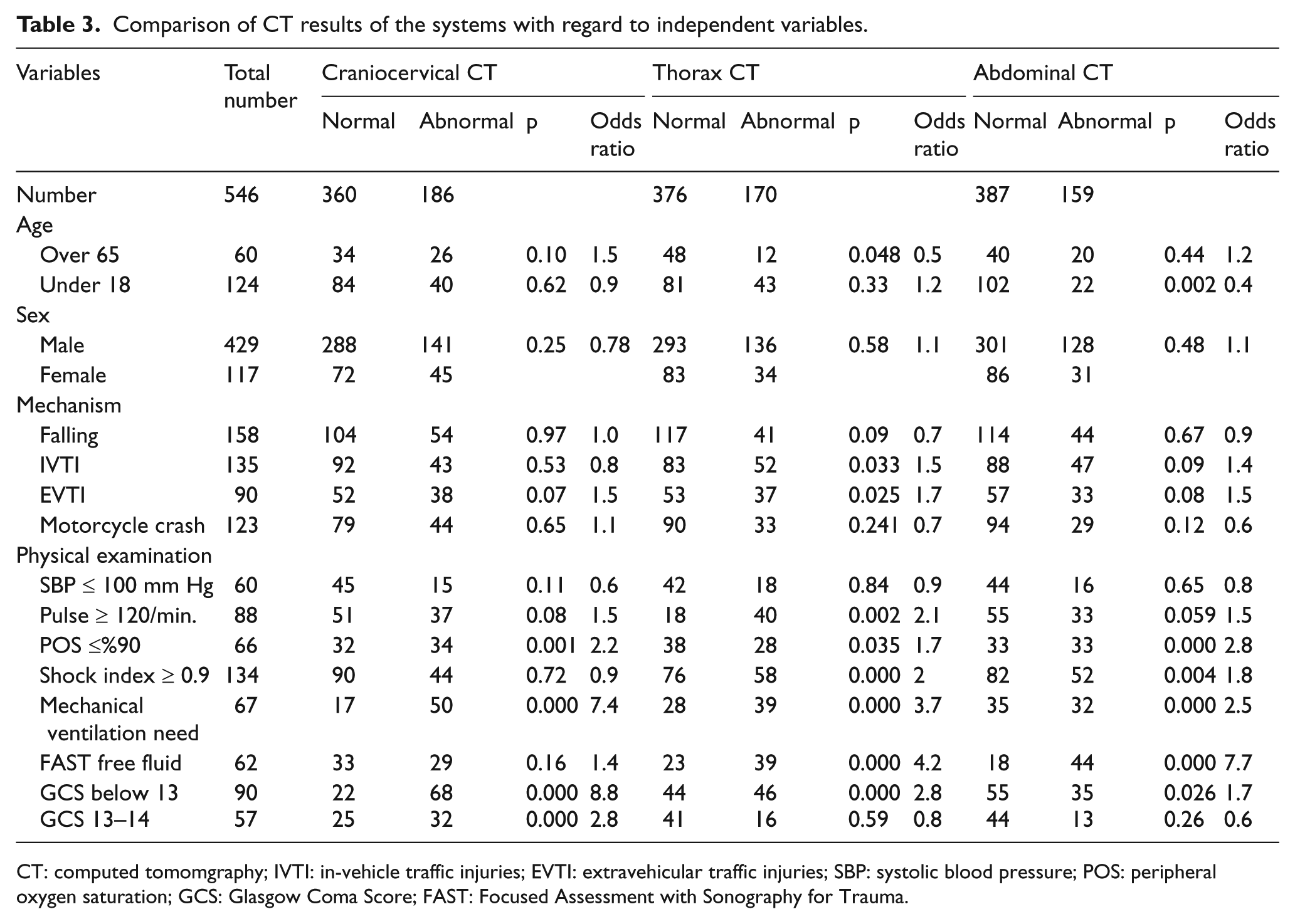
CT: computed tomomgraphy; IVTI: in-vehicle traffic injuries; EVTI: extravehicular traffic injuries; SBP: systolic blood pressure; POS: peripheral oxygen saturation; GCS: Glasgow Coma Score; FAST: Focused Assessment with Sonography for Trauma.
