
Abstract
After cardiac surgery, a certain degree of myocardial injury is common. The arbitrarily proposed biomarker cut-off point in the Third Universal Definition for diagnosing coronary artery bypass grafting (CABG)–related perioperative myocardial infarction (PMI) is controversial and unvalidated for non-CABG surgery. Minimally invasive cardiac surgery is often thought to be associated with less myocardial damage compared to conventional surgical approaches. We conducted a real-life prospective study with serial sampling of high-sensitivity cardiac troponin T (hs-cTnT) in patients undergoing conventional and minimally invasive cardiac surgery. Four different types of cardiac surgery were performed in 400 patients (February 2014–January 2015): CABG, aortic valve replacement, minimally invasive mitral/tricuspid valve surgery through the HeartPort (HP) technique and combined CABG/valve surgery. Each group was further subdivided for comparison between the different surgical techniques. Blood samples were collected consecutively at intensive care unit (ICU) admission and 3, 6, 9, 12, 18, 24 and 48 h thereafter. The hs-cTnT values by peak timepoint differed significantly depending on the surgical approach. The overall peak timepoint for hs-cTnT occurred 6 h after ICU admission. The combined surgery and multiple-valve HP groups had the highest values (medians of 1067.5 (744.9–1455) ng/L and 1166 (743.7–2470) ng/L, respectively). The peak hs-cTnT values for patients developing PMI showed high variability. Differentiation between cardiac surgery–related necrosis and PMI remains challenging. This study emphasizes the importance of a clinically reliable biomarker cut-off value in addition to electrocardiography and echocardiography to optimize PMI diagnosis.
Introduction
Perioperative myocardial infarction (PMI) remains an important complication after cardiac surgery, especially after coronary artery bypass grafting (CABG), and is associated with increased morbidity and mortality.1–4 The incidence reported by the Society of Thoracic Surgeons varies widely depending on the different diagnostic criteria used, with an average of 3.9%. 5 In 2012, the Joint American College of Cardiology, American Heart Association, European Society of Cardiology and World Heart Federation Task Force proposed the Third Universal Definition for CABG-related PMI as elevation of cardiac biomarker values >10× the 99th percentile of the upper reference limit (URL) in patients with normal baseline cardiac troponin (cTn) values (≤ the 99th percentile of the URL) in addition to either new pathological Q waves or new left bundle branch block, angiographically documented new graft or native coronary artery occlusions, or imaging evidence of new viable myocardium loss or new regional wall motion abnormalities. 6
High-sensitivity cardiac troponins (hs-cTn) are the most sensitive and cardiac-specific biomarkers currently available. Recommendations for their use as the gold standard for detection of myocardial injury in acute cardiac care are well described in the literature.6–9 After cardiac surgery, a certain degree of myocardial injury is common, even in the absence of postoperative adverse events.10–11 Moreover, although hs-cTn release may typically reflect de novo myocardial ischaemia, it may be influenced by surgical trauma, the need for cardiopulmonary bypass (CPB), and the myocardial protection technique.11–15 In addition, hs-cTn levels may already be elevated in patients with end-stage renal disease, acute pericarditis, acute heart failure, sepsis, rhabdomyolysis or other clinical conditions. 16
In the context of cardiac surgery, most studies on cardiac biomarker release have primarily examined patients undergoing on-pump CABG surgery,17–20 in contrast to the seldom-studied release pattern of hs-cTn after non-CABG surgical procedures such as isolated valve surgery, combined CABG/valve surgery and minimally invasive cardiac surgery. In our institution, minimally invasive cardiac surgery comprises off-pump single-vessel robotic-assisted CABG (in which dissection of the left internal mammary artery is performed using a robotic system (Da Vinci Surgical System; Intuitive Surgical, Mountain View, CA, USA), and thoracic access to the heart is achieved by left mini-thoracotomy), aortic valve replacement (AVR) through a J-shaped partial upper sternotomy (upper partial sternotomy with a unilateral J-shaped extension to the right through the fourth intercostal space) and mitral and/or tricuspid valve surgery using the HeartPort (HP) technique (a video-assisted right thoracotomy approach to the heart with single-lung ventilation, femoro-femoral CPB and antegrade cardioplegia through endo-aortic balloon clamp technology).
Minimally invasive cardiac surgery is often thought to be associated with a milder degree of myocardial damage compared to conventional surgical approaches through median sternotomy using CPB. We therefore conducted a real-life prospective study with serial sampling of high-sensitivity cardiac troponin T (hs-cTnT), the preferred cardiac biomarker in our institution, to determine its postoperative release pattern after conventional as well as minimally invasive cardiac surgery. Second, we compared hs-cTnT levels with the cut-off values for PMI described in the Third Universal Definition of PMI. 6 Third, we sought to identify outcome-associated variables related to increased hs-cTnT release.
Materials and methods
Study design and patient population
This single-centre prospective study was approved by the institutional ethics committee (2013/038) and preregistered on clinicaltrials.gov (NCT 01913873). Between February 2014 and January 2015, 400 patients undergoing different types of cardiac surgery were eligible for this study. Patients who were on dialysis, with planned insertion of assist devices, with planned deep hypothermic circulatory arrest or admitted for emergency surgery were excluded. After providing written informed consent, 389 patients were finally included in the study. The patients were divided into four groups depending on the type of cardiac surgery: (1) the CABG group; (2) the AVR group; (3) the HP group; and (4) the combined group (combined CABG and valve surgery or multiple valve surgery through median sternotomy). Each group, with the exception of the combined group, was then subdivided for comparison between different surgical techniques: (1) for the CABG group, on-pump CABG versus off-pump CABG (OPCAB) versus off-pump robotic-assisted CABG; (2) for the AVR group, median sternotomy versus J-shaped partial upper sternotomy; and (3) for the HP group, one-valve versus two-valve surgery. A total of eight groups were thus considered for analysis (Figure 1).
