
Abstract
Background:
For critical patients in resuscitation room, the early prediction of potential risk and rapid evaluation of disease progression would help physicians with timely treatment, leading to improved outcome. In this study, it focused on the application of National Early Warning Score on predicting prognosis and conditions of patients in resuscitation room. The National Early Warning Score was compared with the Modified Early Warning Score) and the Acute Physiology and Chronic Health Evaluation II.
Objectives:
To assess the significance of NEWS for predicting prognosis and evaluating conditions of patients in resuscitation rooms.
Methods:
A total of 621 consecutive cases from resuscitation room of Xuanwu Hospital, Capital Medical University were included during June 2015 to January 2016. All cases were prospectively evaluated with Modified Early Warning Score, National Early Warning Score, and Acute Physiology and Chronic Health Evaluation II and then followed up for 28 days. For the prognosis prediction, the cases were divided into death group and survival group. The Modified Early Warning Score, National Early Warning Score, and Acute Physiology and Chronic Health Evaluation II results of the two groups were compared. In addition, receiver operating characteristic curves were plotted. The areas under the receiver operating characteristic curves were calculated for assessing and predicting intensive care unit admission and 28-day mortality.
Results:
For the prognosis prediction, in death group, the National Early Warning Score (9.50 ± 3.08), Modified Early Warning Score (4.87 ± 2.49), and Acute Physiology and Chronic Health Evaluation II score (23.29 ± 5.31) were significantly higher than National Early Warning Score (5.29 ± 3.13), Modified Early Warning Score (3.02 ± 1.93), and Acute Physiology and Chronic Health Evaluation II score (13.22 ± 6.39) in survival group (p < 0.01). For the disease progression evaluation, the areas under the receiver operating characteristic curves of National Early Warning Score, Modified Early Warning Score, and Acute Physiology and Chronic Health Evaluation II were 0.760, 0.729, and 0.817 (p < 0.05), respectively, for predicting intensive care unit admission; they were 0.827, 0.723, and 0.883, respectively, for predicting 28-day mortality. The comparison of the three systems was significant (p < 0.05).
Conclusion:
The performance of National Early Warning Score for predicting intensive care unit admission and 28-day mortality was inferior than Acute Physiology and Chronic Health Evaluation II but superior than Modified Early Warning Score. It was able to rapidly predict prognosis and evaluate disease progression of critical patients in resuscitation room.
Keywords
Introduction
It is always a number of patients attending the general hospital and requiring care in the resuscitation room in China. The conditions of the patients could change rapidly, with a potential risk of deterioration at any time. It is hard to monitor and timely detect the condition progression of critical patients because of the shortage of sufficient space and personnel in the emergency departments. 1 Therefore, the “early warning signal” of critical patients should be identified at early stage. Early detection of risk factor for early deterioration could help to initiate appropriate treatment. 2 Acute Physiology and Chronic Health Evaluation (APACHE II) and Sequential Organ Failure Assessment (SOFA) are commonly used scoring systems for evaluating conditions and prognosis of patients. Such systems were able to predict disease progression and prognosis of critical patients with a high accuracy. One of the major limitations of these scoring systems was that many physiological data were required in addition to biochemical test results. 3 It is impossible to obtain all these parameters quickly in resuscitation room, which limits the application of such accurate scoring systems.
Early Warning Score (EWS) was proposed by Morgan et al. 4 in 1997. EWS was based on the evaluation of heart rate, systolic blood pressure, respiratory rate, body temperature, and awareness of the patients. Preliminary and rapid evaluation of illness condition and prognosis could be performed on the emergency patients. The evaluation results can be rapidly obtained, because all involved physiological parameters can be obtained within minutes. Due to the practicality and effectiveness, EWS was widely applied in the field of first aid. However, there were still limitations of its use. First, criteria were different, such as varied weight of individual parameter. Different criteria would result in inconsistent evaluation results. Second, the sensitivity was relatively low, which was much lower than that of APACHE II system.
EWS was further improved in 2001, which was the Modified Early Warning Score (MEWS). 5 The criteria were preliminarily unified in MEWS. The accuracy of MEWS was improved for evaluating disease progression and prognosis of critical patients in emergency department; however, the total prediction sensitivity was still insufficient. In 2012, the Royal College of Physicians in the United Kingdom has developed National Early Warning Score (NEWS), taking into account the oxygen saturations. 6 Thus, a standardized track and trigger system can be provided with many advantages. First, the disease severity can be preliminarily evaluated. Second, the critical patients can be identified in early stage. Third, the disease progression can be sustainably monitored and timely treated, thus the prognosis can be improved. Nowadays, NEWS has been widely applied in the medical system of commonwealth countries.
