
Abstract
Introduction:
Recreational use of methamphetamine is increasing worldwide, but epidemiology studies from Asia are lacking. We aimed to characterise the trends, drug use pattern, clinical presentations and health services utilisation of acute methamphetamine toxicity presenting to emergency departments and the current practice of emergency department psychosocial interventions in Hong Kong.
Methods:
This was a secondary analysis of a retrospective study on emergency department patients reported to the Hong Kong Poison Information Centre between 2010 and 2019 for acute toxicity related to recreational methamphetamine use. We studied the trend using a negative binominal regression model.
Results:
During the study period, 1225 episodes (involved 979 patients; 68.9% men; with a median age of 33.0 years) were reported. Acute methamphetamine toxicity did not increase significantly (odds ratio = 1.10, 95% confidence interval = 0.86–1.40, p = 0.46). Polysubstance abuse predominated. Many patients developed hypokalaemia (24.0%), rhabdomyolysis (17.2%), acute kidney injury (9.4%) and myocardial injury (4.7%); psychotic symptoms including auditory hallucination (23.8%) and paranoid delusion (21.1%); various acute behavioural disturbances and injuries. Overall, 66 patients required intensive care and 14 patients died. Only a minority of the patients were referred to social workers and voluntary drug treatment and rehabilitation services.
Conclusion:
Methamphetamine has a significant impact on physical and mental health in Hong Kong. Our findings highlight the need for screening for hypokalaemia, rhabdomyolysis, acute kidney injury, myocardial injury and psychosis in methamphetamine users and support policies that address polysubstance abuse, prevent drug use through continued public education and strengthen the referral system by integrating substance abuse services at the emergency department.
Introduction
Methamphetamine, an N-methylated derivative of amphetamine, is a highly addictive psychostimulant. 1 Commonly known as ‘Ice’ because of the crystalline appearance of its hydrochloride salt, methamphetamine is popular among recreational drug users for its euphoric, 1 anorectic (particularly in female users) 2 and aphrodisiac effects (especially among men who have sex with men (MSM) in ‘chemsex’). 3 Over the past decade, recreational use of methamphetamine has been increasing in the United States, Australia, East and South-East Asia.1,4 In Hong Kong, according to the Central Registry of Drug Abuse (CRDA), which collects voluntary reporting from law enforcement agencies, treatment and welfare agencies, tertiary institutions, hospitals and clinics, methamphetamine has become the most common soft drug of abuse. 5 It was also the most prevalent illicit drug found in drugs seized by law enforcement and urine samples from offenders/probationers in the city from 2016 to 2018. 6
Methamphetamine use can cause serious acute toxicity, especially among chronic users with compulsive ‘binge’ consumption because of drug tolerance. Unreliable dosing and concurrent consumption of other drugs further increase the risk. Methamphetamine selectively enhances the release and inhibits the reuptake of dopamine, and to a lesser extent, serotonin and noradrenaline. Acute methamphetamine overdose can result in excessive stimulation of these monoamine pathways in the central nervous system (CNS), producing the typical presentation of acute paranoid psychosis, adrenergic storm and hyperthermia.1,7 –10 Severe poisoning can lead to seizure, coma, intracranial bleeding, myocardial ischaemia, dysrhythmia, shock, acute kidney injury (AKI), rhabdomyolysis, multi-organ failure or even death.1,11–16 Patients with acute methamphetamine toxicity often present to the emergency departments (EDs),17,18 for associated mental illness, trauma, skin- and dental-related problems 19 and behavioural disturbances. 7 They accounted for 159,000 ED visits annually in the United States 20 and 29,700–151,800 additional ED presentations in Australia. 21
Despite its harms and frequent ED presentations, large-scale studies on the epidemiology of acute methamphetamine toxicity from Asia are lacking. Furthermore, psychosocial interventions initiated at the ED that might help reduce future drug-related ED re-attendance, such as referral to voluntary drug treatment and rehabilitation services provided by non-governmental organisations (NGOs), remain unclear. We conducted this study (1) to characterise the trends, patterns of drug use, clinical features and outcome and health services utilisation of patients presenting to EDs with acute methamphetamine toxicity in Hong Kong over a 10-year period from 2010 to 2019 and (2) to evaluate the current practice of ED psychosocial interventions for methamphetamine users.
Methods
This was a secondary analysis of a retrospective study on consecutive patients with acute psychoactive drug toxicity reported to the Hong Kong Poison Information Centre (HKPIC) by public accident and emergency departments (EDs) in Hong Kong between 1 January 2010 and 31 December 2019. The details of the study method have been reported elsewhere. 22 Ethics approved with a waiver of informed consent was sought before the study. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines in reporting the study findings. 23
The HKPIC is the only poison centre in Hong Kong that provides a round-the-clock phone consultation service to healthcare professionals and collects epidemiological data on poisoning voluntarily reported by all local public EDs. Data on each poisoning case, received from either consultation or reporting, are entered into the Poison Information and Clinical Management System (PICMS) by trained staff with routine verification by clinical toxicologists. 24 This database contains territory-wide data representative of acute methamphetamine toxicities treated in all local EDs.
Study population
All patients with acute toxicity related to recreational methamphetamine use within the study period were included. Drug use, including concomitant psychoactive substance exposure, was reviewed by the first author and defined based on clinical diagnosis of the attending clinical team and the poison exposure record in the HKPIC, with or without confirmation by a urine toxicology immunoassay or laboratory toxicology screen. Exclusion criteria included (1) unintentional exposure; (2) malicious exposure; (3) ‘body packing’ (‘body stuffer’ who had swallowed drugs hastily to avoid law enforcement arrest were still included as they were considered likely to be recreational drug users); (4) unrelated cases whose clinical presentations were explained by alternative medical or psychiatric diagnoses or social reasons; (5) confirmed non-exposure with objective evidence that the initially suspected involvement of methamphetamine had not occurred and (6) non-ED cases.