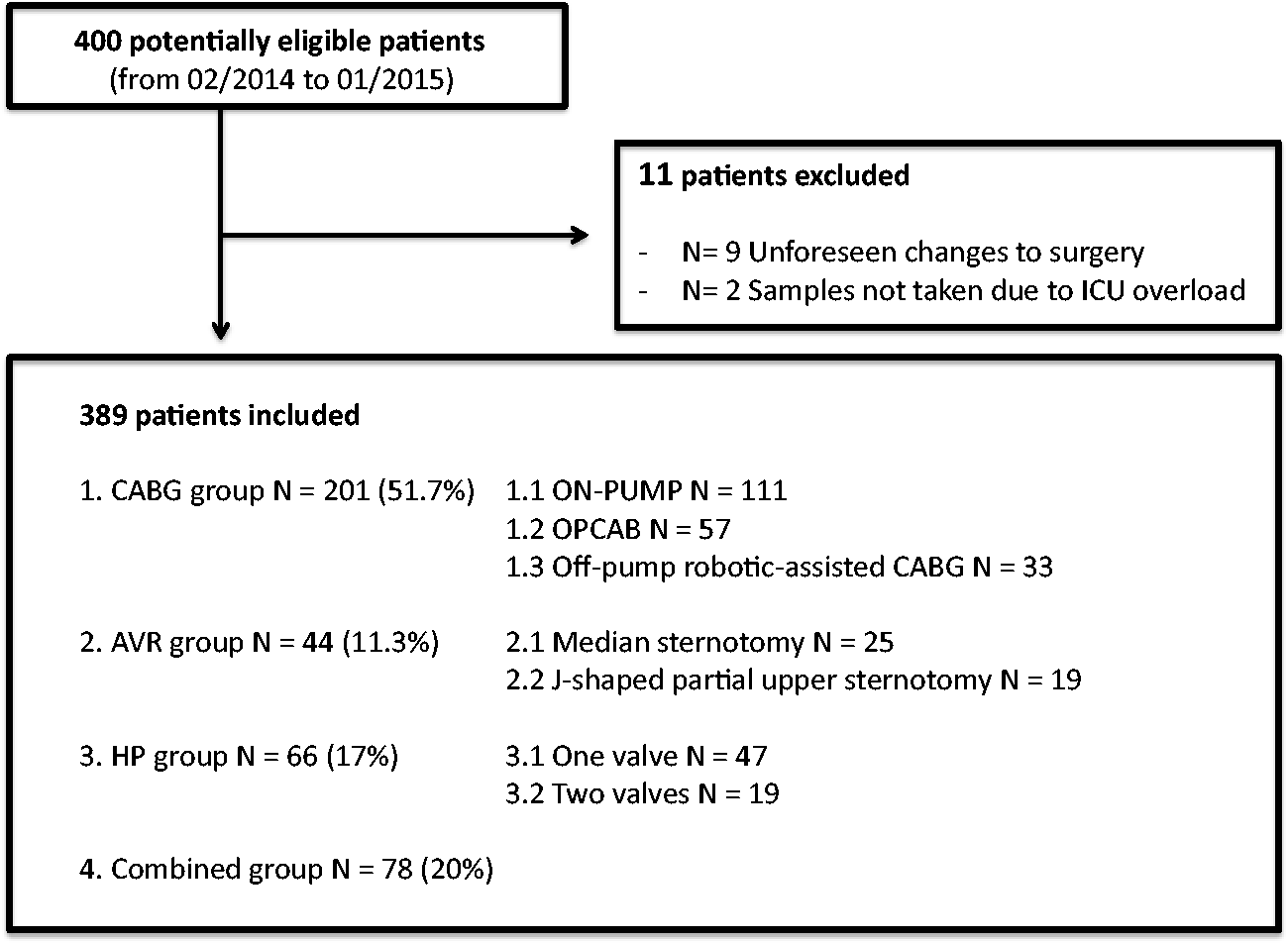
Flowchart illustrating potentially eligible, excluded and included patients by the type of surgery/surgical technique.
Perioperative management and data collection
The surgical technique and the anaesthesia management technique were selected at the discretion of the attending physicians and in accordance with good clinical practice. The study protocol did not interfere with the normal daily clinical management of the included patients. All pre-, intra- and postoperative data were prospectively collected by the same anaesthesiologist (NDM). The preoperative data collected included the patients’ demographic characteristics, medical history, use of habitual medication, presence of comorbid conditions, left ventricular ejection fraction (LVEF) (good LVEF: >50%; moderate LVEF: 30–50%; and poor LVEF: <30%), and renal function (normal: glomerular filtration rate >90; mild renal insufficiency: glomerular filtration rate of 60–89; moderate renal insufficiency: glomerular filtration rate of 30–59; and severe renal insufficiency: glomerular filtration rate <30 mL/min/1.73 m2). The following intraoperative data were collected: CPB and aortic cross-clamp times, myocardial protection strategies and the need for defibrillation (for ventricular fibrillation/tachycardia or atrial fibrillation) before or after weaning from CPB.