NEWS is a rapid and effective prediction system for disease progression, which was suitable for use in the field of emergency. However, as a new system, NEWS lacks sufficient clinical cases for confirmation. The application of NEWS is still at a preliminary stage, especially in China. In our study, hundreds of cases were included, and the results of NEWS, MEWS, and APACHE II were compared for predicting disease progression and prognosis. The value and significance of NEWS was demonstrated for its application in resuscitation room.
Materials and methods
General information
The patients were included from resuscitation room of Xuanwu Hospital, Capital Medical University, during June 2015 to January 2016.
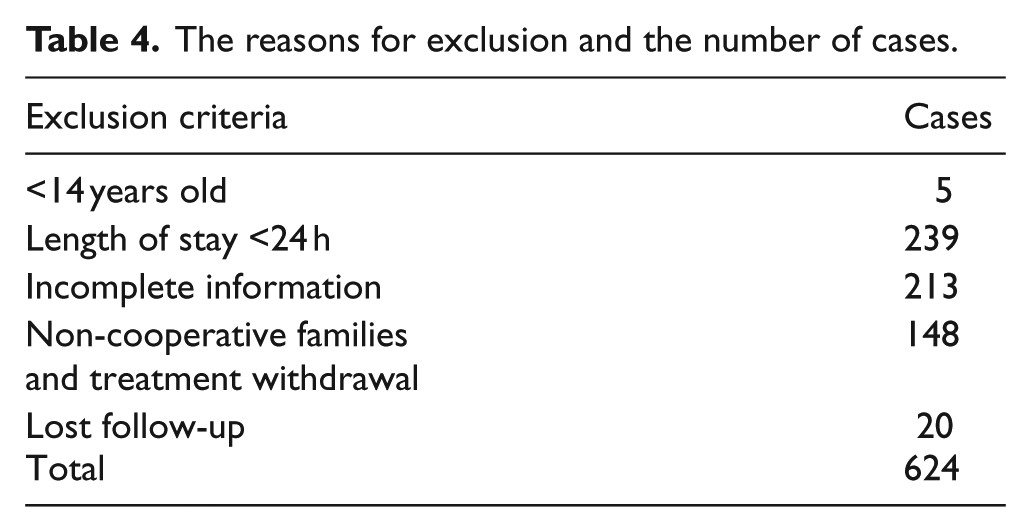
Inclusion criteria: Length of stay of the patient was longer than 24 h. All the clinical laboratory indicators were completed. The informed consent was obtained from all patients or their families. Exclusion criteria: (1) the patient was younger than 14 years old; (2) length of stay was less than 24 h; and (3) incomplete information, including lost follow-up, non-cooperative families and treatment withdrawal. The follow-up lasted for 28 days. All the cases were divided into survival group and death group according to the outcome.
According to MEWS score, the patients were classified into four groups: 0–3, 4–6, 7–9, and >9. According to the NEWS score, the patients were classified into five groups: 0–4, 5–8, 9–12, 13–16, and >16. According to APACHE II score, 7 the patients were classified into four groups: <15, 15–20, 21–25, and >25. The intensive care unit (ICU) admission rate and mortality were compared in different groups of the three evaluation systems.
Research methods
The demographic information of all the included cases was collected, including age, gender, and diagnosis. The physiological parameters included body temperature, respiratory rate, systolic blood pressure, heart rate, oxygen saturation, and whether there was an oxygen therapy (if the oxygen saturation was detected during oxygen therapy, 2 points should be added to the aggregate; whether an oxygen therapy should be given or specific implementation measure should refer to the Emergency oxygen therapy guidelines published by British Thoracic in 2008), awareness (A: awake; V: verbal response; P: painful response; U: unresponsive) scores. The biochemical parameters included serum
All the cases were evaluated by the MEWS (Table 1), NEWS (Table 2), and APACHE II score (Table 3). The ICU admission rate and mortality during hospitalization of all the included cases were recorded.
Modified Early Warning Score (MEWS).
