
Abstract
Background:
Evaluation of chest pain patients in emergency departments to distinguish between high-risk patients who require admission and low-risk patients who can be managed as outpatients is a challenging task.
Objective:
The aim of this study was to evaluate the efficacy of Observation Ward Short Stay Evaluation Service for Chest Pain Protocol to identify and safely discharge low-risk patients with low incidence of major adverse cardiac events within 30 days.
Methods:
This was a single center prospective observational study, conducted from 1 March 2016 to 31 August 2016 at the Emergency and Trauma Department, Hospital Kuala Lumpur, Kuala Lumpur. Observation Ward Short Stay Evaluation Service for Chest Pain Protocol was used to evaluate patients presented with chest pain or angina equivalents. The components involved Thrombolysis in Myocardial Infarction (TIMI) score, serial electrocardiograms, high-sensitivity cardiac troponin T, and exercise treadmill test. Low-risk patients were patients with TIMI < 2, normal serial electrocardiogram, high-sensitivity cardiac troponin T ≤ 14 ng/L, and negative exercise treadmill test. If anyone of the components was not fulfilled patients were considered as high risk, and they were either admitted or referred to clinic for further intervention. Low-risk patients were allowed for discharged. All patients were followed-up in 30 days for any incidence of major adverse cardiac events.
Results:
Totally, 174 patients were studied. Observation Ward Short Stay Evaluation Service for Chest Pain Protocol managed to discharge 102 (58.6%) patients, and 84 (82.4%) of them underwent exercise treadmill test. About 46 (54.8%) patients had negative exercise treadmill test, whereas 38 (45.2%) patients had either positive or inconclusive exercise treadmill test, and they were referred to physician clinic for further cardiac assessment. None of the patients with negative exercise treadmill test developed major adverse cardiac events in 30 days. The sensitivity and the negative predictive value (NPV) of Observation Ward Short Stay Evaluation Service for Chest Pain Protocol were both 100%.
Conclusion:
Observation Ward Short Stay Evaluation Service for Chest Pain Protocol can be applied in emergency departments to identify and safely discharge patients with low risk of major adverse cardiac events in 30 days.
Introduction
Patients with chest pain consist of approximately 5% to 10% of annual presentations to the emergency departments.1,2 One of the life-threatening conditions for urgent intervention is acute coronary syndrome (ACS). According to the guidelines, patients with acute chest pain should be stratified into high, intermediate, and low risk and managed accordingly.3–5 The Malaysia clinical practice guidelines of the management of unstable angina (UA) and non-ST elevation myocardial infarction recommend that low-risk patients can be managed as outpatients with oral antiplatelet and for non-invasive cardiac assessment. 3 However, due to the long waiting list, most of these cardiac assessments can only be performed within a few months.
An ideal risk stratification approach in an emergency department should be able to identify all high-risk and low-risk patients. High-risk patients should be admitted for further intervention, whereas low-risk patients can be treated as outpatients to avoid ward overcrowding and access block. Studies showed that by application of an accelerated diagnostic protocol (ADP) which incorporated risk stratification scoring system, electrocardiography, and cardiac enzyme was able to identify a significant percentage of low-risk patients who could be safely treated as outpatients.6,7 A local study was conducted in the Emergency and Trauma Department Hospital Kuala Lumpur (ETDHKL) to assess the efficacy of an ADP in the department in evaluation of acute chest pain patients. 8 It was conducted from 1 March 2014 to 31 July 2014. The ADP consists of TIMI score, serial ECGs, and high-sensitivity cardiac troponin I. Around 120 patients were studied, and 82.5% were found to be at low risk and allowed for discharge. About 2% of the low-risk patients developed major adverse cardiac events (MACEs) at 30 days. This gave rise to a sensitivity of 90.48% and negative predictive value (NPV) of 97.98%. These were relatively low compared to other large-scale multicenter studies which managed to achieve high sensitivity and NPV of > 99%.6,7,9 A survey regarding the acceptable missing rate of ACS in emergency departments was done by Than et al. and most emergency physicians only accept a missing rate of 1% or less. 10 In order to improve the diagnostic approach in ETDHKL, the previous ADP has been revised and replaced with a new protocol which is Observation Ward Short Stay Evaluation Service for Chest Pain (OBSSES Protocol). This study was to evaluate the efficacy of OBSSES Protocol to identify and safely discharge low-risk patients with low incidence of major adverse cardiac events (MACEs) within 30 days. The Definition of MACEs was listed in Table 1.
Major adverse cardiac events.
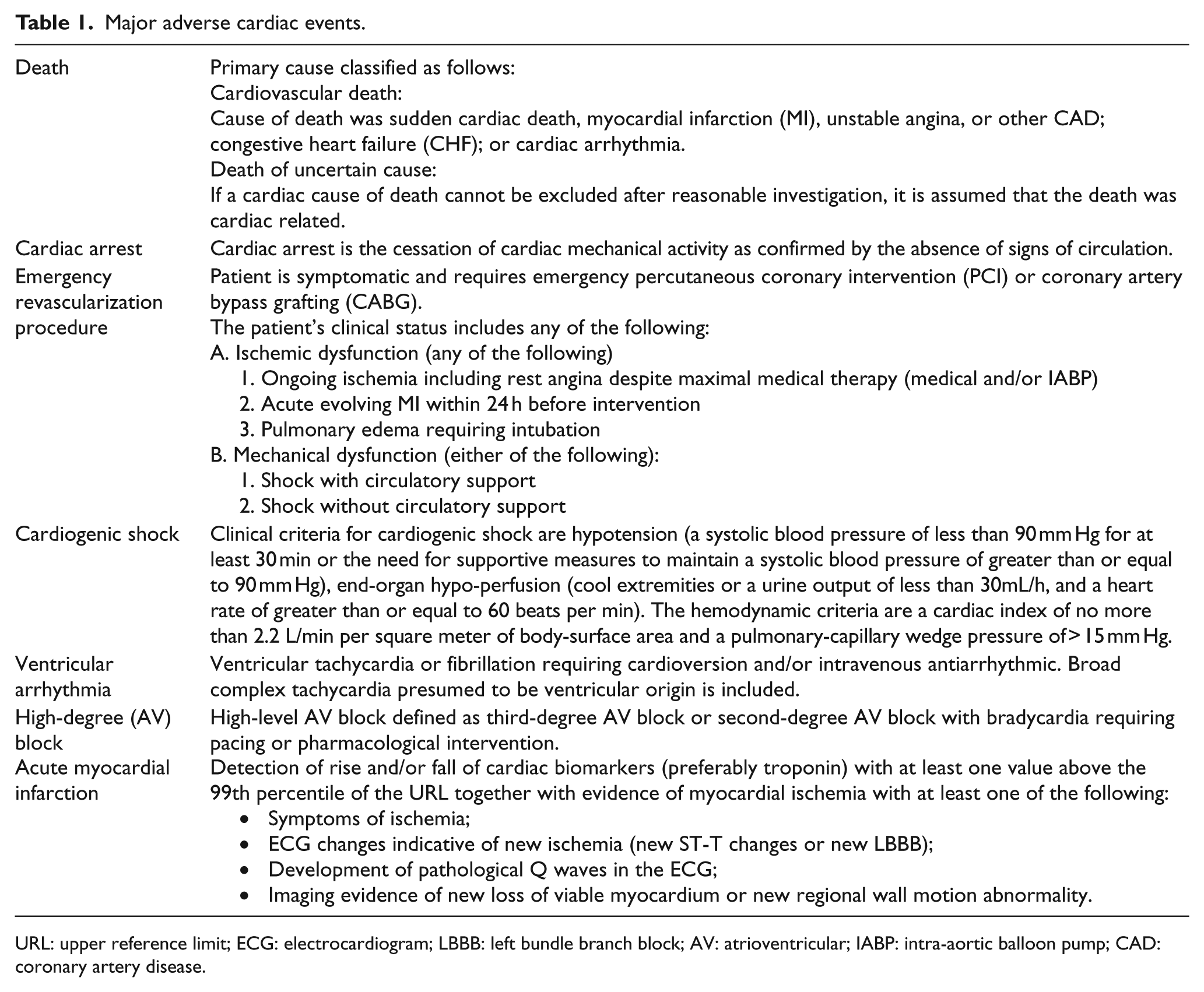
URL: upper reference limit; ECG: electrocardiogram; LBBB: left bundle branch block; AV: atrioventricular; IABP: intra-aortic balloon pump; CAD: coronary artery disease.