Twelve-lead electrocardiographs (ECGs) obtained routinely on the day prior to surgery, immediately upon arrival in the intensive care unit (ICU), daily at 6:00 a.m. and, for the purpose of the study, 24 and 48 h after ICU arrival were retrospectively reviewed by one cardiologist blinded to all other data for evidence of new postoperative ischaemia, as described in the Third Universal Definition of PMI. Transthoracic or transoesophageal echocardiography was performed when clinically indicated to trace new regional wall motion abnormalities and recorded accordingly.
To analyse clinical outcomes, all major adverse events (MAEs) occurring during the ICU stay were divided into cardiac and non-cardiac events. A cardiac MAE was defined as one of the following: new atrial fibrillation, sustained ventricular arrhythmias, systolic heart failure (confirmed by echocardiographic evidence), excessive bleeding (>2.0 L/24 h and/or the need for re-exploration), new signs of ischaemia (Q and non-Q wave) on ECG and urgent re-exploration. Non-cardiac MAEs included respiratory failure (infection, prolonged intubation for >24 h, need for re-intubation), renal failure (a glomerular filtration rate reduction > 50% of the baseline value), the need for dialysis, stroke, and sepsis (defined as life-threatening organ dysfunction caused by an infection). Other postoperative variables recorded included the use of inotropes and vasopressors in the operating room or ICU, ICU/hospital stay durations and ICU/in-hospital mortality. The follow-up occurred retrospectively after 30 days, 12 months and three years by consulting electronically available medical charts.
High-sensitivity cardiac troponin T
In our institution, hs-cTnT is routinely measured at ICU admission and at 6:00 a.m. every day until discharge from the ICU (or otherwise as decided by the attending ICU physician). In the interest of the study, serial sampling occurred on a predefined time schedule. The hs-cTnT values measured in blood samples collected before induction of anaesthesia were considered the baseline values (T ind). Blood samples were then consecutively collected at ICU admission (T0) and 3, 6, 9, 12, 18, 24 and 48 h after ICU admission for a total of nine samples per patient. All analyses were performed in the department of Clinical Chemistry of the OLV Hospital on a cobas® 6000 <601> analyser (Roche Diagnostics, Switzerland) with an Elecsys® Troponin T hs assay by dedicated laboratory technicians blinded to all patient data. The 99th percentile for hs-cTnT was 14 ng/L. The limit of quantification for hs-cTnT, corresponding to the lowest concentration with a coefficient of variation less than or equal to 10%, was 13 ng/L.
Statistical analysis
We divided the hs-cTnT peak values by the URL (14 ng/L) for comparison with other assays and for compatibility with the Third Universal Definition of PMI. For descriptive purposes, we arbitrarily divided the peak values into quartiles; Q1: 0 to <10× the URL (<140 ng/L); Q2: 10 to <30× the URL (140–420 ng/L); Q3: 30 to <50× the URL (421–700 ng/L), and Q4: >50× the URL (>700 ng/L). The categories of hs-cTnT were arbitrarily selected according to a retrospective analysis of patients undergoing cardiac surgery in our institution over the last decade.
Continuous variables are presented as the means and standard deviations or as the medians and interquartile ranges as appropriate. Hs-cTnT differences between groups were assessed using analysis of variance (ANOVA) or a Kruskal–Wallis test as appropriate. The groups were as follows: (1) the CABG group; (2) the AVR group; (3) the HP group; and (4) the combined group. Categorical variables are presented as the observed frequencies and percentages. Differences between groups were assessed using Fisher’s exact test.
Longitudinal hs-cTnT data were analysed using a linear mixed model that included a random intercept to account for within-patient correlations. The model included the baseline value (at induction), type of surgery and timing of measurement as fixed effects; the latter two variables were included as class factors. In addition, the interaction between surgery and timing was included to assess whether the differences between surgery types varied across the different timepoints. For all timepoints, an overall test for a difference between surgery types was performed. When this difference was significant, all pairwise testing between the surgery types was performed using a Bonferroni step-down correction to the significance level to account for multiple testing. Estimates of the differences and their associated confidence intervals (using adjusted significance levels) were calculated. Similar analyses were performed to assess differences between the timepoints for the various surgery types. To satisfy the normality assumption, the hs-cTnT values were log-transformed prior to analysis. Estimated differences and confidence intervals were back-transformed to ratios and presented accordingly.
Unless otherwise noted, all tests were two-sided and performed with a significance level of 5%. All statistical analyses were performed using SAS version 9.4 for Windows with SAS/STAT version 4.1.
Results
Four hundred adult patients undergoing different types of cardiac surgery were eligible for inclusion. Nine patients were excluded due to intraoperative, unforeseen changes to the planned operative procedure. For two patients, samples were not collected due to ICU work overload (Figure 1).
Patient characteristics and perioperative data
Table 1 shows the patients’ characteristics, intraoperative details and postoperative variables by the type of surgery and surgical technique. Most patients underwent coronary surgery (on-pump, off-pump, or off-pump robotic-assisted, n = 201, 51.7%). Overall, highly significant differences (P < 0.001) were observed for age, the percentage of redo surgery, statin use, preoperative LVEF and elevated baseline hs-cTnT values (>14 ng/L). Twenty-eight percent of the study population exhibited chronic renal insufficiency.