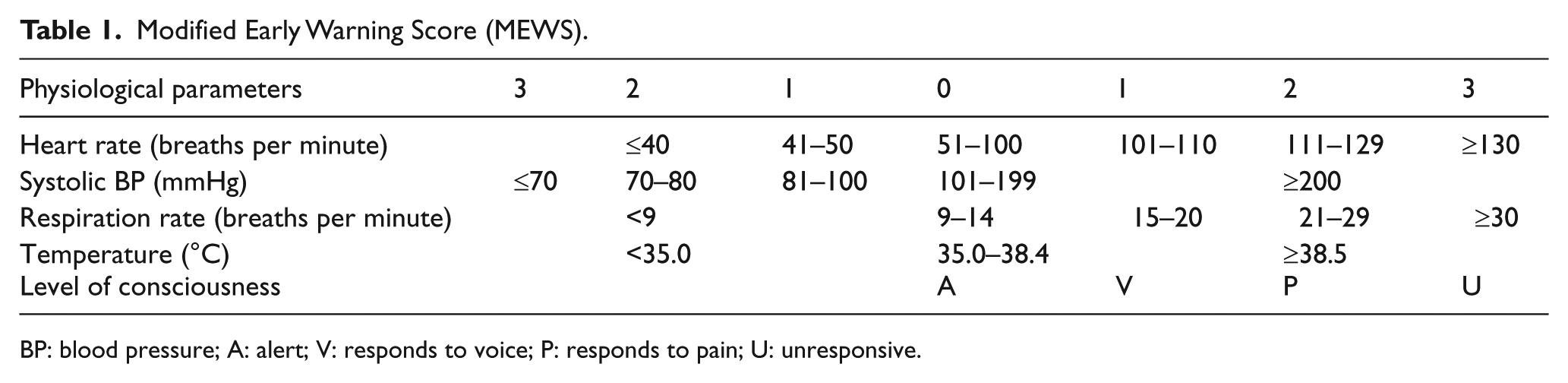
BP: blood pressure; A: alert; V: responds to voice; P: responds to pain; U: unresponsive.
National Early Warning Score (NEWS).
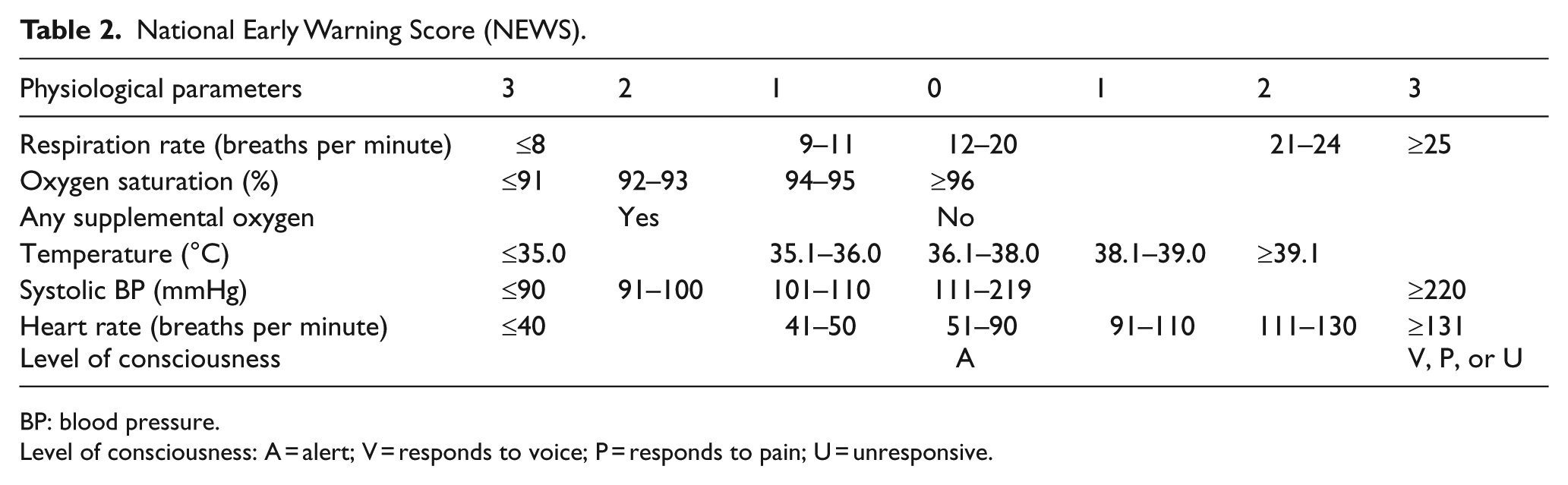
BP: blood pressure.
Level of consciousness: A = alert; V = responds to voice; P = responds to pain; U = unresponsive.
The APACHE II Severity of Disease Classification System.