All eligible cases were identified from the PICMS using poison code search. Electronic medical records, including ED record, discharge summary and psychiatrist consultation notes, were then retrieved from the Clinical Management System (CMS) of the Hospital Authority for review. The CMS is a central data repository that contains all clinical, laboratory and treatment data of every patient treated in all public hospitals in Hong Kong. Data were collected by two research assistants independently in parallel based on a standardised data entry coding manual. Any discrepancies were resolved by the principal investigator. Patient demographic data, the type, time and route of drugs used, data on clinical and laboratory parameters, associated problems (e.g. injuries), end-organ toxicities, interventions (e.g. administration of antidote), clinical outcome and psychosocial interventions (including psychiatric consultation, referral to social workers and NGO drug treatment and rehabilitation services, etc.) were collected.
We evaluated the whole clinical course of individual cases from presentation to hospital discharge or death. The outcome of acute poisoning was classified by clinical toxicologists according to the American Association of Poison Control Centers’ (AAPCC) National Poison Data System into five categories: no effect, mild effect, moderate effect, major effect or death. 25
Data analysis
Because of a lack of previous studies in Hong Kong, a priori sample size calculation was not performed. We analysed the data using descriptive statistics with no imputation of missing values. We calculated the median annual incidence of methamphetamine-related visits per 100,000 ED attendances. We also determined the annual rates of methamphetamine-related ED visits per 100,000 population based on the mid-year population data from the Census and Statistics Department. We then evaluated the time trend using a negative binomial regression model to allow for overdispersion, with the logarithm of total ED attendance of the same year as the offset term. The Spearman correlation between the number of toxicities reported to the HKPIC and the number of reported methamphetamine users in CRDA and the market value of the drug seized by the Hong Kong Customs and Excise Department of the same year were determined.
For data on the patterns of drug use, clinical presentations, outcome and health resources utilisation, we summarised categorical variables using proportions and continuous variables using mean values with standard deviations or medians with interquartile ranges (IQRs), as appropriate. We further analysed the episodes that involved methamphetamine only as a subgroup to separate the effect of methamphetamine from other co-ingestions. The Statistical Package for the Social Sciences (SPSS) for Window version 27.0 (IBM Corp., Armonk, NY, USA) was used for data analysis, with a two-tailed p-value < 0.05 considered statistically significant.