Characteristics of the patients, intraoperative details and postoperative variables by the type of surgery and surgical technique.
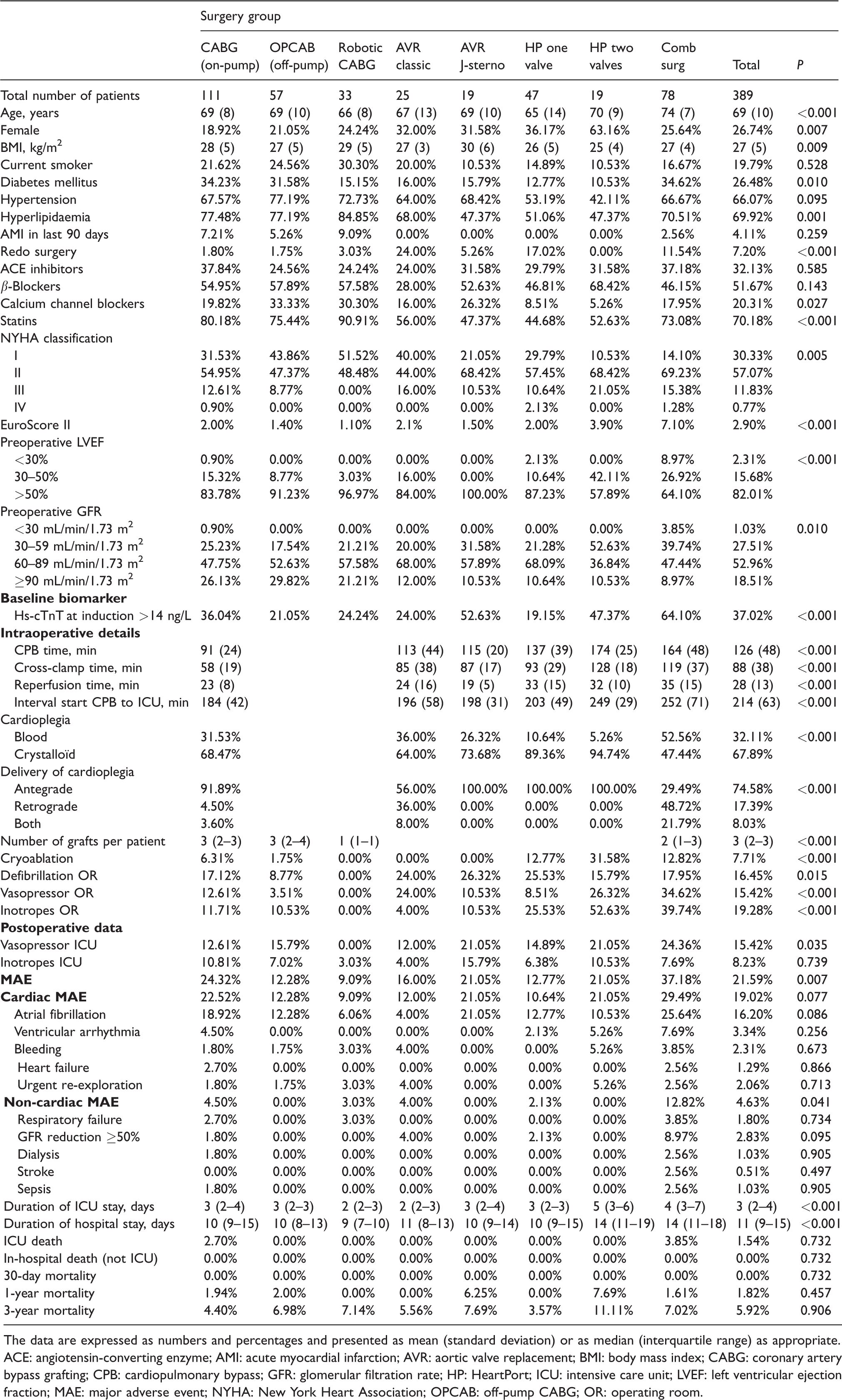
The data are expressed as numbers and percentages and presented as mean (standard deviation) or as median (interquartile range) as appropriate.
ACE: angiotensin-converting enzyme; AMI: acute myocardial infarction; AVR: aortic valve replacement; BMI: body mass index; CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; GFR: glomerular filtration rate; HP: HeartPort; ICU: intensive care unit; LVEF: left ventricular ejection fraction; MAE: major adverse event; NYHA: New York Heart Association; OPCAB: off-pump CABG; OR: operating room.
Intraoperative details
The CPB time and aortic cross-clamp time differed significantly depending on the type of surgery. These durations were the longest in the multiple valve HP group. Cold antegrade crystalloid cardioplegia was the most commonly used myocardial protection strategy. Cryoablation for atrial fibrillation was performed in 7.7% of patients, the highest proportion of which were in the multiple valve HP group (31.6%). Defibrillation for arrhythmias during or after weaning from CPB was performed in 16.5% of the study patients.
Postoperative outcomes
A total of 124 MAEs (100 cardiac and 24 non-cardiac) were observed in 84 different patients (21.6%), mainly in the on-pump CABG group and the combined surgery group. The minimally invasive procedures resulted in almost no non-cardiac MAEs. Isolated valve surgery (aortic and mitral/tricuspid valve) resulted in fewer adverse events compared to CABG and combined surgery, except for atrial fibrillation in the ICU. Although 15 patients (3.8%) developed new ECG evidence (Q and non-Q wave) of ischaemia and were clinically considered PMI cases, only 7 (1.7%) patients met the criteria described by the Third Universal Definition of PMI (a vast majority of whom received CABG surgery). Urgent re-exploration was required in eight patients (2.1%), all due to excessive bleeding.
