
Abstract
Introduction
The National Early Warning Score (NEWS) was introduced in 2012 by the Royal College of Physicians in the United Kingdom. It improves the assessment accuracy in acute illness and facilitates early detection of clinical deterioration. This study aimed to evaluate the prognostic value of NEWS in predicting outcomes among patients diagnosed with coronavirus disease 2019 (COVID-19) and to analyze the clinical characteristics and risk factors associated with mortality.
Methods
This retrospective cohort study analyzed the clinical data from patients with COVID-19 admitted to the emergency resuscitation room of Beijing Luhe Hospital, Capital Medical University, between December 2022 and January 2023. Data included initial laboratory test results obtained within 1 h of admission, chest computed tomography findings, NEWS, Modified Early Warning Score (MEWS), and quick Sequential Organ Failure Assessment (qSOFA) score. Receiver operating characteristic curves were used to evaluate the predictive performance of NEWS, MEWS, and qSOFA for 30-day all-cause mortality. Patients were categorized into survivor and nonsurvivor groups. Differences in laboratory parameters and imaging features between the two groups were compared, and logistic regression was employed to identify independent risk factors for prognosis.
Results
A total of 446 patients were enrolled, including 219 survivors and 227 nonsurvivors. The area under the receiver operating characteristic curve (AUROC) for predicting mortality was 0.945 (95% confidence interval: 0.926–0.963) for NEWS, which was significantly higher than those for MEWS (0.903, 95% confidence interval: 0.877–0.929) and qSOFA (0.902, 95% confidence interval: 0.881–0.923) (p < 0.05). No significant difference was observed between the AUROCs of MEWS and qSOFA. Multivariate logistic regression analysis identified NEWS, white blood cell count, platelet count, D-dimer level, comorbidities (respiratory diseases and diabetes), and clinical classification as independent risk factors for COVID-19 prognosis (all p < 0.05). Moreover, the proportion of patients with bilateral lung involvement exceeding 50% on chest computed tomography was significantly higher in the nonsurvivor group (81.8%, p < 0.001).
Conclusion
Early application of NEWS combined with key laboratory indicators is valuable for assessing disease severity and predicting prognosis in patients with COVID-19.
Keywords
Introduction
Since December 2019, coronavirus disease 2019 (COVID-19) has remained a persistent global public health challenge. Following the comprehensive adjustment of China’s epidemic control policies on 7 December 2022, the country experienced its first wave of infections between December 2022 and January 2023. As the primary point of care for critically ill patients, the emergency department requires rapid and accurate risk-stratification tools to optimize resource allocation, facilitate precise treatment, and improve patient outcomes.
The National Early Warning Score (NEWS) and Modified Early Warning Score (MEWS) are widely used clinical tools for early identification and dynamic monitoring of critical illness;1,2 whereas the quick Sequential Organ Failure Assessment (qSOFA) score is commonly applied for sepsis screening. 3 Although the predictive value of these scoring systems has been validated in numerous studies, their performance may be influenced by factors such as viral mutations, population-level immunity, and regional disparities in healthcare resources. However, evidence validating these scoring systems, particularly in the Chinese COVID-19 patient population, remains limited.
Therefore, this retrospective study analyzed clinical data from patients with COVID-19 admitted to the emergency resuscitation room of Beijing Luhe Hospital, Capital Medical University, between December 2022 and January 2023. This study aimed to systematically evaluate the prognostic performance of NEWS, MEWS, and qSOFA and to further identify independent risk factors associated with patient outcomes, thereby providing evidence to support early detection of high-risk patients and the rational allocation of emergency medical resources.
Data and methods
General data
This retrospective study enrolled consecutive patients with COVID-19 who were admitted to the emergency resuscitation room of Beijing Luhe Hospital, Capital Medical University, between December 2022 and January 2023. Patients were categorized into survivor and nonsurvivor groups based on all-cause mortality within 30 days of admission. According to the inclusion criteria, all patients treated in the emergency resuscitation room during the study period who had a confirmed diagnosis of COVID-19 using reverse transcription polymerase chain reaction testing, in accordance with the “Diagnosis and Treatment Protocol for Novel Coronavirus Infection (Trial Version 10),” were enrolled. 4 Exclusion criteria were as follows: (a) inability to obtain initial vital signs at admission or laboratory results within 1 h due to critical illness, death, or refusal to cooperate; (b) age <18 years;.(c) loss to follow-up within 30 days, resulting in an indeterminable study outcome. This study was conducted in accordance with the ethical standards of the Declaration of Helsinki (1975, as revised in 2024) and was approved by the Ethics Committee of Luhe Hospital, Capital Medical University (Approval Number: 2024-LHKY-001-01). All patient data were deidentified to ensure anonymity. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 5
Observation indicators
Data were obtained through analysis of electronic medical records. Upon admission to the emergency department, baseline data were collected, including vital signs such as mental status, body temperature, heart rate, respiratory rate, blood pressure, and peripheral oxygen saturation. These parameters were used to calculate the NEWS, MEWS, and qSOFA score.
NEWS 6 consists of seven parameters: heart rate, respiratory rate, oxygen saturation, supplemental oxygen therapy, body temperature, systolic blood pressure, and level of consciousness. Each parameter is scored from 0 to 3, except for supplemental oxygen therapy, which is scored from 0 to 2. The aggregate NEWS ranges from 0 to 20.