Results
Over the study period, 1225 episodes of acute methamphetamine toxicity involving 979 patients were reported from local EDs to the HKPIC. Among these, 603 episodes of 501 patients involved methamphetamine only.
The median annual number of episodes of acute methamphetamine toxicity was 120 (IQR = 93–150), corresponding to 5.64 (IQR = 4.14–6.72) per 100,000 ED attendances. The median annual incidence rate of methamphetamine-related ED visits was 1.63 (IQR = 1.31–2.06) per 100,000 population. Acute methamphetamine toxicities did not increase significantly during the study period (odds ratio (OR) = 1.10, 95% confidence interval (CI) = 0.86–1.40, p = 0.46). The number of acute toxicities reported to the HKPIC was significantly correlated with the number of reported methamphetamine users in the CRDA (Spearman’s rho 0.82, p = 0.004), but not with the market value of methamphetamine seized by law enforcement of the same year (Spearman’s rho 0.33, p = 0.35).
Table 1 shows the demographic features of the reported ED episodes of acute methamphetamine toxicity. The median age of the patients was 33.0 years (IQR = 27.0–40.0 years). The majority of episodes involved men (68.9%) and 279 episodes (22.8%) involved patients who received social allowance. Ambulance transportation and police involvement were required in 931 (76.0%) and 416 episodes (34.0%), respectively. Overall, 37 episodes involved non-local residents (e.g. tourists), 9 episodes involved pregnant patients and 52 episodes involved MSM.
Demographic characteristics and pattern of drug use of methamphetamine users.
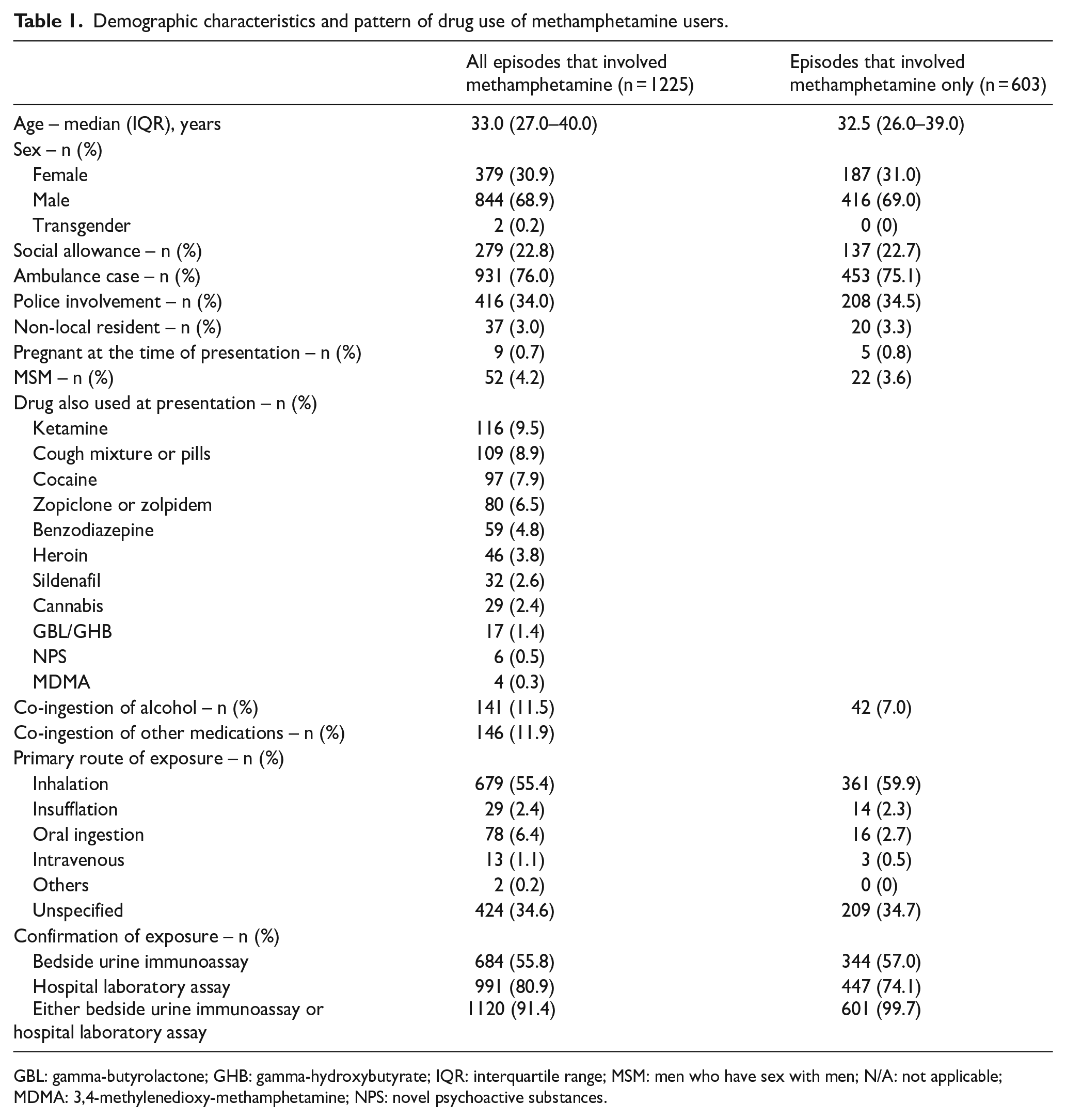
GBL: gamma-butyrolactone; GHB: gamma-hydroxybutyrate; IQR: interquartile range; MSM: men who have sex with men; N/A: not applicable; MDMA: 3,4-methylenedioxy-methamphetamine; NPS: novel psychoactive substances.
The pattern of drug use is shown in Table 1. More than half of the episodes involved polysubstance use, with methamphetamine and ketamine being the commonest combination of illicit drugs (n = 116, 9.5%). Table 2 shows previous drug use pattern and co-morbidities. Over 80% had a previous history of recreational drug use and 73.3% had used methamphetamine in the past. A significant proportion had a history of drug-induced psychosis (44.6%), and some patients had schizophrenia, antisocial and borderline personality disorder and psychiatric follow-up. However, among those who were receiving psychiatric treatment, only half were compliant. Only a minority had received detoxification treatment (20.7%), social worker follow-up (27.2%) and NGO drug treatment and rehabilitation services before (8.9%).
Past drug use pattern, psychiatric, medical and treatment history of methamphetamine users.
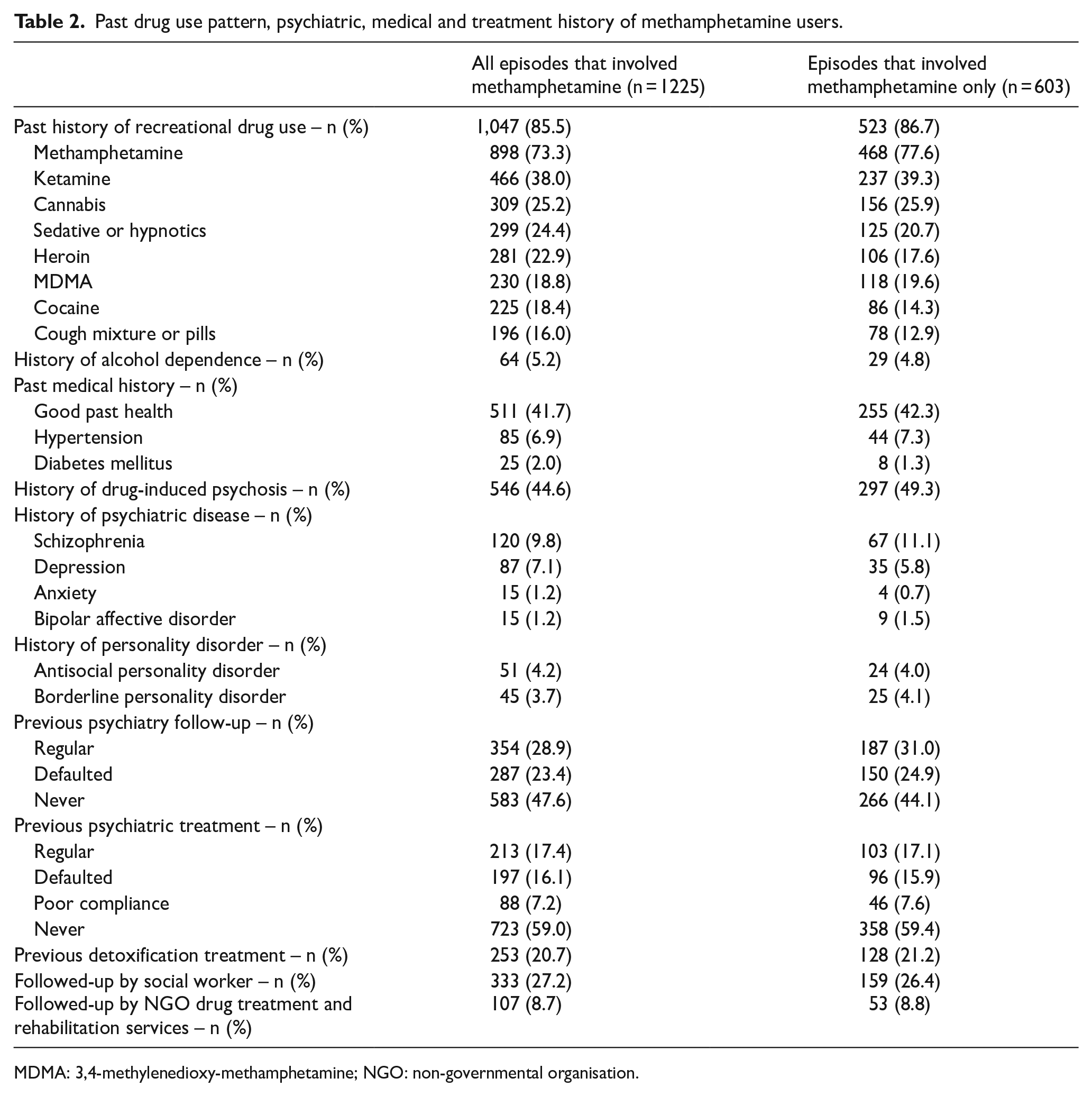
MDMA: 3,4-methylenedioxy-methamphetamine; NGO: non-governmental organisation.