Six patients (1.5%) died in the ICU. Five of these deaths had a cardiac origin. One patient died after a massive stroke. No other patients died in-hospital. At 12 months and three years of follow-up, six (1.5%) and 17 (4.3%) patients, respectively, had died because of a cardiovascular disease, and seven (1.7%) and an additional six (1.5%) patients, respectively, were lost to follow-up.
High-sensitivity cardiac troponin T
A total of 3477 blood samples were collected during the first 48 h after ICU admission. All patients had a baseline value determined before induction of anaesthesia (T ind). Twenty-four sampling data points were missing among 13 patients. These blood samples were excluded from analyses that involved hs-cTnT at the affected timepoints.
The estimated mean hs-cTnT profiles analysed by a linear mixed model for each surgery type group at each different timepoint are shown in Figure 2. The values by peak timepoint differed significantly depending on the type of surgery. The overall peak timepoint for hs-cTnT occurred 6 h after ICU admission (T6) in all groups. The combined surgery and multiple valve HP groups showed the highest hs-cTnT values at T6 (median 1067.5 (744.9–1455) ng/L and 1166 (743.7–2470) ng/L, respectively). The off-pump robotic-assisted CABG group showed the lowest hs-cTnT value at T6 (median 46.8 (24.4–70.9) ng/L).
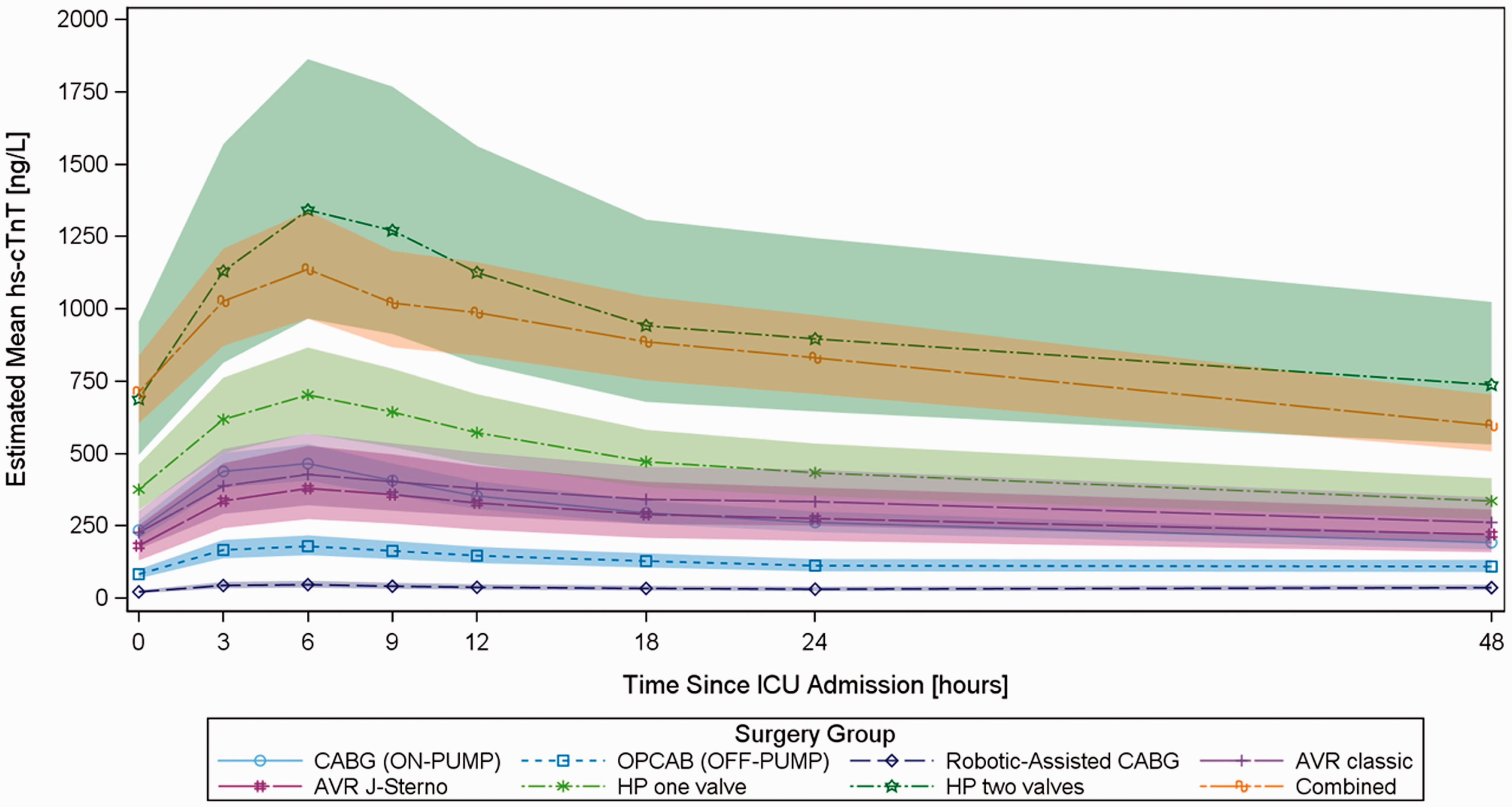
Estimation of the mean high-sensitivity cardiac troponin T profile by a linear mixed model for each surgical type group at each time point. AVR: aortic valve replacement; CABG: coronary artery bypass grafting; HP: HeartPort; OPCAB: off-pump CABG.