Methods
This was a prospective, observational, single-center study, which was conducted in ETDHKL, Malaysia from 1 March 2016 till 31 August 2016, and was approved by the Medical Review & Ethics Committee (MREC), Ministry of Health of Malaysia in 2016 (Approval Code: NMRR-16-24-28858). Hospital Kuala Lumpur is the largest hospital in the Ministry of Health of Malaysia. It is a government tertiary referral hospital with an average of 350,000 emergency department visits per year.11,12
Components of OBSSES Protocol included TIMI score, serial ECG, high-sensitivity cardiac troponin T (hs-cTnT), and exercise treadmill test (ETT) within 1 week. Low-risk patients were patients with TIMI score < 2, normal/inconclusive serial ECG findings, hs-cTnT > 14 ng/L, and negative ETT. Low-risk patients were expected to have low risk of MACEs in 30 days, and allowed for discharge. High-risk patients were patients with either TIMI score ≥ 2, serial ECG shown ischemic/evolutional changes, hs-cTnT > 14 ng/L, or positive/inconclusive ETT. High-risk patients were expected to have high risk of MACEs in 30 days, and they were either admitted or referred to physician clinic for further evaluation.
The sample size of this study was calculated based on the need for adequate sensitivity. 13 The aim of this study was to achieve a sensitivity of at least 99% because this is the level of sensitivity most emergency physicians were comfortable with. 10 A sample size of about 121 patients was required to achieve an adequate sensitivity of at least 99% (Appendix 1).
The sampling method of this study was a convenient method which dependent on the availability of the investigators. Patients who were 18 years and above with a chief complaint of non-traumatic chest pain, or angina equivalent symptoms, hemodynamically stable, and fulfilled all the inclusion criteria, and consented were recruited into the study. Patients with new onset angina, prolonged angina at rest, crescendo angina, ST elevation myocardial infarction (STEMI), hemodynamically unstable, known other causes of chest pain, traumatic chest pain, required for hospitalization because of other illnesses, refused for consent, under palliative care or terminally ill patients, pregnant, and not available for follow-up after discharge were excluded. (Table 2)
Inclusion and exclusion criteria.
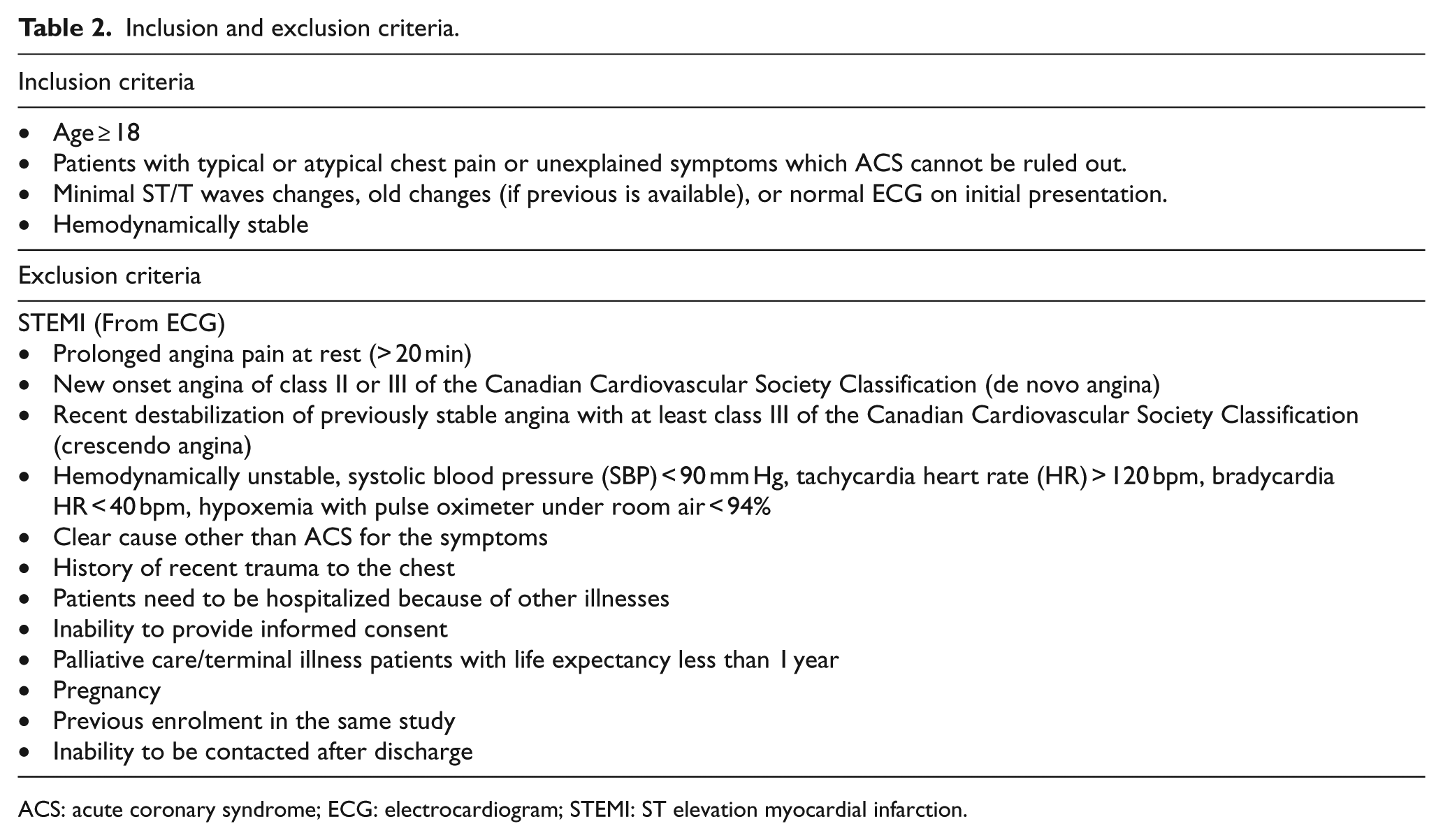
ACS: acute coronary syndrome; ECG: electrocardiogram; STEMI: ST elevation myocardial infarction.