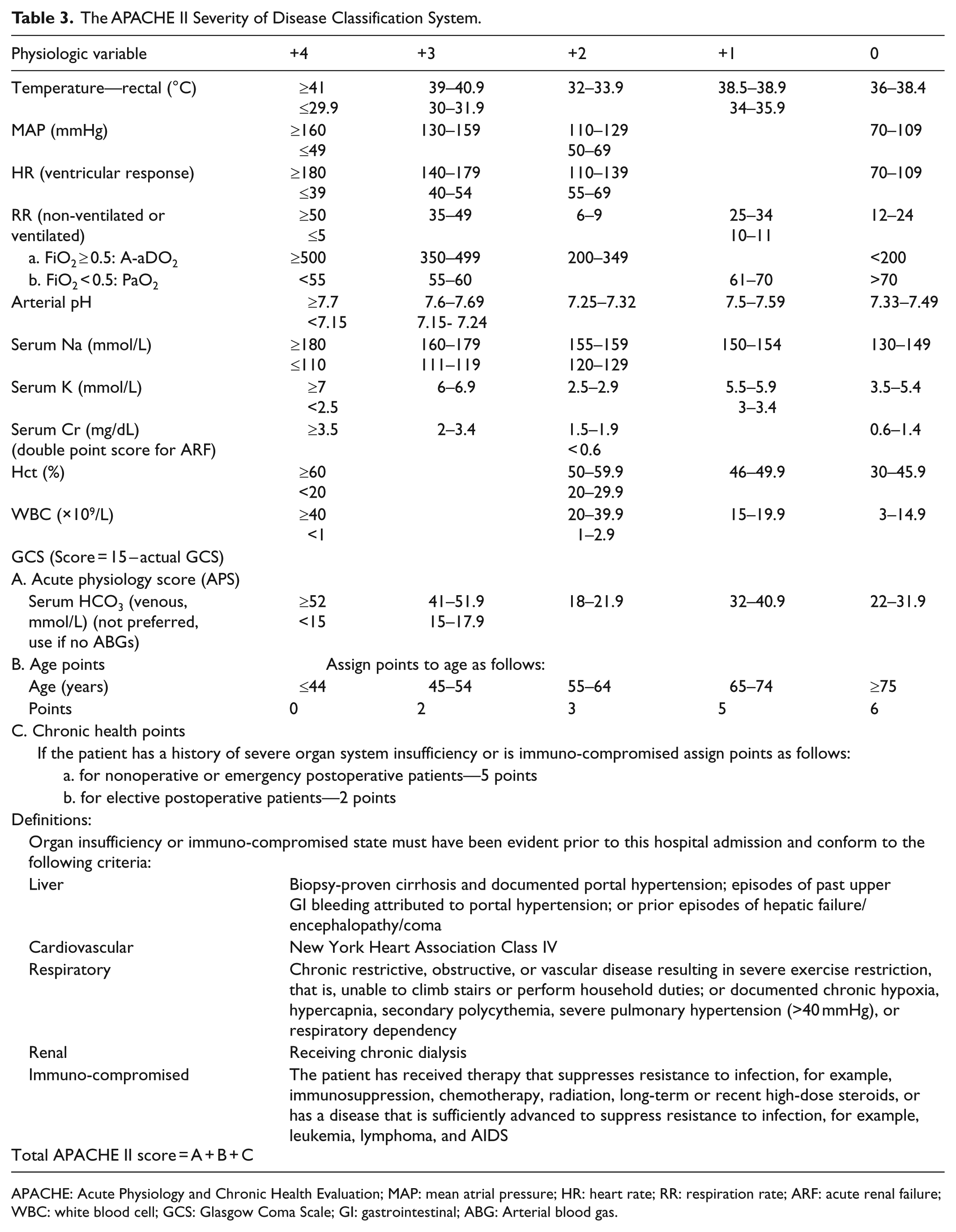
APACHE: Acute Physiology and Chronic Health Evaluation; MAP: mean atrial pressure; HR: heart rate; RR: respiration rate; ARF: acute renal failure; WBC: white blood cell; GCS: Glasgow Coma Scale; GI: gastrointestinal; ABG: Arterial blood gas.
Statistical methods
The statistical analysis was performed using SPSS 19.0 and MedCalc statistical software (v12.3.0.0). The data were expressed as mean ± standard deviation
Result
General information
During June 2015 to January 2016, a total of 1246 cases were treated in resuscitation room of Xuanwu Hospital, Capital Medical University. A total of 621 cases meeting the inclusion criteria were included, with 375 male and 246 female. The reasons for exclusion and the number of cases are shown in Table 4. The cases were aged between 14 and 99 years old with an average of 64.54 ± 14.38 years. There were 258 cases with neurological diseases (41.5%), 117 cases with cardiovascular disease (18.8%), 95 cases with respiratory diseases (15.4%), 67 cases with digestive diseases (10.8%), 46 cases with urinary system disease (7.4%), and 38 cases of others and unknown diseases (6.1%). Finally, there were 58 cases of death and 563 cases of survival; 138 cases were admitted to the ICU; 483 cases were admitted to the general ward or cured to discharge from hospital. Both the ICU admission and mortality of patients were significantly uplifted with the increased scores obtained in NEWS, MEWS, and APACHE II (p < 0.01, Table 5).