The entire study cohort was subdivided into quartiles according to the mean peak postoperative hs-cTnT level (Q1, <140 ng/L; Q2, 140–420 ng/L; Q3, 421–700 ng/L; and Q4, >700 ng/L), as shown in Tables 2 and 3. MAEs (cardiac and non-cardiac) were more frequent in the fourth quartile (Q4) and tended to affect more patients in the combined surgery group (83%). The ICU and hospital stay durations were significantly longer for patients in Q4, but this characteristic did not translate into a significantly poorer long-term outcome. For clinical outcomes, large heterogeneity was observed among the patient population (Table 4). No significant difference in the incidence of PMI was observed between the four quartiles. Patients with non-cardiac MAEs tended to have higher peak hs-cTnT values.
Peak high-sensitivity cardiac troponin T levels by quartile, the type of surgery and surgical technique.

AVR: aortic valve replacement; CABG: coronary artery bypass grafting; hs-cTnT: high-sensitivity cardiac troponin T; HP: HeartPort; OPCAB: off-pump CABG.
Characteristics of the patients, operative details, and postoperative variables by quartiles of the mean peak high-sensitivity cardiac troponin T level.
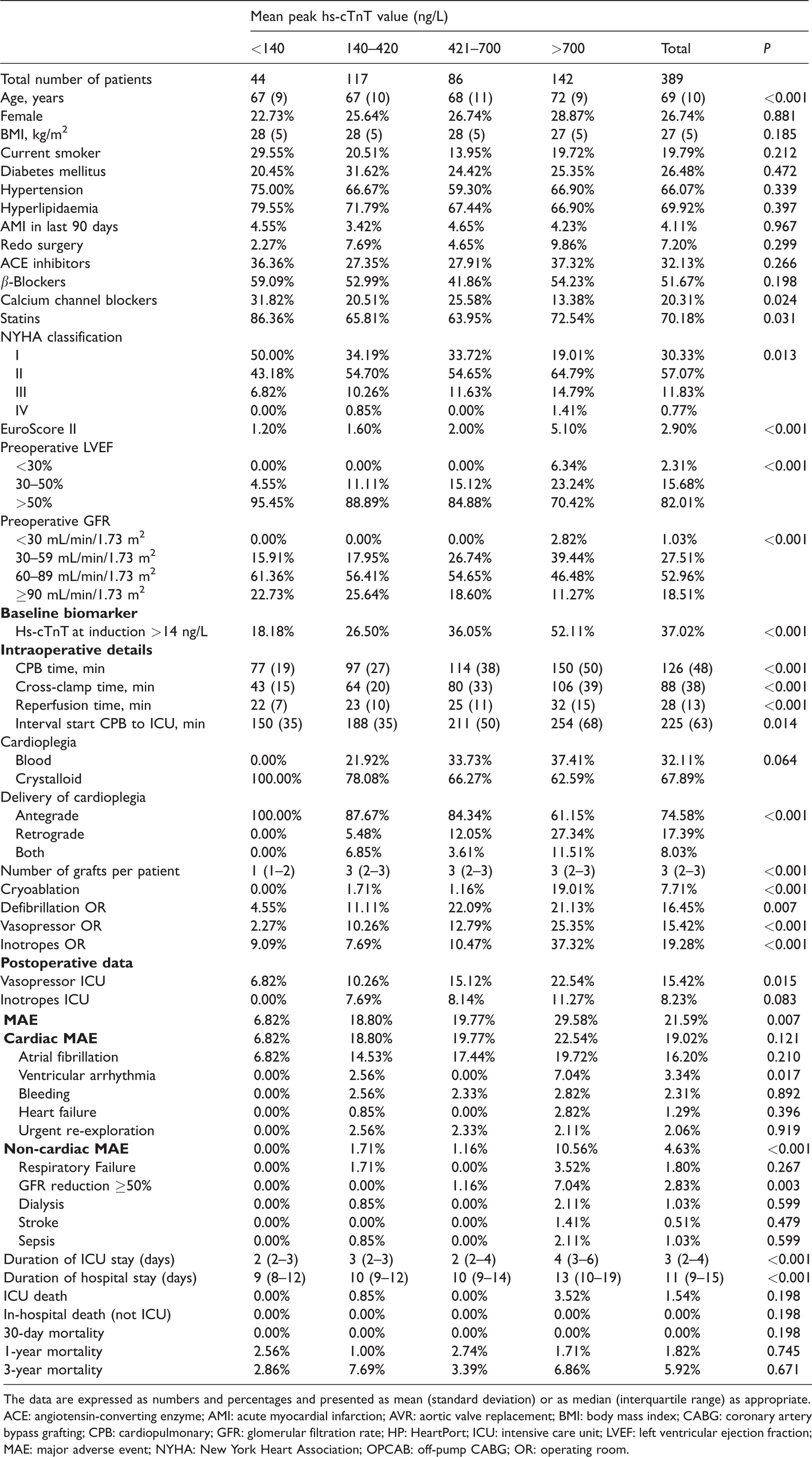
The data are expressed as numbers and percentages and presented as mean (standard deviation) or as median (interquartile range) as appropriate.