All of the recruited patients were observed in the observation ward for serial ECG and hs-cTnT tests. The hs-cTnT test was performed using Elecsys® Troponin T high-sensitivity assay. It is a quantitative assay. The diagnostic cut off of this assay for myocardial infarction is more than 14 ng/L. 14 Patients were classified into Groups A, B, and C based on the duration of the onset of the symptoms. Group A was patients presented within 2 hours of symptoms, Group B was patients presented between 2 and 4 hours of symptoms, and Group C was patients presented more than 4 hours of symptoms. Each group had their own timing for hs-cTnT test. T0 is defined as hs-cTnT taken at 2 to 4 hours after the onset of the patients’ symptoms. T2 is defined as hs-cTnT taken 2 hours after T0, and T4 is defined as hs-cTnT taken at 4 hours or more after the onset of patients’ symptoms. For Group A, patients had to wait until 2 hours of symptoms for the first hs-cTnT test (T0), whereas for Groups B and C, the first hs-cTnT test (T0/T4) can be taken on admission. For Groups A and B, if T0 was negative, hs-cTnT would be repeated at 2 hours after T0, and it would be labeled as T2 (Figure 1).
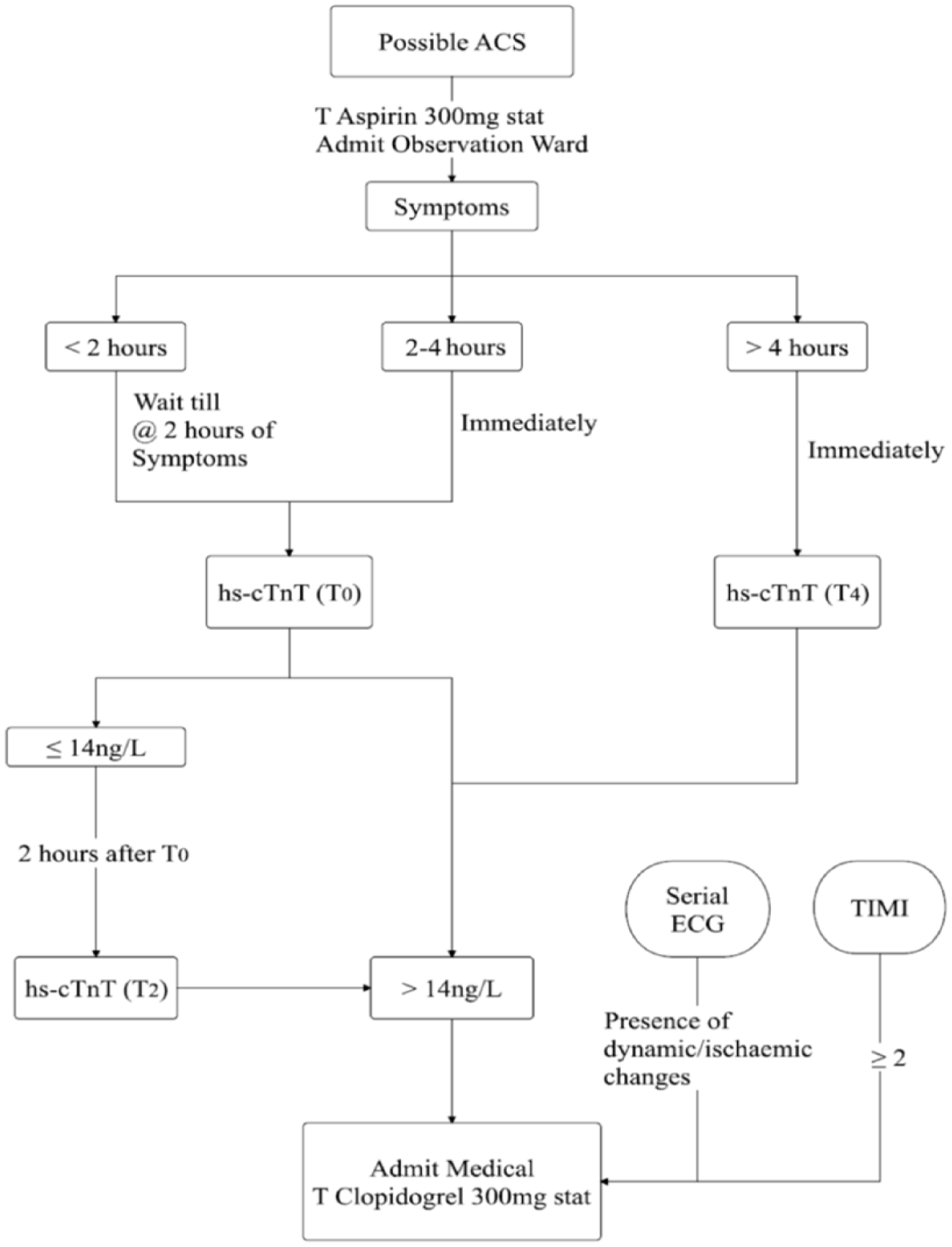
Study flow chart part I.
TIMI score was calculated for all patients. Patients with TIMI score ≥ 2, ischemic or dynamic changes in serial ECGs, or either T0, T2 or T4 > 14 ng/L were diagnosed as having ACS. They were treated with dual antiplatelet and anticoagulant, and admitted for further intervention in the ward. Whereas patients with TIMI score < 2, no ischemic or dynamic changes in serial ECGs, T0 and T2 or T4 ≤ 14 ng/L, resolving symptoms, and hemodynamically stable were discharged with an appointment for exercise treadmill test (ETT) within 1 week. Patients unable to perform ETT were referred to physician clinic for further cardiac assessment. If there were no contraindications, all discharged patients were continued with oral salicylic acid (Aspirin) 150 mg daily.
An appointment for ETT within 1 week was arranged for all the discharged patients to assess for the possibility of stress induced myocardial ischemia, unless patients unable to perform ETT. The test was performed by well-trained medical assistants or staff nurses and supervised by medical officers. Results would be reviewed by medical officers under the supervision of emergency physicians. Consultation with cardiologist was available at all time if needed. Patients with negative ETT were low-risk patients and they were allowed for discharge. Whereas patients with positive or inconclusive ETT were high-risk patients and they were referred to physician clinic for further cardiac assessment. They were continued with oral Clopidogrel 75 mg daily, and salicylic acid (Aspirin) 150 mg daily (Figure 2).