It was also determined that the possibility of multiple injuries in patients with free fluid in the FAST increased by 5.6 times (Table 4) and the possibility of a positive finding in the whole-body CT increased by 6.8 times compared to the patients who did not have free fluid according to the FAST. The possibility of a positive finding in the patients with free fluid according to the FAST was 4.2 times more in thorax CT and 7.7 times more in whole abdominal CT (Tables 1 to 3).
Comparison of multi-trauma patients with other patients in terms of independent variables.
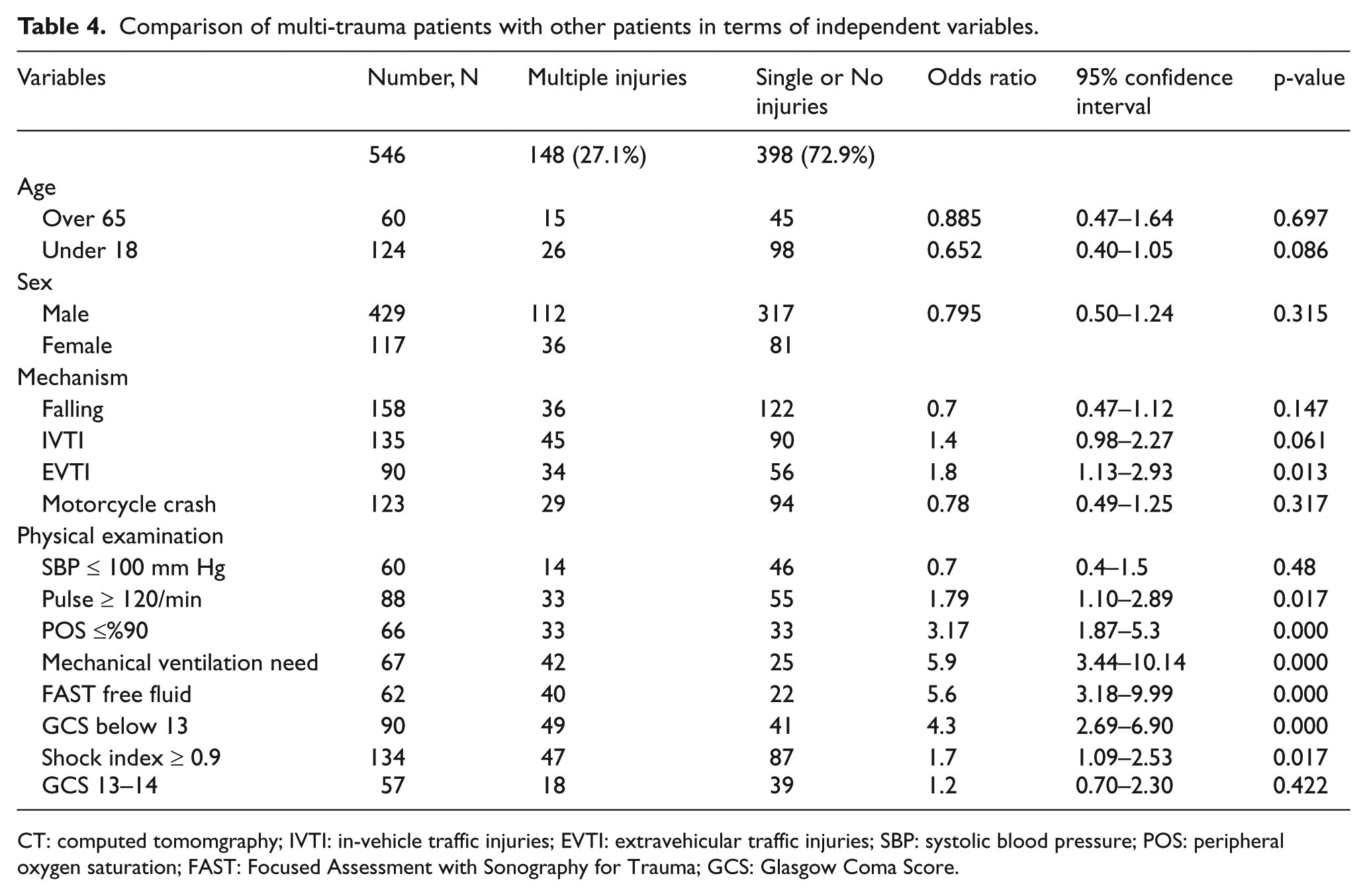
CT: computed tomomgraphy; IVTI: in-vehicle traffic injuries; EVTI: extravehicular traffic injuries; SBP: systolic blood pressure; POS: peripheral oxygen saturation; FAST: Focused Assessment with Sonography for Trauma; GCS: Glasgow Coma Score.