Table 3 shows the clinical presentations at the time of ED presentation. Most patients were triaged to a higher acuity with prominently neurological and cardiovascular manifestations compatible with sympathomimetic toxidrome. Notably, many patients had psychotic features such as auditory hallucination (23.8%) and paranoid delusion (21.1%). Also, around one-fifth had hypokalaemia. Rhabdomyolysis (creatine kinase > 1000 IU/L) was common (17.2%). AKI, metabolic acidosis and myocardial injury were seen in 9.4%, 4.3% and 4.7% of the episodes, respectively. Other severe complications included ventricular dysrhythmia (n = 2), acute myocardial infarction (n = 3), heart failure (n = 1), coma (n = 36), seizure (n = 33), acute ischaemic stroke (n = 3), acute haemorrhagic stroke (n = 2), respiratory failure (n = 17) and severe hyperthermia with a temperature ⩾40°C (n = 13). Cardiac arrest occurred in 16 episodes.
Clinical presentations of acute methamphetamine toxicity in the emergency department.
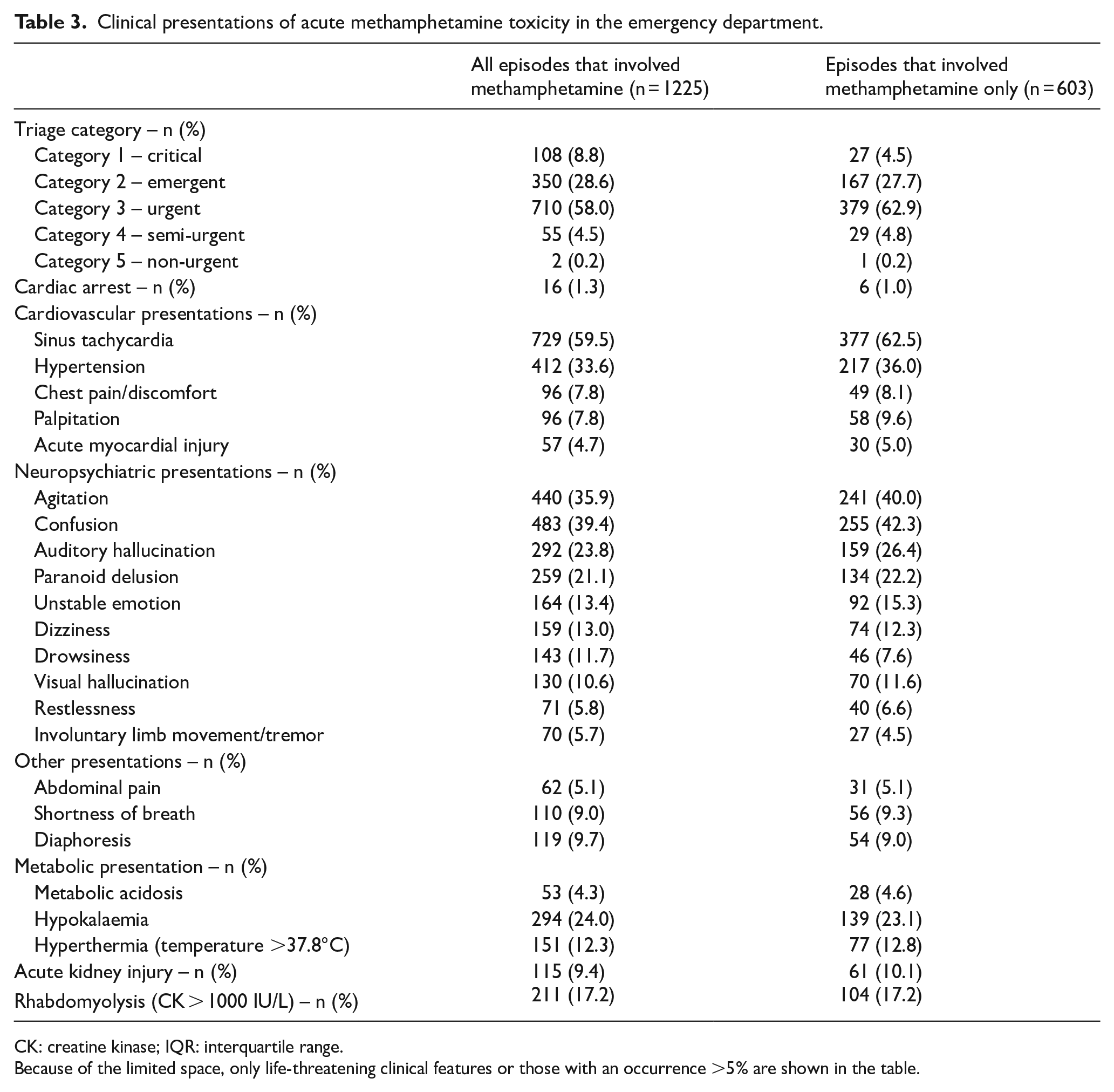
CK: creatine kinase; IQR: interquartile range.