The reasons for exclusion and the number of cases.
The ICU admission rate and mortality corresponding to different scores obtained in NEWS, MEWS, and APACHE II.
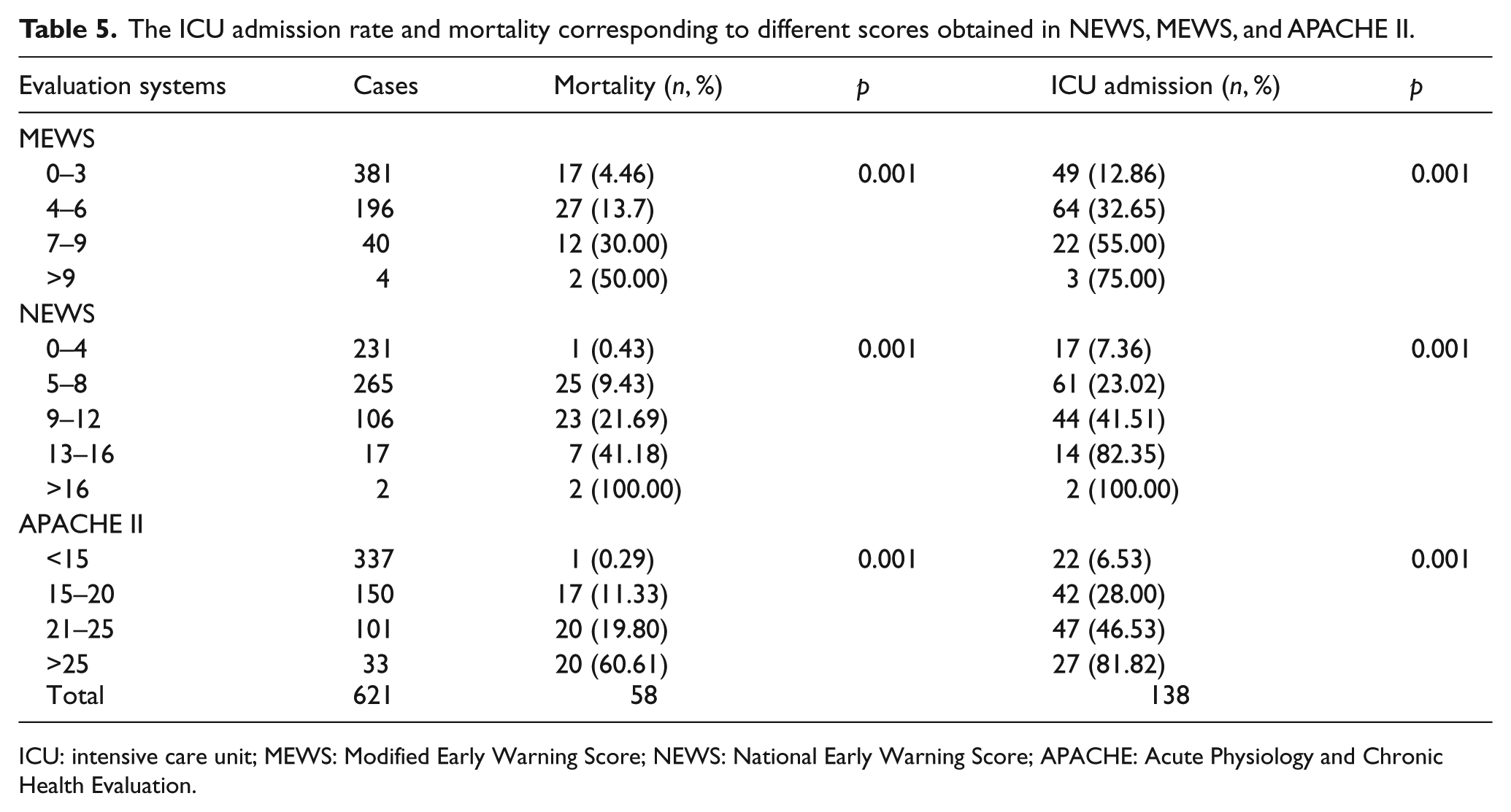
ICU: intensive care unit; MEWS: Modified Early Warning Score; NEWS: National Early Warning Score; APACHE: Acute Physiology and Chronic Health Evaluation.