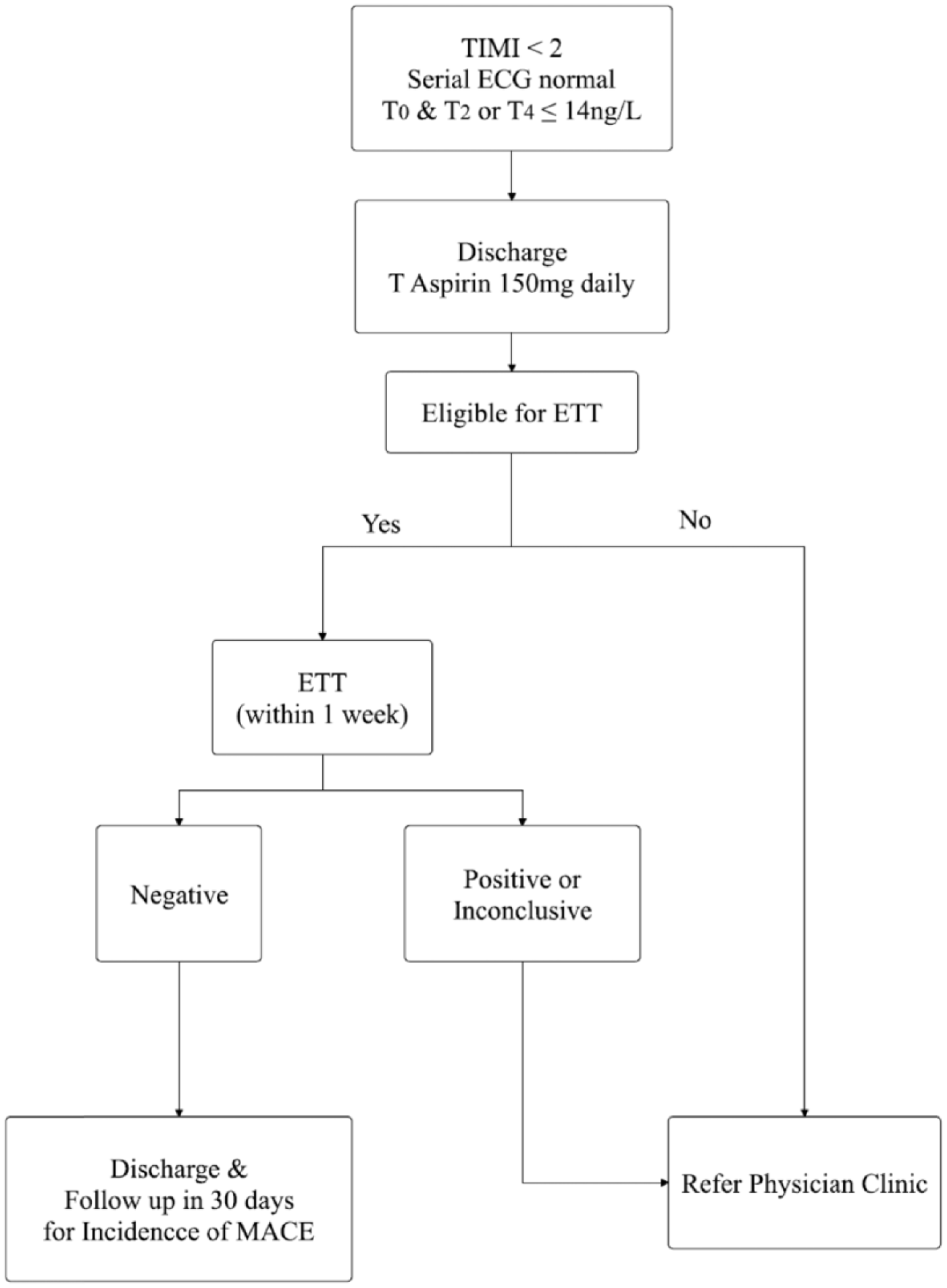
Study flow chart part II.
All studied patients were reviewed in 30 days for any incidence of MACEs via either phone call, inpatient case note reviewed, administration record for revisit or readmission to ETDHKL, and laboratory records.
Statistical Package for Social Science (SPSS), 22nd edition and Microsoft Excel were used as the statistics software programs to process and analyze all the raw data. Baseline characteristics of patients were presented by using descriptive statistics such as charts, distribution, frequencies, or percentage. Continuous data were presented as means ± standard deviations (SD), or as medians and interquartile ranges. Categorical data were presented as frequencies and percentages. The sensitivity, specificity, positive, and negative predictive values of the modified accelerated diagnostic protocol for MACEs in 30 days were calculated by using chi-square analyses. For all analyses, p values less than 0.05 were considered statistically significant.
Results
During the studied period, 328 consented patients were recruited initially. About 154 patients were excluded from the study because 94 did not follow OBSSES Protocol, 45 defaulted ETT, and 15 defaulted physician clinic follow-up (Figure 3).
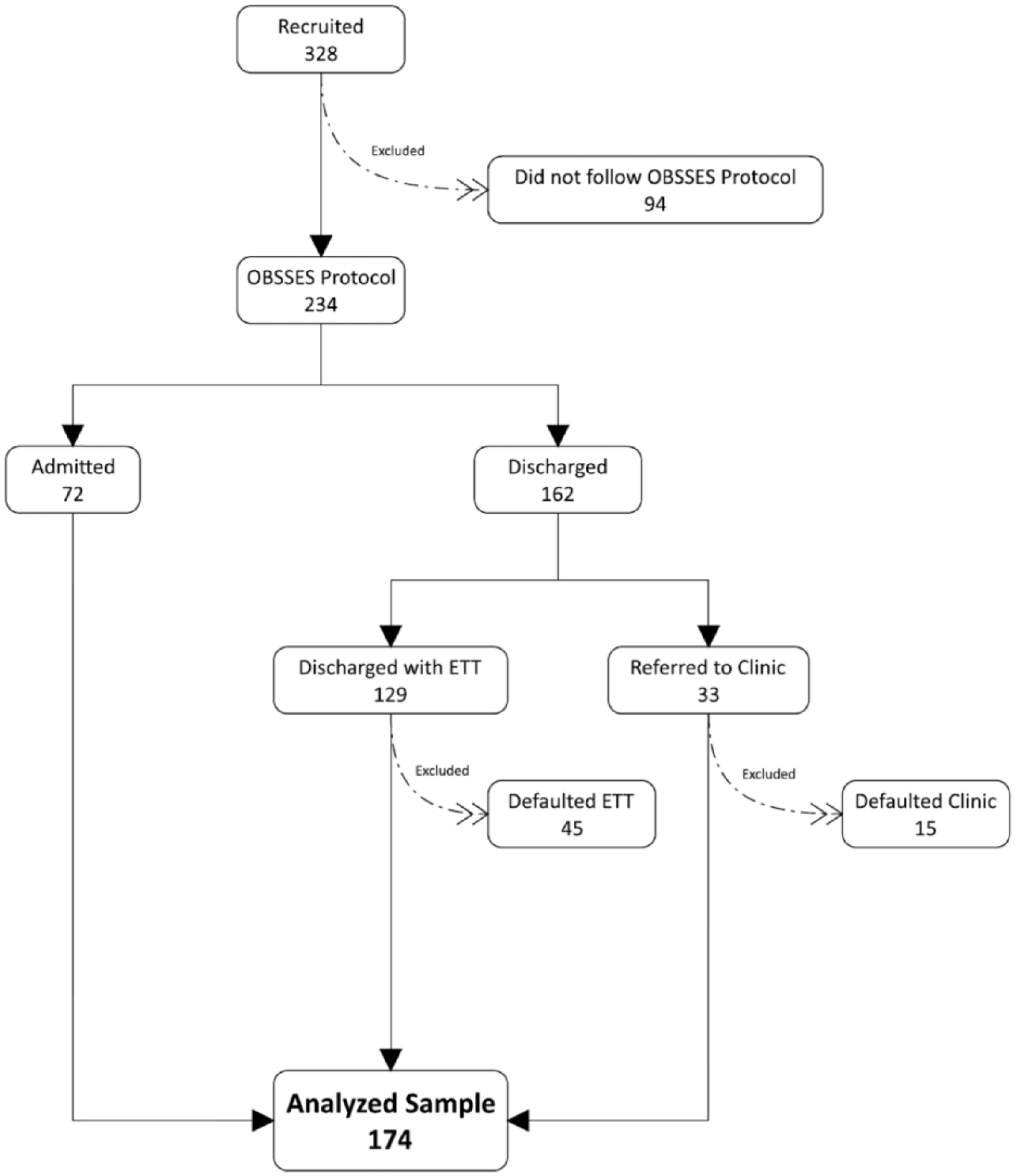
Summary of the overall process of patients’ recruitment.
A total of 174 patients were analyzed, of which 72 patients (41.4%) were diagnosed as ACS and admitted to the medical ward for further intervention and 102 patients (58.6%) were allowed for discharge. Among the discharged patients, 84 (82.4%) were discharged with ETT appointment within 1 week, and 18 (17.6%) were referred to physician clinic appointment for further cardiac assessment because they were not eligible for ETT.