It was found that the possibility of multiple injuries in patients with GCS < 13 increased by 4.3 times (Table 4) and the possibility of a positive finding in whole-body CT increased by 8 times compared to the patients with GCS ≥ 13. The possibility of a positive finding in patients with GCS < 13 was 8.8 times more in craniocervical CT, 2.8 times more in thorax CT, and 1.7 times more in whole abdominal CT (Tables 1 to 3).
Moreover, we determined that the possibility of multiple injuries in patients with peripheral oxygen saturation ≤ 90% increased by 3.2 times (Table 4) and the possibility of a positive finding in the whole-body CT increased by 2.8 times compared to the patients with normal peripheral oxygen saturation. The possibility of a positive finding in patients with peripheral oxygen saturation ≤ 90% was 2.2 times more in craniocervical CT, 1.7 times more in thorax CT, and 2.8 times more in whole abdominal CT (Tables 1 to 3).
We also found that the possibility of multiple injuries in patients with a pulse rate of ≥ 120/min. increased by 1.8 times (Table 4) and the possibility of a positive finding in whole-body CT increased by 2.5 times compared to the patients with a pulse rate below 120 per minute. The possibility of a positive finding in patients with a pulse rate of ≥ 120/min. was 2.1 times more in thorax CT and 1.5 times more in whole abdominal CT (Tables 1 to 3).
Moreover, we indicated that the possibility of multiple injuries in EVTI (extravehicular traffic injuries) patients increased by 1.8 times (Table 4) and the possibility of a positive finding in whole-body CT increased by 2 times compared to IVTI (in-vehicle traffic injuries) patients. The possibility of a positive finding in EVTI patients was 1.7 times more in thorax CT (Tables 1 to 3).
It was also concluded that the possibility of multiple injuries in patients with a SI of 0.9 increased by 1.7 times (Table 4) and the possibility of a positive finding in whole-body CT increased by 1.7 times compared to the patients with normal SI. The possibility of a positive finding in patients with a SI of 0.9 was 2 times more in thorax CT and 1.8 times more in whole abdominal CT (Tables 1 to 3).
Finally, when we examined clinical patient outcomes, we observed that 47% (n = 258) of the patients were hospitalized, 47% (n = 260) of the patients were discharged (our emergency department acting as a level 3 trauma center, so we may discharge patients from our emergency department without any hospitalization), 2% of the patients (n = 10) were transferred, 2% of the patients leave hospital without permission, and 1% (n = 5) of the patients were death. In our study, 25 positive multiple injuries patients have undergone operative measures instead of pure supportive management. So, it means that there was around 4.6% of patients has major changed of their management plan after WBCT.
Discussion
In our study aiming to indicate risky patient group with regard to multiple injuries in whole-body CT scans for traumatic patients, we found that the need for mechanical ventilation, fluid detected by the FAST, GCS being under 13, hypoxia, tachycardia, raised SI, and extravehicular traffic injuries as a mechanism served as the basis for findings to determine were high-yield criteria for WBCT in polytrauma. The highest risk groups in terms of multiple traumas involved, respectively, the need for mechanical ventilation, detection of free fluid in the FAST, GCS being under 13, and hypoxia. Moreover, we observed that these findings did not always indicate system injuries; for instance, hypoxia involved mostly craniocervical injury.