Because of the limited space, only life-threatening clinical features or those with an occurrence >5% are shown in the table.
Disorganised behaviours, as shown in Table 4, were frequent with many methamphetamine users found wandering, lying on the floor, running naked or exposing their body indecently in public areas before ED arrival. Many patients had concomitant self-harm behaviours (16.4%), including a few extraordinary acts of self-mutilation (e.g. self-amputation of genitalia with broken glass in one case). A number of patients were brought to the ED because of a gesture of attempting to jump from a building (4.0%) and four patients did jump, resulting in major trauma and multiple injuries. Although not consistently documented, many drug users either acted impulsively because of their frustration with the psychotic symptoms or misjudged the risk of their reckless behaviour under drug influence. Equally prominent were violent behaviours to others during their acute presentation (15.8%), with the patient’s family members being the most common target of physical violence. Associated injuries were also common (14.9%) among users.
Injuries and behavioural problems associated with methamphetamine use.
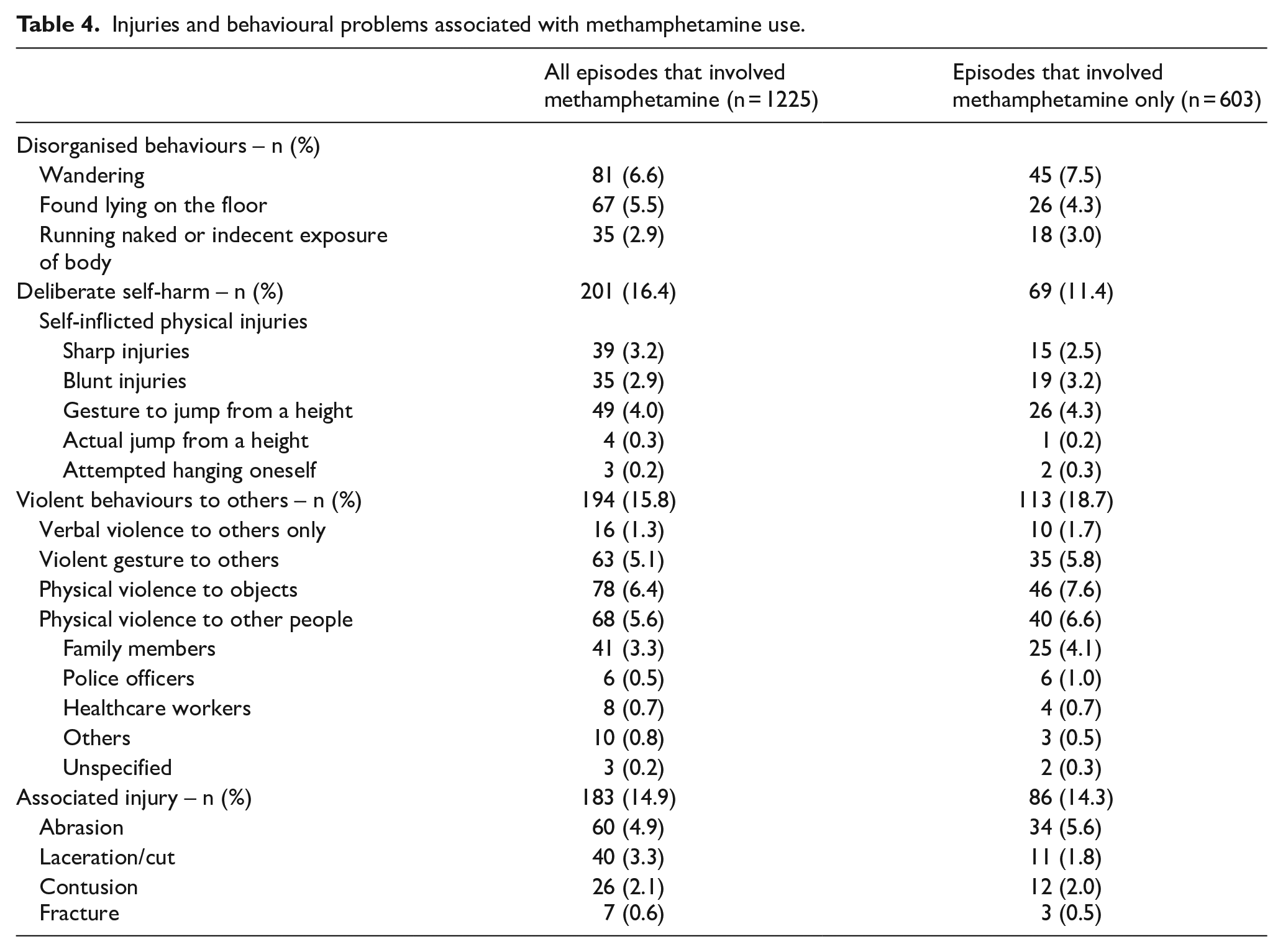
Table 5 summarises the clinical management. Supportive treatment was the mainstay. Many patients required physical (44.2%) or chemical restraint (31.0%) or both in the ED and in the hospital. Diazepam was the most frequently used for chemical restraint, followed by midazolam and haloperidol. Gastrointestinal decontamination and antidotes were rarely needed. Potassium replacement was required in 71 episodes and sodium bicarbonate (for urine alkalisation or metabolic acidosis) was administered in 34 episodes. A small number of patients required organ support, including intubation and mechanical ventilation (n = 47), inotrope (n = 18), renal replacement therapy (n = 7), antiarrhythmic and electrical therapy (n = 4) and extracorporeal membrane oxygenation (n = 1). Cardiopulmonary resuscitation was performed in 13 episodes. According to AAPCC classification, 325 (26.5%) patients had moderate effects, 44 patients (3.6%) had major effects and 14 (1.1%) patients died of acute toxicity.