ACE: angiotensin-converting enzyme; AMI: acute myocardial infarction; AVR: aortic valve replacement; BMI: body mass index; CABG: coronary artery bypass grafting; CPB: cardiopulmonary; GFR: glomerular filtration rate; HP: HeartPort; ICU: intensive care unit; LVEF: left ventricular ejection fraction; MAE: major adverse event; NYHA: New York Heart Association; OPCAB: off-pump CABG; OR: operating room.
Peak high-sensitivity cardiac troponin T levels by quartile and clinical outcome.
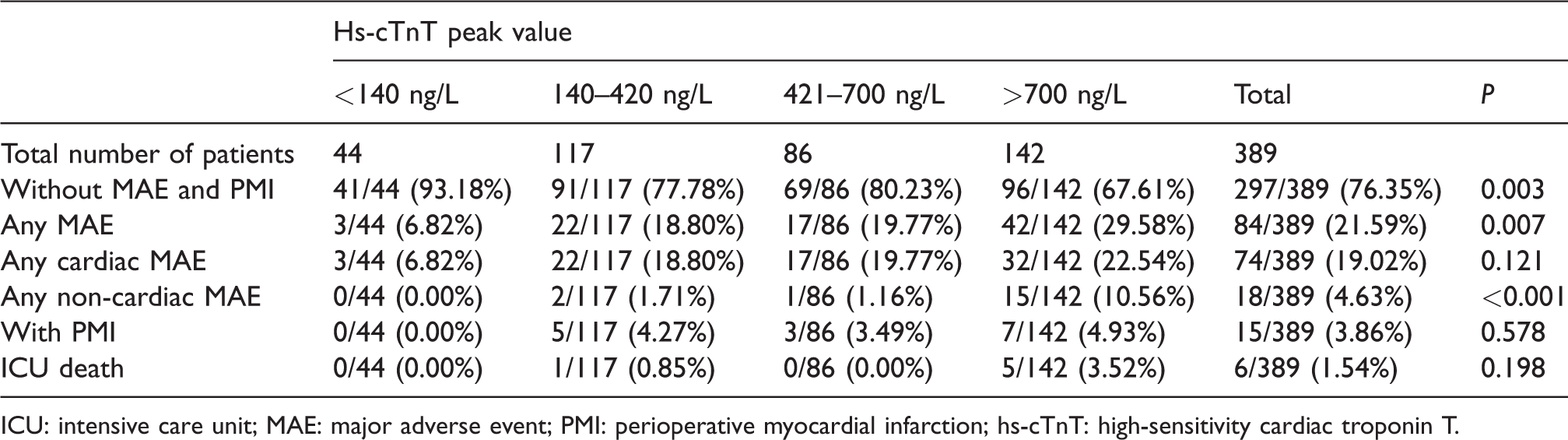
ICU: intensive care unit; MAE: major adverse event; PMI: perioperative myocardial infarction; hs-cTnT: high-sensitivity cardiac troponin T.
Discussion
In this study, we showed that (1) postoperative hs-cTnT release differed significantly depending on the type of cardiac surgery; (2) multiple variables can account for higher postoperative hs-cTnT release, complicating the clinical use of this parameter in the early postoperative setting; and (3) the literature-defined cut-off value for diagnosing CABG-related PMI does not seem to be useful in a real-life clinical setting following different types of cardiac surgery.
Previous studies have shown that a single postoperative peak cTn value at 20–24 h after cardiac surgery is a significant predictor of prolonged postoperative ICU and hospital stays as well as short- and long-term adverse outcomes.21–23 In our study, we demonstrated a consistent hs-cTnT peak timepoint and were able to map a release pattern by regular, postoperative serial sampling. In contrast to most published studies using standard troponin assays, we used the URL to help improve comparability. In spontaneous myocardial infarction, serum levels of hs-cTnT increase within 3–12 h and peak within 16–24 h from the onset of symptoms. 24 In contrast, in our study population, hs-cTnT reached an earlier overall peak at 6 h after ICU admission, or approximately 9–10 h after CPB initiation. Moreover, we showed that hs-cTnT release differs significantly depending on the type of cardiac surgery, and that the magnitude of hs-cTnT release correlated with the expected extent of surgically-induced myocardial injury. In line with previous reports on CABG surgery,25,26 we found lower peak values following off-pump CABG surgery than those after on-pump CABG surgery. For off-pump robotic-assisted CABG surgery, our results support the concept that this minimally invasive technique, which avoids CPB and restricts the procedure to single-vessel revascularization, is accompanied by less surgical trauma and therefore results in lower cardiac biomarker release compared to conventional on-pump CABG and OPCAB surgery, which generally include revascularization of more than one vessel. One retrospective study with 65 patients conducted by Harskamp et al., 27 comparing hybrid coronary revascularization (HCR; on-pump robotic-assisted CABG with percutaneous revascularization) and OPCAB, showed that the median (IQR) release of cardiac troponin I (cTnI) as a ratio of the URL was 3.5 (0.8–9.1) after HCR and 12.8 (6.9–21.8) after OPCAB (P=0.001). 27 In conventional AVR surgery, the placement of sutures into the aortic annulus and right atrium, as well as the CPB and aortic cross-clamp times, contribute to the induced myocardial damage. In our study, no statistically significant differences were observed in the mean peak hs-cTnT values, CPB time or aortic cross-clamp time between conventional and minimally invasive AVR through J-sternotomy. The extent of myocardial injury in mitral valve surgery is expected to be greater than that in most other types of cardiac surgery. Lasocki et al. compared the release of cardiac biomarkers in 502 patients after different cardiac surgical procedures and observed the highest postoperative cTnI concentration in mitral valve repair patients. 22 Even with a minimally invasive technique via HP technology, we encountered higher hs-cTnT peak values after mitral valve surgery; indeed, the extent of injury depended on the size of the atrial incisions, duration of CPB, aortic cross-clamp time and adequacy of myocardial protection.