Baseline characteristic data showed that both high-risk and low-risk patients were more male than female. Low-risk patients were younger. The mean age of the low-risk patients was 42.9 (SD 14.9) years, and for the high-risk patients was 58.3 (SD = 12.7) years. Co-morbidities such as hypertension, DM, dyslipidaemia, CVA, CAD, and history of PCI or CABG were more common in high-risk patients. Totally, 20 (12%) patients presented within 2 hours of symptoms, 22 (13%) patients between 2 to 4 hours of symptoms, and 120 (76%) patients presented with more than 4 hours of symptoms. (Table 3) There was no significant difference between the baseline characteristics of the analyzed population and the excluded population (Table 4).
Baseline characteristics of the high-risk and low-risk patients.
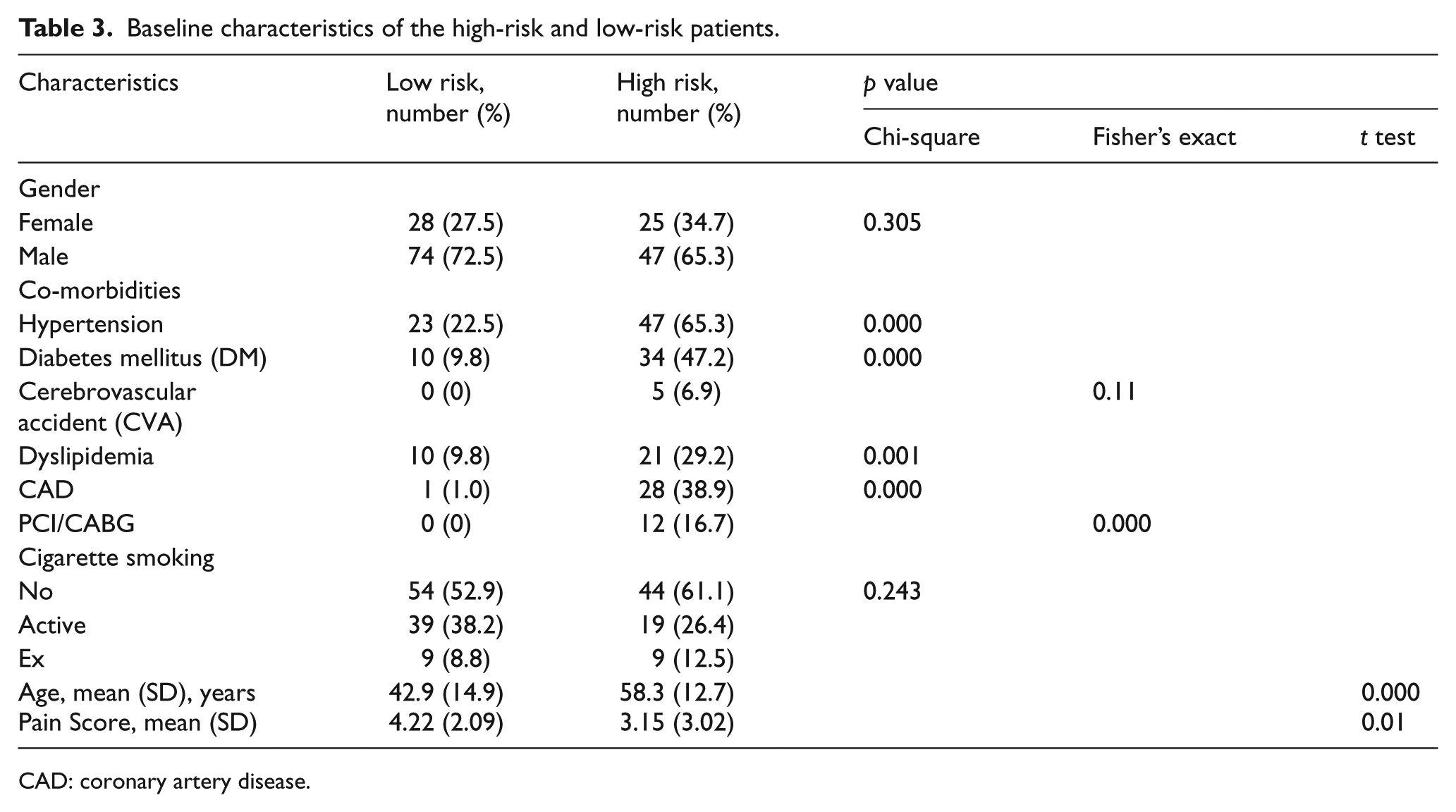
CAD: coronary artery disease.
Baseline Characteristics of the analyzed and excluded population.
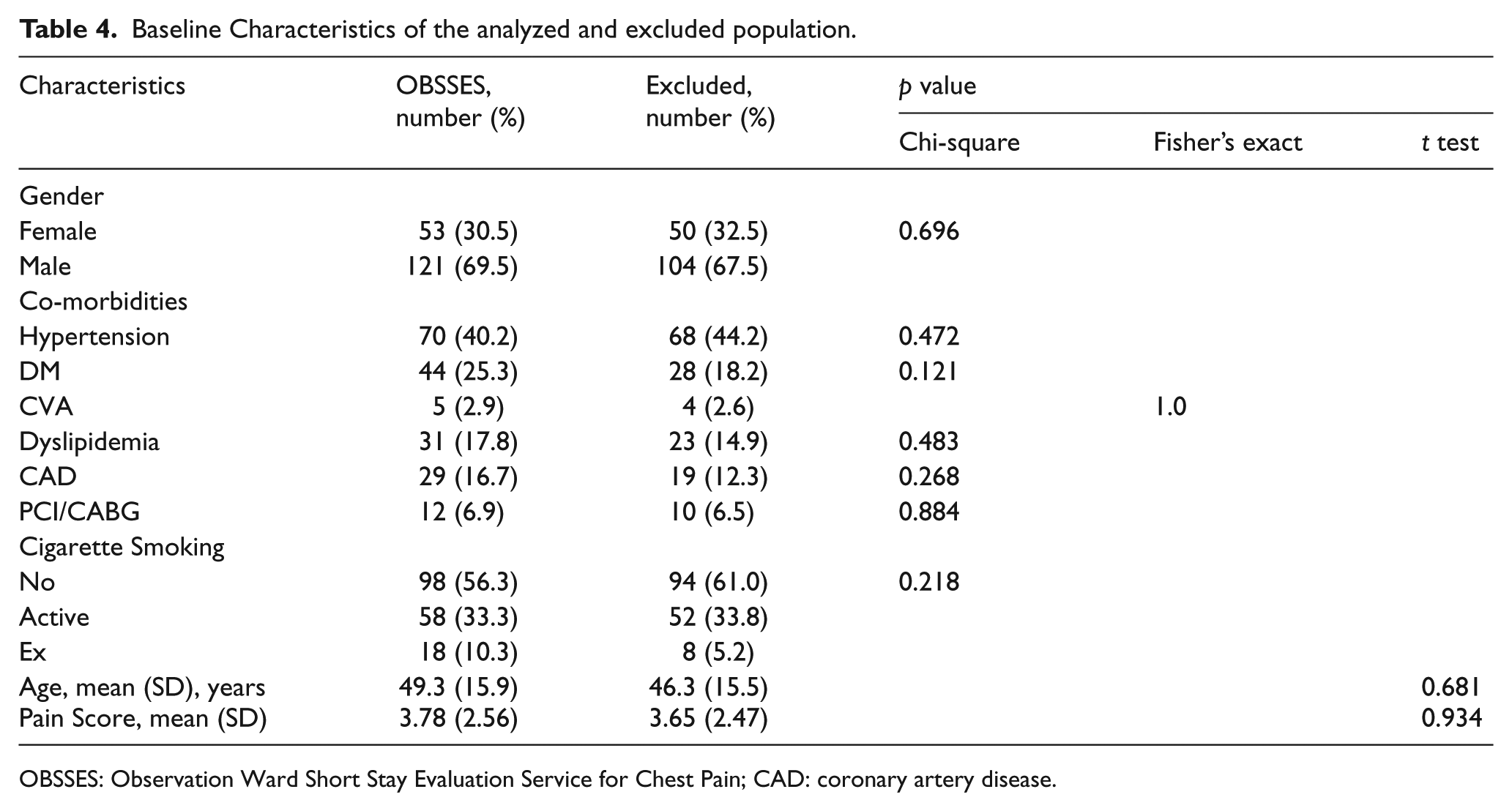
OBSSES: Observation Ward Short Stay Evaluation Service for Chest Pain; CAD: coronary artery disease.