The results of NEWS, MEWS, and APACHE II between death group and survival group
For the death group, NEWS result was 9.50 ± 3.08, MEWS result was 4.87 ± 2.49, and APACHE II result was 23.29 ± 5.31. All were significantly higher than those in the survival group, with NEWS result of 5.29 ± 3.13, MEWS result of 3.02 ± 1.93, and APACHE II result of 13.22 ± 6.39 (p < 0.01, Table 6).
The comparison of NEWS, MEWS, and APACHE II between death group and survival group.
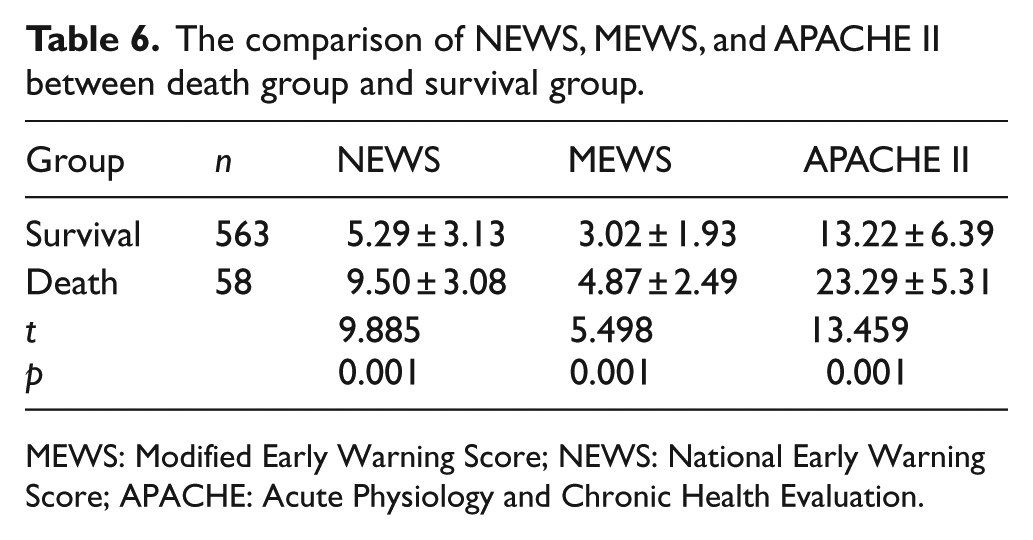
MEWS: Modified Early Warning Score; NEWS: National Early Warning Score; APACHE: Acute Physiology and Chronic Health Evaluation.
The performances in predicting ICU admission
The AUC of all three systems were compared. For the NEWS, the AUC for predicting ICU admission was 0.760 and the best cut-off point was 7, with a sensitivity of 58.7% and specificity of 79.3%. For the MEWS, the AUC was 0.729 and the best cut-off point was 3, with a sensitivity of 64.5% and specificity was 68.7%. For the APACHE II score, the AUC was 0.817 and the best cut-off point was 16, with a sensitivity of 76.1% and specificity of 74.1%. The accuracy of the NEWS in predicting ICU admission was lower than the APACHE II score (Z = 2.354, p = 0.019), but higher than the MEWS (Z = 2.269, p = 0.023; Figure 1).
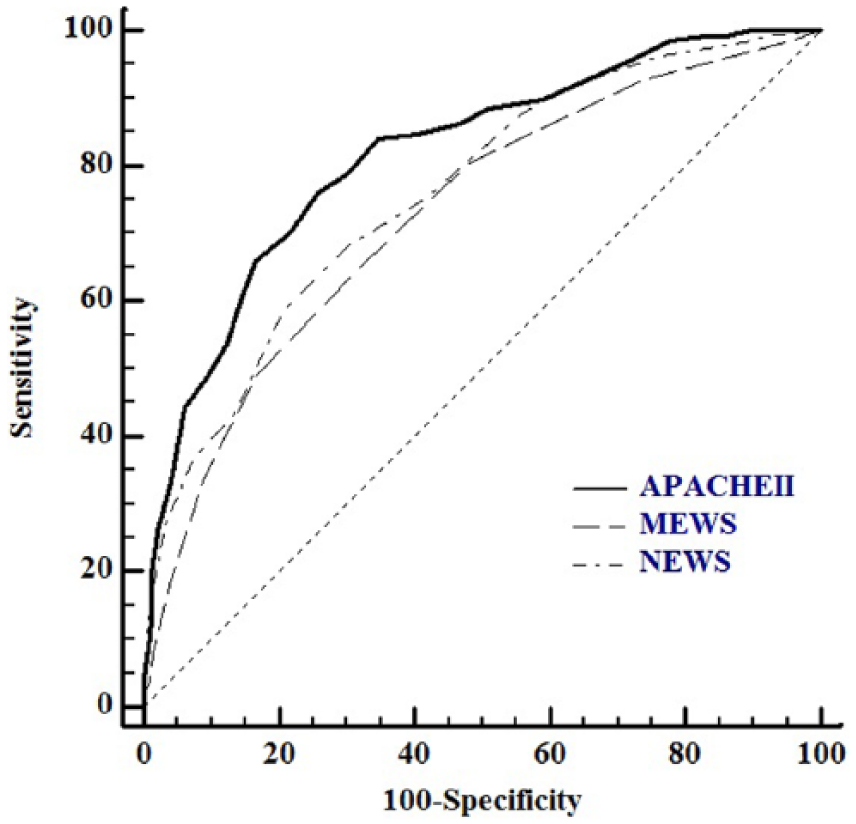
The comparison of NEWS, MEWS, and APACHE II on area under ROC curve for predicting ICU admission.