In addition to factors related to the surgical procedure itself, other mechanisms that influenced the release and clearance of hs-cTnT in our study population can be defined. First, a high degree of variability in the patient characteristics was observed among the different surgical groups. In particular, unfavourable clinical characteristics such as a high EuroScore II and poor LVEF were mostly present in the highest troponin quartile, suggesting that these patients had high myocardial vulnerability. Second, an elevated baseline hs-cTnT value was observed in all study groups, particularly in patients who underwent combined – and thus more extensive – cardiac surgery. Third, moderate to severe renal insufficiency was particularly prominent in the combined and multiple-valve HP groups. Patients with chronic renal insufficiency but without acute coronary artery disease have increased cTn concentrations; 28 thus, in this patient group, a postoperative increase in biomarker levels is difficult to interpret. Acute postoperative renal failure was observed almost exclusively in the combined surgery group. Only a few studies have evaluated the influence of acute kidney injury on hs-cTnT, and these studies have suggested a delay in troponin clearance as the underlying mechanism,29,30 thus leading to higher hs-cTnT values. Fourth, cardiac arrhythmia (and the need for intraoperative cryoablation and/or defibrillation) as well as the use of inotropes is a factor known to induce myocardial injury, 6 and the incidence of cardiac arrhythmia was significantly elevated in the multiple valve HP group.
The biomarker cut-off point for diagnosing CABG-related PMI is controversial; in most published studies, the reported cTn values are well above the arbitrarily proposed cut-off value. When using the hs-cTnT criteria suggested by the Third Universal Definition, we found a PMI incidence rate of only 1.7%. Although all patients developing PMI showed peak hs-cTnT values above the URL (140 ng/L), no clear cut-off value could be differentiated. Nevertheless, 67% of the patients without MAEs showed a peak hs-cTnT level higher than 10× the URL. Furthermore, we also observed that the peak hs-cTnT values in patients with the highest incidence of MAEs were more than 50× the URL. These results are consistent with the findings of other authors. Recently, in a study of 805 patients undergoing isolated or multiple heart valve surgery, Cubero-Callego et al. reported a new hs-cTnT cut-off value (1057 pg/mL at 16 h) above the URL with high sensitivity and specificity for diagnosing PMI in patients with pathological ECG and/or transthoracic echocardiography (TTE) criteria after heart valve surgery. 31 The correlation between the magnitude of myocardial injury and the degree of myocardial instrumentation may explain the high cut-off point in isolated as well as multiple valve surgery. Interestingly, the same study showed that dual criteria (elevation of hs-cTnT levels plus ECG and/or TTE evidence) were more sensitive and specific for the diagnosis of PMI after valve surgery than any single criterion. Omar et al. found that an hs-cTnT level of 3466 ng/L is a diagnostic marker of PMI, 32 although the incidence of PMI was only 2.16%, with most PMI cases occurring after CABG surgeries (84%). Furthermore, in 215 patients undergoing valve surgery, Fellahi et al. found that a mean cTnI value of 14 ng/mL was associated with the likelihood of a severe cardiac event. 33
Our study has several limitations. First, the relatively small number of MAEs, especially PMI, limits the power for estimation of the prognostic role of hs-cTnT. Second, not all patients had a postoperative echocardiographic control, in which case new regional wall motion abnormalities would have been missed. Third, patients with elevated baseline levels of other cardiac biomarkers were not excluded, possibly obscuring the role of hs-cTnT as a marker for diagnosing PMI.
In conclusion, differentiation between cardiac surgery-related necrosis and PMI remains challenging due to the inherent association of cardiac surgery with varying levels of myocardial injury. Depending on the type of cardiac surgery and surgical technique, including conventional and minimally invasive techniques, significant postoperative differences in the magnitude of hs-cTnT release were observed in this study. When the hs-cTnT values collected in our study were compared with the cut-off values for PMI as described in the Third Universal Definition of PMI, this cardiac biomarker seemed to be inappropriate as a stand-alone marker for the diagnosis of PMI. As substantial inter-individual differences were present in pre- and intraoperative patient- and procedure-linked variables in this study, conclusions regarding the reported cardiac biomarker concentrations must be interpreted with caution. This study emphasizes the importance of a clinically reliable biomarker cut-off value for diagnosing PMI, assuming that one exists. More data are therefore required to assess this clinical problem for PMI diagnostic optimization by methods in addition to ECG and echocardiographic criteria.
Footnotes
Acknowledgements
The authors particularly thank the anaesthesiologists and the entire nursing staff of the Anaesthesiology, Critical Care and Cardiovascular Departments; without their diligent efforts, this study would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Except for the reagents for measuring hs-cTnT, which were kindly provided by Roche Diagnostics, Belgium, this study was funded by departmental sources only.