Among the high-risk patients who were admitted to medical ward, 38 (52.8%) patients were treated as ACS by medical team after further evaluation. Among this cohort, 24 (63.2%) patients had NSTEMI, 13 (34.2%) patients had UA, and 1 (2.6%) patient had cardiac death. The specificity and PPV of OBSSES Protocol to diagnose ACS were both 35.9% (Figure 4).
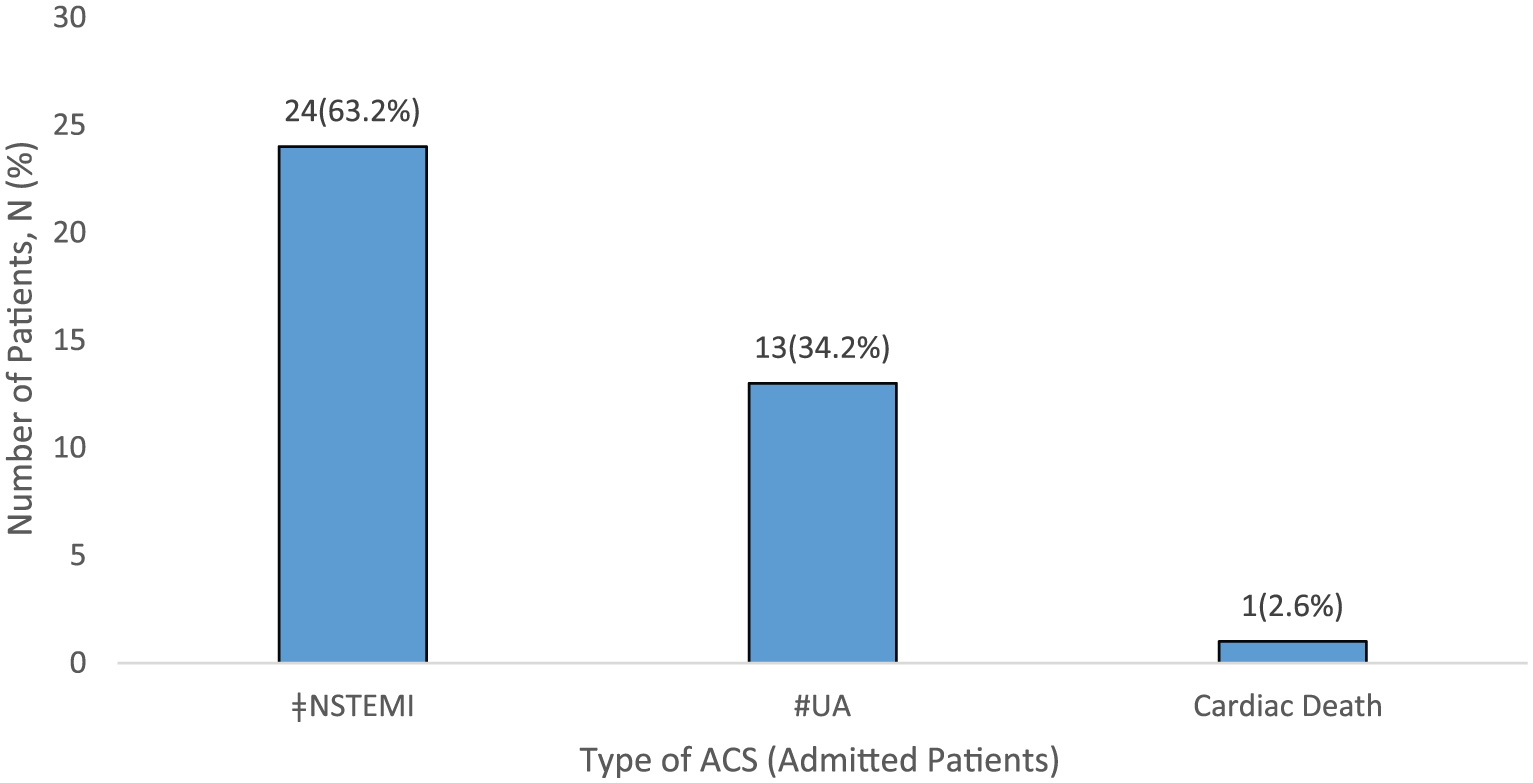
Type of ACS among admitted patients.
About 102 patients were allowed for discharge. Totally, 84 (82.4%) patients discharged with an appointment for exercise treadmill test within 1 week, and 18 (17.6%) patients discharged with a referral to physician outpatient clinic for further cardiac assessment. Patients who underwent ETT, 46 (54.8%) patients had negative ETT, 17 (20.2%) patients had positive ETT, and 21 (20.6%) patients had inconclusive ETT (Figure 5). Among the 38 patients with either positive or inconclusive ETT, six patients underwent invasive coronary angiogram, and two patients found to have significant coronary stenosis which required stenting. The incidence of MACEs among low-risk patients with negative ETT in 30 days were zero. The sensitivity and NPV of OBSSES Protocol to identify and safely discharge low-risk patients were both 100%.