Traumas are annually causing 5.8 million deaths in 1998 and this number accounts for approximately 10% of deaths in total. 15 The World Health Organization 16 estimated that there would be a 28% increase in injury-related mortalities between 2004 and 2030.
Hence, trauma management in emergency departments has progressively become more significant. In the REACT study, a randomized, controlled study where international, multi-centers including four hospitals from the Netherlands and one from Switzerland were involved to conduct some research on whole-body CT, it was noted that there was not any significant difference in terms of in-hospital mortalities when WBCT was compared with conventional CT scanning. 14 Even though mortality is a primary criterion in these similar studies, clinical conditions may also function as important as other criteria on a daily practice. Among these conditions, whole-body CT detecting any possible overlooked diagnosis, additional pathologies that are not fatal but causing morbidity and disability can be listed. Taking these clinical conditions into consideration does not only contribute to our ability to indicate diagnosis that may interfere with the patients’ quality of life, but also helps reduce the number of medical legal issues. Similar to the REACT study, mortality rates in the emergency department are very low in our study. However, pathologies that have been determined in our study serve as severe morbidity causes and lead to the risk of disability. Therefore, we believe that the use of whole-body CT on the right patients is of great importance.
Asha et al. 11 found that WBCT was associated with an increase in radiation exposure: there was an 8% absolute risk increase of exposure to high radiation dose. Ronnie et al. found that a WBCT scan confers an appreciable risk of malignancy to patients, 42% of whom required no scan at all in his series, with only 16% demonstrating radiological evidence of polytrauma. Ronnie et al. 17 suggest that large numbers of patients are being subjected to unnecessary radiation with its long-term risk of future life-threatening consequences of malignancy. For these reasons, the risk of radiation should be avoided by reducing the number of unnecessary WBCT scans by choosing the right patient, especially in the children.
Patient population of the REACT study includes trauma patients who have life-threatening vital problems, who are tachypneic or bradypnic, tachycardic, hypotensive, whose estimated external blood loss is more than 500 mL, whose GCS is less than 13, and who has abnormal pupil reaction. Moreover, patient admission criteria are defined as having one of the injury mechanisms, such as flail chest, open chest or multiple rib fractures, severe abdominal injury, pelvic fracture, unstable vertebral fractures/spinal cord compression, suspected clinical diagnosis such as fracture in at least two long bones, falling from 3-m high, being thrown from the vehicle, casualties or critically wounded patient in the same vehicle, and wedged or trapped chest/abdomen.14,18 In addition to all these criteria mentioned above, we also used the need for mechanical ventilation, detection of free fluid in the FAST, hypoxia, and SI, and we observed that they composed high-risk criteria in determining multiple trauma patients. Our study is different than the studies in the literature as we endeavored to set new risk criteria in determining multiple trauma patients and our study involves new findings. If these high-risk criteria set in our study had also been used in the REACT study, a difference in terms of mortality rates might have been detected in the patients who had been given whole-body CT compared to the patients who had not been given whole-body CT. In this regard, the importance of selecting particularly the right patient has also been emphasized in the REACT study. 14 Furthermore, prospective studies with more patients involving high-risk criteria that we had set in our study are needed in the literature. Such similar studies will reveal more accurate results in determining the effects of whole-body CT over mortality. Moreover, these studies will be more effective if they do not only examine differences in terms of mortality between patients who are given whole-body CT and patients who are not given whole-body CT, but also involve overlooked diagnosis, morbidity, and medico-legal considerations.
Limitations
Our study is retrospective. We could not compare the patients which managed without WBCT scan as a control.
Conclusion
High-risk group in terms of multiple traumas involves the need for mechanical ventilation in trauma patients, positivity in the FAST, GCS being under 13, hypoxia, tachycardia, positivity in SI, and extravehicular car injuries as a mechanism. This patient group should be underwent whole-body CT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
University of Ege open all medical data to researchers of Ege Ethical Committee approval.
Informed consent
It is retrospective study and we had Ethical Committee approval, so no need for the informed consent.
Ethical approval
University of Ege ethical approval committee permission date 16 May 2016, number: 16-4.1/15.