The comparison of area under ROC curve for predicting death
For the NEWS, the AUC for death prediction was 0.827 and the best cut-off point was 6, with a sensitivity of 84.5% and specificity of 66.7%. For the MEWS, the AUC was 0.723 and the best cut-off point was 4, with a sensitivity of 56.9% and specificity was 79.4%. For APACHE II score, the AUC was 0.883 and the best cut-off point was 18, with a sensitivity of 81.03% and specificity of 77.98%. Comparing the three systems, the accuracy of NEWS for predicting death was lower than the APACHE II score (Z = 2.243, p = 0.025), but higher than the MEWS (Z = 3.316, p = 0.001; Figure 2).
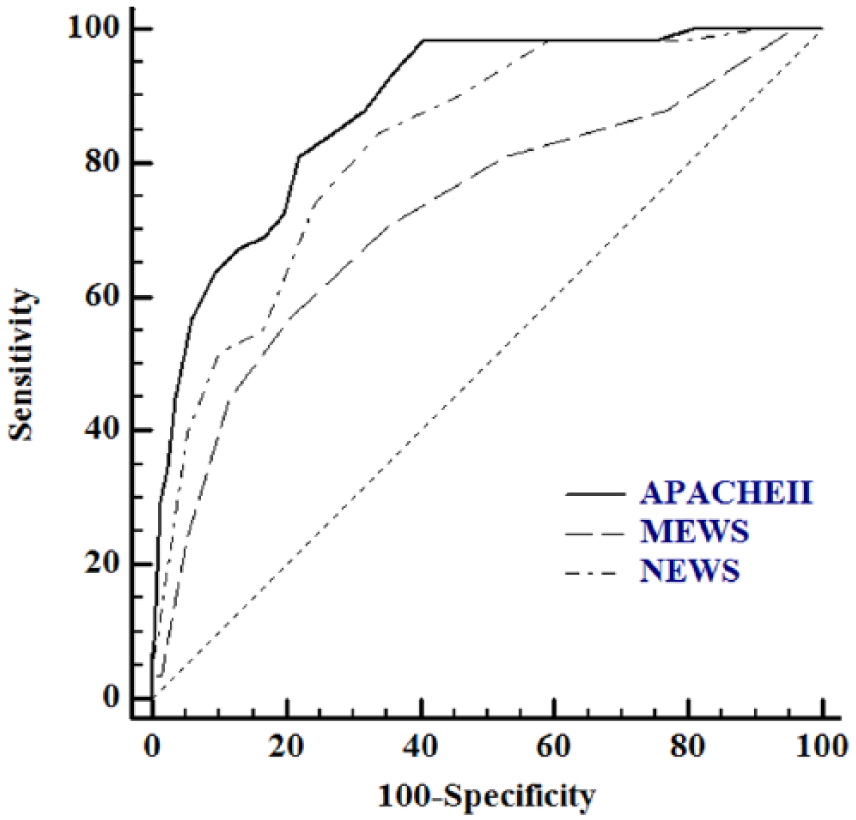
The comparison of NEWS, MEWS, and APACHE II on area under ROC curve for predicting death.
Discussion
In the emergency department, the patients were generally in a critical and complicated condition. It puts forward high requirement to the physician. The disease progression and risk of deterioration should be accurately determined and predicted. In addition, timely, correct, and effective treatment should be made for saving the lives of critical patients, as well as improving prognosis. 8 One of the most commonly applied systems for evaluating disease severity and prognosis is the APACHE II score. The system is accurate and effective. However, so many parameters were required that APACHE II may take around 24 h, which limited its application and practical value in emergency departments. 3 Ideally, the NEWS and MEWS scores should be no more than 5 min, the time required to get APACHE II score is more than 2 h.