Treatment of acute methamphetamine toxicity in the emergency department and hospital.
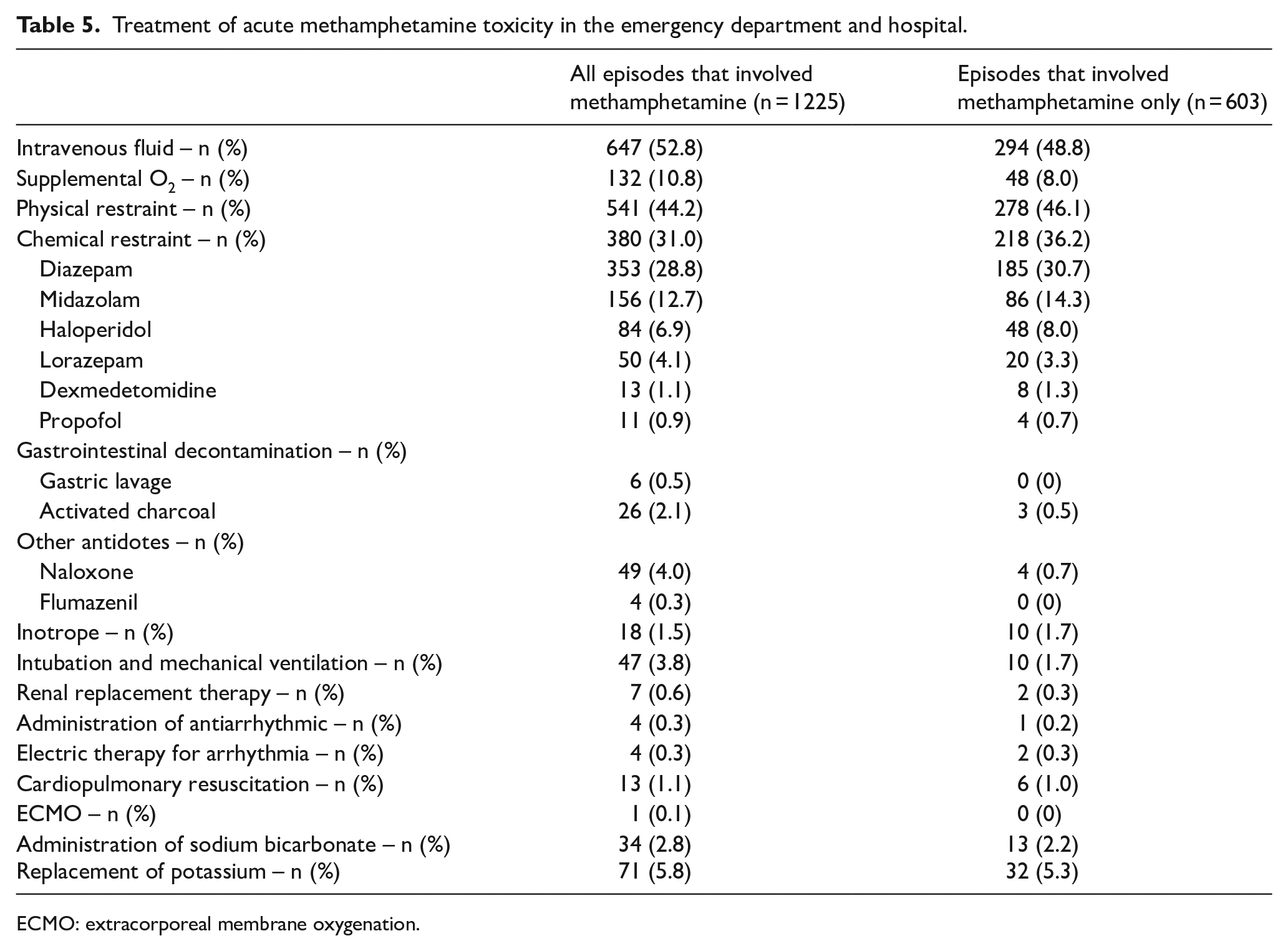
ECMO: extracorporeal membrane oxygenation.
As for patient disposition, 4.9% were discharged directly from the ED and 14.0% left against medical advice (Table 6). The majority were managed in the emergency medicine ward (EMW) or observation ward by emergency physicians and nurses (63.6%). Around a third were admitted to the general ward or psychiatric ward and 66 required intensive care unit (ICU) care (5.4%). The median lengths of stay in EMW, general wards and psychiatric wards were 19.6 h, 2.7 days and 15.8 days, respectively. As for ED-initiated psychosocial interventions, 70.9% required urgent psychiatric consultation and 28.1% referral to outpatient psychiatric service. Only 18.6% were referred to social worker and 4.8% to NGO drug treatment and rehabilitation services upon hospital discharge.
Patient disposition and clinical outcome of methamphetamine users.