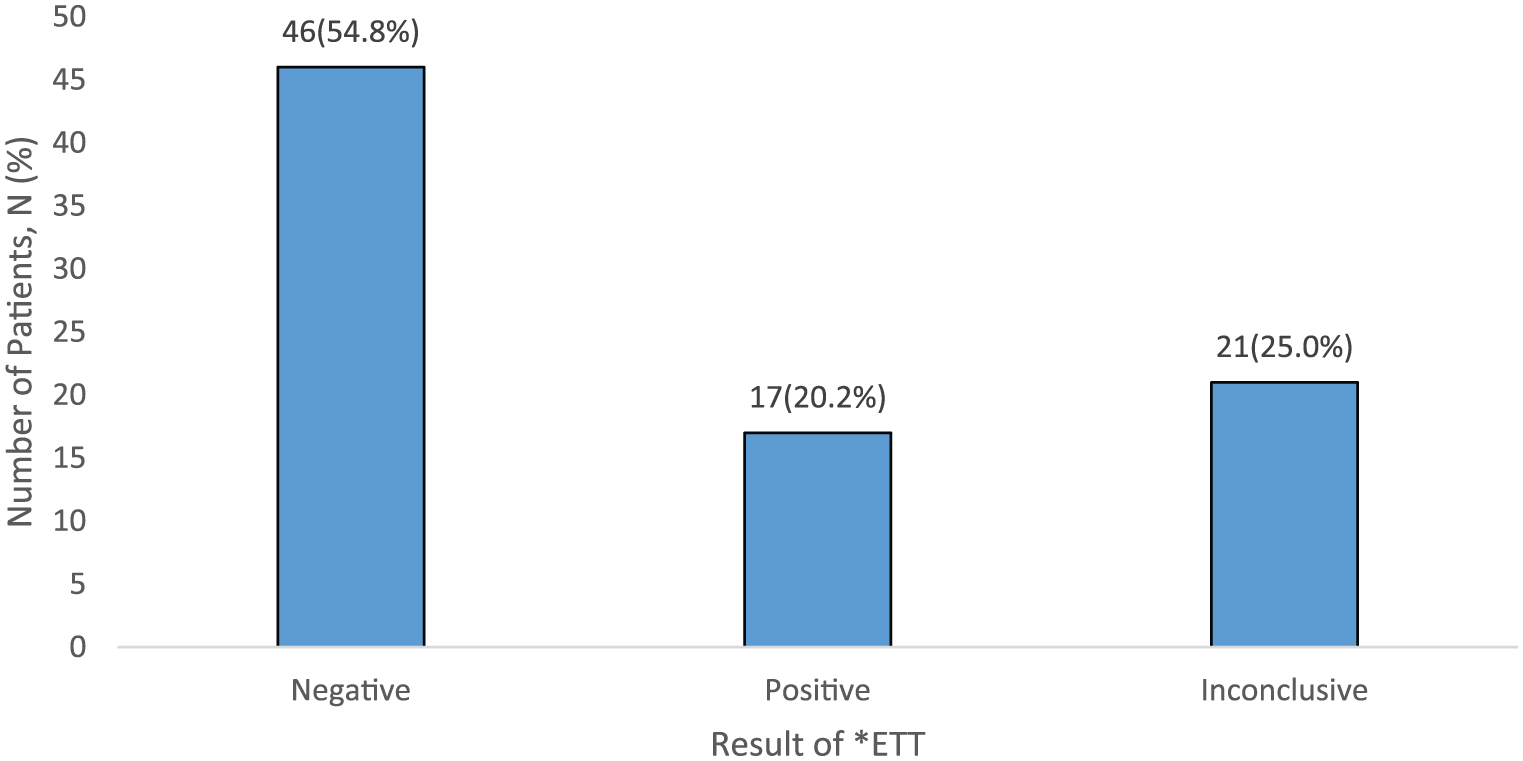
Results of ETT.
Subgroup analysis of the excluded population was conducted to evaluate incidence of MACE. Among patients who met the criteria for admission but discharged, three patients developed UA and one patient had NSTEMI. Two patients, who met the criteria for discharge with ETT but admitted, were diagnosed to have UA in the ward. Among patients who were supposed to be discharged with ETT but were discharged without further follow-up, one patient revisited ED and admitted for UA. Among patients who defaulted ETT, two patients revisited ED and admitted for UA.
Discussion
Chest pain is a common presentation which consists of 10% of emergency departments visits and 25% of annual hospital admission yet only about 15% to 25% of the admitted patients have the diagnosis of ACS. 6 This number represents a very small proportion of chest pain patients in emergency departments. Most of the patients were unlikely to have ACS; however, inadvertent discharge of patients with true or ongoing ACS will lead to deleterious outcomes. Pope et al. study showed that missed acute myocardial infarction (AMI) and UA had almost double the mortality rate for patients who were not admitted, as compared to patients who were. 15
According to the ETDHKL annual censor, in 2014, a total of 466 patients with the initial impression of possible ACS were admitted to observation ward in ETDHKL; after undergoing evaluation, 339 (73%) were allowed for discharged without further follow-up or cardiac assessment. There was a possibility of inadvertent discharge of patients with underlying significant CAD.
A study regarding the efficacy of the previous ADP in ETDHKL, which consisted of a TIMI score of 0, normal of no dynamic changes in serial ECGs, and hs-cTnI of ≤ 0.02 ng/mL showed a miss rate of 2% and only achieved a sensitivity of 90.48% and a NPV of 97.98%. 8 Compared with this study, the previous studied cohort was younger and with lower cardiovascular risk factors, only included patients with TIMI of zero; however, there was still 2% risk of MACEs in 30 days. This study showed that OBSSES Protocol with TIMI score of 0 or 1, hs-cTnT ≤ 14 ng/L, normal serial ECG, and negative early ETT, was the better protocol to evaluate chest pain patients in emergency departments.
Totally, 102 (58.6%) patients were allowed for discharged, this was better than the three studies done by Than et al. which are ASPECT, ADAPT, and EDACS ADP.6,7,9 In ASPECT, ADAPT, and EDACS ADP studies, the investigators only able to identify 9.8%, 20%, and 51.3% of low-risk patients, respectively. OBSSES Protocol managed to discharge more patients form the emergency department and reduce the rate of ward overcrowding and access block.
None of the discharged patients developed MACEs within 30 days of the initial presentation; this gave rise to zero MACE within the 30 days of discharge. The incidence of MACEs in ASPECT and ADAPT studies were 0.9% and 0.25%, respectively.6,7
OBSSES Protocol managed to achieve better sensitivity and NPV than ASPECT and ADAPT trials.6,7 Both of the sensitivity and NPV of OBSSES Protocol were 100%, whereas the sensitivity and NPV for the previous study were 90.48% and 97.98%, respectively, for ASPECT were 99.3% and 99.1% respectively, and for ADAPT were 99.7% for both of the sensitivity and NPV. Even though this study included patients with TIMI score of 1 compared to the previous study, ASPECT and ADAPT trials, which only recruited patients with TIMI score of 0, this study still managed to achieve higher sensitivity and negative NPV. This could be due to the additional of ETT as one of the components of OBSSES Protocol.
Studies done by Douglas et al. show that immediate ETT in emergency department is a safe and reliable method for risk stratification of patients with low risk of MACEs. 16 In J Douglas’ study patients fulfilled the criteria underwent immediate ETT was safe even for patients with known CAD and ongoing chest pain. In their study, patients were identified as low risk based on initial 12 lead ECG and physical findings. Patients were sent for immediate ETT even before the cardiac biomarkers were available. The mean time from admission to the emergency department to ETT was 1 hour. In their studies, there were no significant adverse outcomes during the exercise stress test. There were no patients from this study developed significant complications like AMI, arrhythmia, cardiac arrest, or syncopal attack during ETT.
In this study, ETT was unable to be done on the same day due to logistic issue. Although appointment for ETT was arranged, and the purpose of ETT was explained clearly, there were still 45 patients who defaulted ETT. It would be better if ETT could be performed before patients were allowed for discharge to improve the default rate, and patients with positive or inconclusive results could be referred earlier to medical team; however, resource limitation was a major constrain to carry it out.
Ninety-four patients failed to follow OBSSES Protocol and were excluded from the study. OBSSES Protocol was just a guide to chest pain management in ETDHKL, but the final disposition of patients was still based on patient clinical findings and emergency physician decisions. Among the 94 patients, 38 met the admission criteria but 13 were discharged without further follow-up, 12 were discharged to physician clinic, and 9 were discharged with an appointment for ETT. The reasons given by the emergency physicians were patients’ ECG changes were old changes, elevated serum cardiac troponin T was due to chronic renal failure, and patients’ symptoms were caused by other more benign conditions. On the other hand, 56 patients who had met the criteria for discharge with ETT, 25 were admitted and 31 were discharged without any appointment for ETT or further follow-up. The reasons were patients did not have good family support and thus better to be admitted, patients likely to default outpatient appointment, the gut feeling of the emergency physicians that patients were not safe enough to be discharged, or the emergency physicians did not think ACS or coronary artery disease (CAD) was the underlying cause of patients’ symptoms.