EWS is able to rapidly determine the condition of patients in emergency department. The prognosis can also be preliminarily evaluated. EWS has been widely applied for rapid data acquisition. In 2001, MEWS was proposed by Subbe as a modified EWS. MEWS has preliminarily standardized the EWS, which reduced the prediction error due to the various standards and inconsistent weight of individual parameter. The prediction accuracy of disease progression and prognosis has been improved.8–10 However, the sensitivity of the MEWS was relatively low. In 2012, the Royal College of Physicians in the United Kingdom has developed NEWS, taking into account the oxygen saturations. 6 Until now, NEWS has become more and more popular for better accuracy.
One study has compared the evaluation ability of critical diseases between NEWS and a typical MEWS. The AUC for predicting death in NEWS was 0.848, while it was 0.815 in MEWS. 11 NEWS was a much more sensitive system than MEWS, which was contributed to the addition of oxygen saturation.
The similar results were observed in our study. In MEWS, the score in death group was significantly higher than that in survival group (p = 0.001), indicating the capacity of evaluation. However, compared with NEWS, the AUC of MEWS were smaller, both in predicting ICU admission and death. Therefore, the application value and sensitivity of the MEWS should be less significant than NEWS. It could be explained by the addition of oxygen saturation and oxygen therapy considerations in the NEWS. In addition, the weight of included parameters were thus varied and improved. All these factors improved the sensitivity of prediction.
Other studies have also suggested a better application value of NEWS on disease progression prediction. A retrospective analysis has been performed on 35,585 cases. 12 It indicated a significant value of NEWS on predicting cardiac events, ICU admission, and mortality. Another study has been performed on 1684 patients with pre-hospital emergency care. The patients with high NEWS score suffered a significantly uplifted ICU admission rate, 48-h mortality, and 30-day mortality. It indicated a new application value of NEWS in pre-hospital emergency care. 13
The NEWS was also compared with APACHE II score, which has been considered as a gold standard for disease and prognosis prediction. 7 APACHE II score has been the most common clinical system for evaluating disease and prognosis of critical patients. However, many parameters were required so that the data could not be rapidly obtained. Therefore, the application of APACHE II in triage and care level improvement has been limited. On the contrary, the parameters required by NEWS are easy to be obtained, which would be more significant in rapid triage and condition evaluation. In our result, for NEWS, AUC for predicting ICU admission and death was 0.760 and 0.827, indicating medium prediction ability. The AUC of NEWS was higher than that in MEWS, while lower than that in APACHE II score (p < 0.05), indicating a prediction ability of APACHE II > NEWS > MEWS.
However, some limitations have been also observed in NEWS and it is susceptible to interference. First, NEWS evaluates without taking into account the age. For patients with different ages, prognosis would be varied even with same NEWS score. Some study suggested that age should be considered in NEWS. 1 point should be added to the aggregate for the patients between 10 and 19 years old. Then, 1 point should be added for each increased 10 years. After considering the age, the area under curve for evaluating ICU admission rate, admission mortality, 30-day mortality rate, and 90-day mortality rate were significantly higher than that of without considering age factor. In addition, it was significantly correlated with the result of APACHE II system (r = 0.420, p < 0.001). 14 Still, large-scale clinical study should be further performed to explore how to include the age factor into NEWS system. Second, NEWS works with different prediction ability for various diseases. Liu et al. 15 considered that NEWS enjoyed a relatively strong prediction ability on prognosis of respiratory diseases, with an area under ROC curve of 0.885; while the prediction ability on cardiovascular disease was relatively weak, with an area under ROC curve of 0.798. However, another study has obtained contrary results. It considered that NEWS should be weak in predicting chronic hypoxic respiratory diseases. The patient may be stable even at the warning threshold of NEWS. Because the patient has adapted to long-term hypoxia and the oxygen saturation has been in a low state, the uplifted NEWS score would not be fully correlated with the patient’s condition. 16 However, further study should be performed to draw the final conclusions. Multiple center and large data studies should be conducted for a more accurate conclusion in the future.
Conclusion
In short, the prognosis and illness conditions prediction ability of the NEWS was lower than the APACHE II score, but superior to the MEWS. NEWS can provide rapid evaluation on the ill state of critical patients in resuscitation room. Thus, the potential critical patients can be screened in earlier stage, resulting in timely treatment and improved prognosis.
Footnotes
Acknowledgements
We thank Dr Yuan Min and Dr Hu Shaobao for their help with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are included in this article (and its supplementary information files).
Informed consent
Informed consent has been obtained from patients and their families, and the informed consents have been signed.