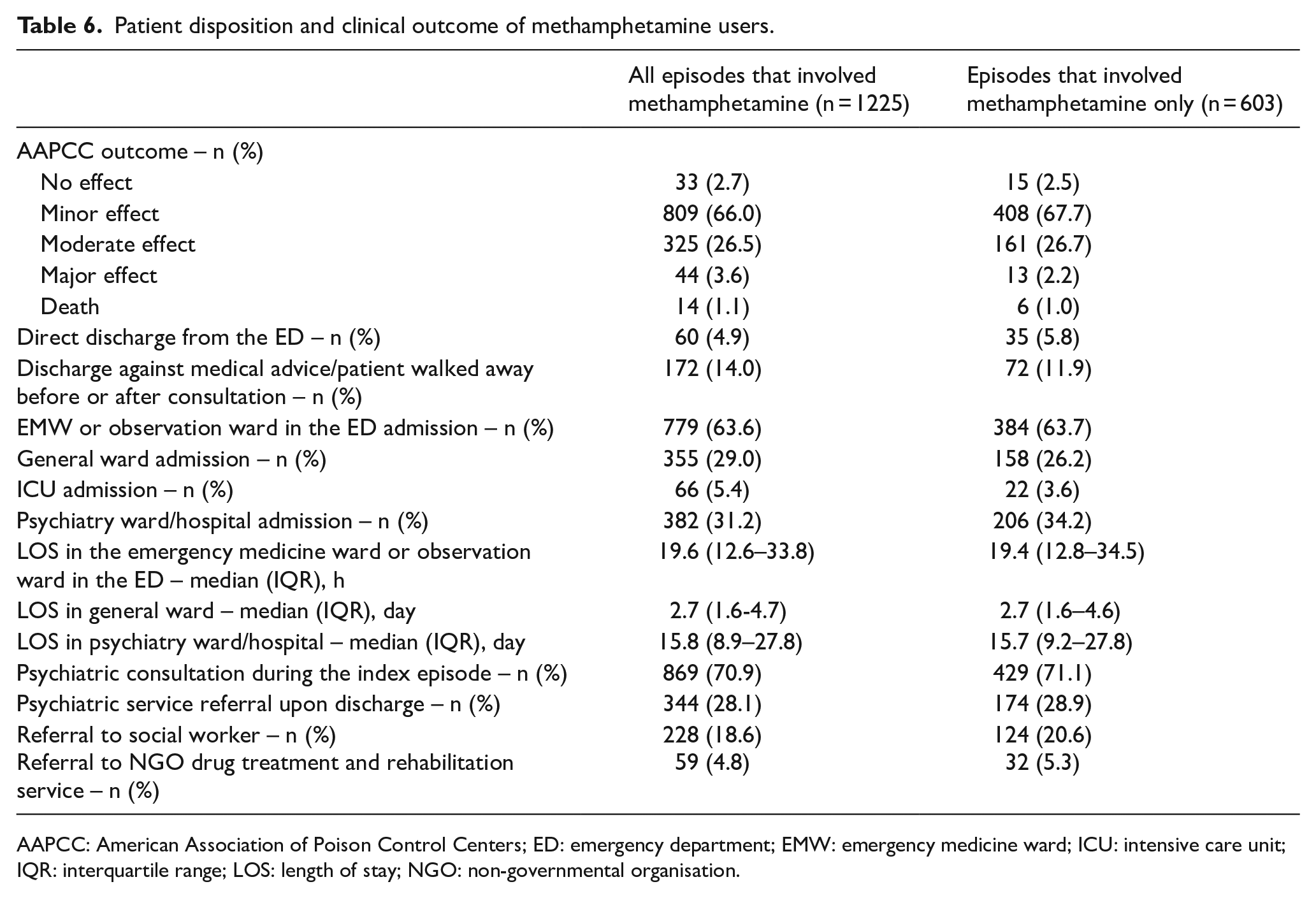
AAPCC: American Association of Poison Control Centers; ED: emergency department; EMW: emergency medicine ward; ICU: intensive care unit; IQR: interquartile range; LOS: length of stay; NGO: non-governmental organisation.
Subgroup analysis of the episodes that involved only methamphetamine showed similar patterns of trend, correlation, demographic, clinical and outcome characteristics. The findings are shown in the respective tables.
Discussion
Although the reported number of acute methamphetamine toxicities has not increased significantly in Hong Kong over the last decade, a significant proportion of users developed end-organ toxicities, psychotic symptoms, acute behavioural disturbances and injuries, with 14 deaths (1.1%) and 66 ICU admissions (5.4%) identified in this study. Only a minority of methamphetamine users were referred to social workers and NGO drug treatment and rehabilitation services upon ED or hospital discharge.
The median annual incidence rate of methamphetamine-related ED visits in Hong Kong was lower than that in the United States (1.63 vs 33.0 per 100,000 population). 20 Similar population-level estimate has not been published in Europe or in other Asian countries or cities. In 2017, the European Drug Emergency Network reported 864 cases of amphetamine misuse from 31 sentinel hospitals in 21 European countries. 26 The difference in incidence can be explained by differences in drug supply and consumption, access to healthcare and method of data collection. This study provides population-level estimates in Asia for benchmarking and longitudinal monitoring of the impact of drug-control interventions.
It is interesting to see the significant correlation between the HKPIC data and CRDA statistics. The number of acute methamphetamine toxicities reported to the HKPIC was roughly one-tenth of the number of reported methamphetamine users in the CRDA. There was a lack of correlation between the HKPIC data and drug seizure data. One possible explanation is that some of the methamphetamine seized might come from shipments transiting Hong Kong, which were not intended for local market. 27
As for the pattern of drug use, polysubstance use predominated. From chart review, we found that many drug users used methamphetamine along with other drugs to potentiate the desired effect or to reduce the undesirable effects of methamphetamine, such as using benzodiazepine or zopiclone to reduce insomnia. Of note, a number of heroin users used methamphetamine to create synergistic highs, balance drug effects or curb opioid withdrawal,6,28 a rising combination also seen in the United States as ‘twin epidemics’ of opioid and methamphetamine abuse. 29 This combination poses a greater risk because of the more complicated presentations (co-occurring opioid and sympathomimetic syndromes). Many drug users also used methamphetamine to replace ketamine (because of ketamine-associated bladder dysfunction) and heroin (as an inexpensive substitute). 29 These findings highlight the importance of continued monitoring to match drug-control policy and clinical management with the prevailing pattern of drug use.