Subgroup analysis of the excluded population showed that among the five patients who had met the criteria for discharged with ETT appointment, two patients were admitted instead of discharged, one patient was discharged without appointment for ETT, and two patients were discharged with ETT appointment but patients defaulted. The two patients who had admitted were treated as UA in the ward, and the other three patients readmitted to ED for UA. Although this subgroup analysis found out that there were some cardiac events among the excluded patients, these events were not MACEs. Furthermore, all these five patients were supposed to be discharged with ETT appointment thus they might be able to be identified during ETT.
The specificity of OBSSES Protocol was only 35.9% in rule in ACS. The specificity was low; however, it was better than ASPECT and ADAPT trials which only achieved a specificity of 11.0% and 23.4%, respectively.6,7In this study, hs-cTnT was used, compared with the old generation hs-cTnT able to detect myocardial injury earlier.17–19 However, its specificity is relatively low, elevated value in hs-cTnT is not specific to ACS, certain medical conditions can lead to increased baseline hs-cTnT, such as chronic renal failure, elderly, and known underlying CAD. In order to improve the specifity of hs-cTnT, delta change of serial hs-cTnT can be calculated.20–22
OBSSES Protocol was only able to achieve high sensitivity and NPV if all the components are included. The sensitivity and NPV of isolated ECG, hs-cTnT, and TIMI score in patients with possible ACS were not as high as the complete OBSSES Protocol (Table 5). OBSSES Protocol without the component of ETT was only able to achieve a sensitivity of 87.0% and NPV of 94.1%. These were lower than the sensitivity and NPV of the ASPECT and ADAPT trials.6,7 This can be due to the different cut-off point of TIMI score.
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of OBSSES Protocol and each isolated component of OBSSES Protocol.
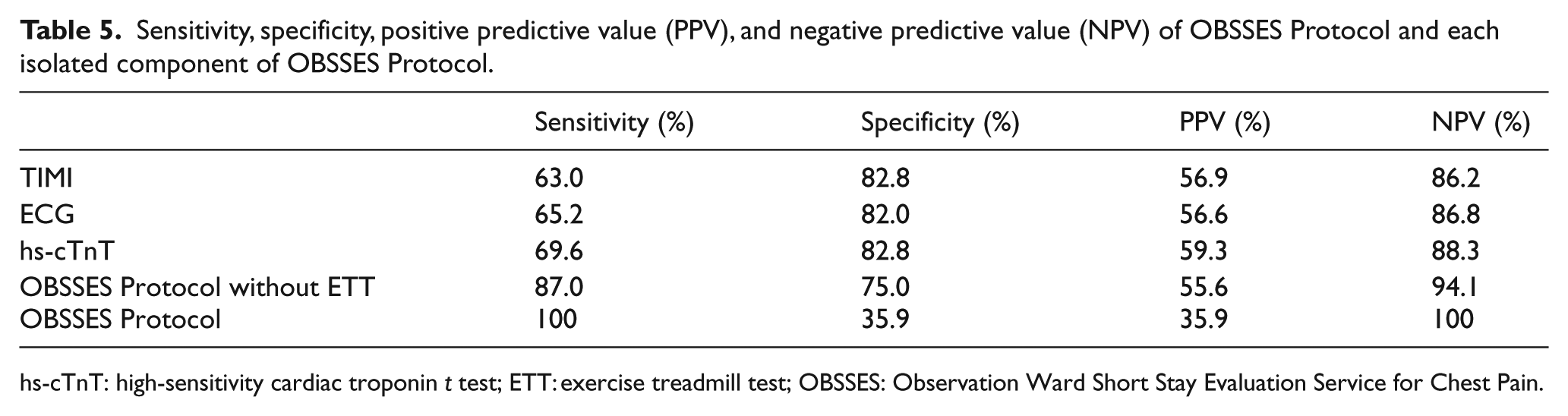
hs-cTnT: high-sensitivity cardiac troponin t test; ETT: exercise treadmill test; OBSSES: Observation Ward Short Stay Evaluation Service for Chest Pain.
Future studies
Our study showed that ETT played an important role in excluding ACS with short term of MACEs. In further studies, we suggest ETT or other confirmatory test like stress echocardiogram which can be easily performed in emergency departments should be performed before patients are allowed for discharged to avoid defaulters. Future studies also can consider point-of-care hs-cTnT to shorten the observation or waiting time in the emergency departments, and involved the dynamic or delta change of hs-cTnT to improve the specificity of hs-cTnT especially in patients with elevated baseline cardiac troponin level.
Limitations
This is a single center study and the sampling method of this study was a convenient method which dependent on the availability of the investigator thus not all the patients who fulfilled the criteria within the studied period were recruited into the study.
Gold standard invasive coronary angiography (ICA) to investigate CAD was not performed in all of the studied patients, thus the severity of CAD were unable to be assessed. It was unethical to perform ICA in all of the patients because the test is invasive, is not without complications, and too costly. In view of that, there is still a possibility that some of the studied patients with underlying CAD were not detected and discharged to the community. These patients although did not suffer from any MACEs within the 30 day, the long term complication is still uncertain. However, this study did shows that OBSSES Protocol can be apply safely in emergency departments to evaluate and discharge patients with low risk of short-term MACEs within 30 days.
Conclusion
This study shows that OBSSES Protocol which included TIMI score of 0 or 1, negative serial ECGs, hs-cTnT ≤ 14 ng/L, and negative ETT in evaluating patients presenting with symptoms suspicious of ACS in emergency departments, is an effective and safe protocol to identify and discharge patients with low incidence of MACEs in 30 day.
Footnotes
Appendix
To calculate the sample size (N) based on the need for adequate sensitivity, the following formula was used:
Acknowledgements
Authors would like to thank Dato’ Sri Dr Abu Hassan Ashaari, the Head of Department, Emergency and Trauma Department, Hospital Kuala Lumpur, Prof. Rashidi Bin Ahmad, the consultant and senior lecturer in emergency medicine, University Malaya Medical Center, Mr. Nagalingam A/L Poomaly, the medical assistance U32, Emergency and Trauma Department Hospital Kuala Lumpur, and all the staff of Emergency and Trauma Department Hospital Kuala Lumpur, who contributed to the study. Dr. Mahathar Bin Abdul Wahab involved in the concept and methodology of the study. He supervised all the time for the study which includes the proposal, data collection, data analysis, and manuscript preparation. Dr. Kok Siew Yean involved in the concept, literature reviewed, methodology, proposal, data collection, data analysis and interpretation, and manuscript preparation. Associate Prof. Mohd Idzwan Bin Zakaria supervised for the study proposal, data analysis, data interpretation, and manuscript preparation.
Declaration of conflicting interests
The aims of the study was to study the efficacy and the safety of OBSSES Protocol, which is a modified accelerated diagnostic protocol in the evaluation of patients presented with chest pain or angina equivalents in Emergency and Trauma Department, Hospital Kuala Lumpur. The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article..
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Study data and results are available in SPSS and Microsoft Excel files.
Ethical approval and Informed consent
This study was approved by the Medical Review & Ethics Committee (MREC), Ministry of Health of Malaysia in 2016 (Approval Code: NMRR-16-24-28858). All the studied or recruited patients were consented.