Similar to previous studies, a significant proportion of methamphetamine users in this study had a history of recreational drug use, psychiatric co-morbidities and psychotic features.9,17,30 Methamphetamine has been associated with a higher risk of schizophrenia than cocaine, opioids and alcohol except cannabis. 31 Increase in frequency, duration and severity of methamphetamine use are associated with a higher risk of psychotic symptoms,32,33 which might last for months even after drug abstinence. 34 It is necessary to screen for psychotic symptoms when methamphetamine users present to the ED with acute toxicity.
ED patients with new-onset psychosis or violent behaviours should also be screened for methamphetamine use. Notably, methamphetamine users generally had a poor compliance with outpatient psychiatric follow-up appointment and treatment. Only a minority had received detoxification treatment, social service and NGO drug treatment and rehabilitation service in the past and were referred to these services upon ED or hospital discharge. These findings highlight the need to strengthen the current referral system by integrating and bringing drug service providers from different sectors to the patients while they are still in the hospital to maximise engagement. There is also a need to develop strategy to reinforce patient compliance to treatment.
Overall, the clinical toxicities were similar to those reported in other ED-based studies7 –10,17 with a comparable triage acuity.9,17 This study adds to the literature by showing that up to one-fifth of the patients developed hypokalaemia, which is under-reported before. Hypokalaemia can be explained by β2-adrenergic stimulation causing intracellular shift of potassium and activation of Na-K-ATPase. Rhabdomyolysis, AKI and myocardial injury occurred in many methamphetamine users, as shown in previous studies.7,12 –15 These complications cannot be reliably predicted with history and physical examination alone. The presenting electrocardiogram (ECG) of those with myocardial injury can be non-diagnostic. 12 We recommend routine checking of serum potassium, creatinine, creatine kinase and cardiac troponins for patients presenting to the ED with acute methamphetamine toxicity. We concur with Richards et al. 14 that patients with unexplained rhabdomyolysis should be screened for methamphetamine exposure.
Another challenge ED staff need to face is the behavioural disturbances. Methamphetamine use is often associated with agitation, psychotic symptoms,8,17,35 violent behaviours and aggression,7,9,17,29,36 requiring chemical and/or physical restraints,7,17,37 police and ambulance service,7,9,17,30 and is resource intensive.7,17,19,37,38 Compared with other drugs, methamphetamine users are more agitated, violent and aggressive,30,36 posing a higher risk to staff and other people around. Greater methamphetamine consumption has been associated with higher self-reported impulsivity 39 and alcohol co-ingestion may further increase aggression. 40 Consistent with previous studies, methamphetamine-based violence commonly involved patient’s family members, 41 but healthcare workers, paramedics and police are also at risk. There is a need to protect patients’ cohabiting family members and staff in case of aggression.
In keeping with previous studies, in Hong Kong, the majority of acute methamphetamine toxicities were managed in the EDs with symptom-directed supportive treatment.7,8,17 Physical and chemical restraints were applied at similar rates as reported elsewhere. 17 Most cases of rhabdomyolysis and AKI responded to intravenous fluid or alkaline diuresis,7,14,15 but a few cases required renal replacement therapy. The overall ICU admission rate, death rate and ED length of stay were comparable with those previously reported.7,17
Limitations
This study had several limitations. First, information bias and missing data are inherent weaknesses of its retrospective design. It was likely that only the main clinical features were documented and we could only assume their absence when they were not. Second, the HKPIC reporting mechanism might miss milder cases. We believe we have captured the majority of severe cases that required HKPIC consultation. Also, the reporting mechanism had been consistent over the study period and the trend analysis should be robust. Third, there was no standard criterion for the determination of the relationship between drug use and ED visit. We could only rely on the clinical judgement of the treating physicians with subsequent vetting during data collection. Forth, not all cases underwent toxicology screening since there was no standardised drug screening protocol in different EDs. Given the low self-reporting rate of drug use, diagnosis could be missed if history was not forthcoming or if the clinicians did not consider methamphetamine toxicity in their differential diagnosis. Despite these limitations, this study provides population-level estimates of the incidence from an Asian city, longitudinal data for trend analysis and real-world clinical data to inform clinical management.
Conclusion
Although the reported number of acute methamphetamine toxicity has not increased significantly in Hong Kong over the last decade, its impact on physical and mental health is significant. Our findings highlight the need for screening for hypokalaemia, rhabdomyolysis, AKI, myocardial injury and psychosis in ED patients with acute methamphetamine toxicity. Drug-control policies that address polysubstance use, prevent drug use through continued public education and strengthen the referral system by integrating substance abuse services at the ED are important to reduce harm.
Footnotes
Acknowledgements
The authors thank Ms Annie Chan and Ms Agatha Ho for their help in data collection and the staff in HKPIC for their help in data retrieval.
Author contributions
R.P.K.L. conceived and designed the study. R.P.K.L. acquired the data. R.P.K.L. and E.H.Y.L. analysed and interpreted the data. R.P.K.L. drafted the manuscript, and R.P.K.L., C.K.C., M.L.T., M.S.H.T. and T.H.R. critically revised the manuscript for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Beat Drugs Fund from the Narcotics Division of the Security Bureau of the Government of the Hong Kong Special Administrative Region (BDF190053). The funder had no role in study design, data collection/analysis/interpretation or manuscript preparation.
Availability of data
The study data are not available because the authors did not obtain permission to share date from the research ethics committees.
Informed consent
Informed consent from the recruited subjects was waived by the research ethics committees because of the retrospective nature of the study and anonymity in the data analysis.
Ethical approval
The study was approved by the Institutional Review Board of The University of Hong Kong/Hong Kong West Cluster of the Hospital Authority (HA; reference no. UW 20-597) and the Research Ethics Committee of the Kowloon Central/Kowloon East Cluster of the HA (reference no. KC/KE-20-0270/ER-2).