MEWS 7 comprises five parameters: body temperature, respiratory rate, heart rate, systolic blood pressure, and level of consciousness. Body temperature is scored from 0 to 2, whereas the remaining four parameters are scored from 0 to 3, yielding a total score ranging from 0 to 14.
qSOFA includes three components, each assigned 1 point when present: respiratory rate ≥22 breaths/min, systolic blood pressure ≤100 mmHg, and an altered mental status (defined as disorientation or a reduced response to stimuli). The total qSOFA score ranges from 0 to 3.
All enrolled patients underwent evaluations for complete blood count, biochemical profiling, and blood gas analysis within 1 h of admission. The following parameters were measured: white blood cell (WBC) count, neutrophil (NEU) count, lymphocyte (LYM) count, neutrophil-to-lymphocyte ratio (NLR), platelet (PLT) count, C-reactive protein (CRP), procalcitonin (PCT), D-dimer, albumin (ALB), alanine aminotransferase(ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), creatine kinase-MB (CK-MB), blood urea nitrogen (BUN), serum creatinine (Scr), potential of hydrogen (pH), partial pressure of carbon dioxide (pCO2), partial pressure of oxygen (pO2), and lactate (Lac). The specific procedures were as follows:
Complete blood count. Peripheral venous blood samples were collected in ethylenediaminetetraacetic acid (EDTA-K2) anticoagulant vacuum tubes. Analysis was performed using the Mindray BC-5390 CRP fully automated hematology analyzer, which employs electrical impedance and flow cytometry (with fluorescent staining) for cell counting and differentiation. Biochemical testing. Peripheral venous blood samples were collected in coagulation-promoting vacuum tubes. Samples were centrifuged at 3000 r/min for 10 min at room temperature to separate the serum. Biochemical analysis was conducted using the Beckman Coulter AU5800 fully automated biochemical analysis system. Blood gas analysis. Arterial blood samples were obtained from radial or femoral artery using preheparinized Westmed blood gas syringes and were immediately analyzed using the Radiometer ABL90 FLEX blood gas analyzer to determine pH, pO2, pCO2, and Lac.
Computed tomography (CT) was performed using a Philips UCT 530+ 40-slice CT scanner. Clinical classification was performed according to the diagnosis and treatment protocol for novel coronavirus infection (Trial Version 10). 4
Statistical analyses
A prospective sample size calculation was not performed; however, post hoc evaluation confirmed the robustness of the data for multivariate modeling. The final model incorporated 22 independent variables. With 227 observed endpoint events (deaths), the events-per-variable (EPV) ratio was 10.32, exceeding the conventional threshold of 10. This indicates that the sample size was adequate for reliable parameter estimation and ensures the stability of the final model.
Receiver operating characteristic (ROC) curves were generated for the NEWS, MEWS, and qSOFA score to assess their predictive performance for mortality in patients with COVID-19. DeLong’s test was applied to compare the areas under the respective ROC curves, evaluating differences in the discriminatory ability among the three scoring systems. Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS) software, version 23.0. Continuous variables with a normal distribution were analyzed using the independent samples t-test. Non-normally distributed variables were presented as median values with interquartile ranges (IQRs; Q1, Q3) and compared using the Mann–Whitney U test. Categorical variables were expressed as percentages, and intergroup differences were analyzed using the chi-squared test. Variables with a p-value <0.05 in univariate analyses and no evidence of multicollinearity in bivariate analyses, along with clinically meaningful variables with sufficient event counts, were included in the multivariable logistic regression model to identify independent predictors of mortality. Model calibration was evaluated using the Hosmer-Lemeshow goodness-of-fit test. Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs).A two-sided p-value <0.05 was considered statistically significant.
Results
General information
A total of 446 patients were included in this study, as illustrated in the study flow diagram (Figure 1). The baseline clinical characteristics of the study population are summarized in Table 1. The overall cohort had a median age of 79 years (IQR: 71, 86), and 66.8% of patients were male. Significant differences were observed between the survivor and nonsurvivor groups in terms of demographic characteristics, clinical classifications, comorbidities, laboratory parameters, and the three early warning scores. Compared with survivors, nonsurvivors demonstrated a significantly higher prevalence of respiratory diseases (including chronic obstructive pulmonary disease, asthma, interstitial lung fibrosis, and pulmonary embolism), diabetes, and cerebrovascular disease as well as a greater proportion of severe and critical clinical types (p < 0.05). In addition, the nonsurvivors exhibited significantly higher WBC and NEU counts; NLR; CRP, PCT, D-dimer, AST, CK-MB, BUN, Scr, and Lac levels; and NEWS, MEWS, and qSOFA score; whereas they demonstrated significantly lower LYM and PLT counts and ALB, pH, pCO2, and pO2 levels (p < 0.05).

The study flow diagram.
Baseline characteristics of the study population (N = 446).

IQR: interquartile range; WBC: white blood cell; NEU: neutrophil; LYM: lymphocyte; NLR: neutrophil-to-lymphocyte ratio; PLT: platelet; CRP: C-reactive protein; PCT: procalcitonin; ALB: albumin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; TBIL: total bilirubin; CK-MB: creatine kinase-MB; Scr: serum creatinine; BUN: blood urea nitrogen; pH: potential of hydrogen; pCO2: partial pressure of carbon dioxide; pO2: partial pressure of oxygen; Lac: lactate; NEWS: National Early Warning Score; MEWS: Modified Early Warning Score; qSOFA: quick Sequential Organ Failure Assessment.
Predictive performance of NEWS, MEWS, and qSOFA for mortality in patients with COVID-19
ROC curves were generated to evaluate the predictive ability of the three scoring systems for mortality, and the areas under the receiver operating characteristic curve (AUROC) were calculated (Figure 2). The AUROC values for all three scoring systems exceeded 0.9, demonstrating excellent predictive performance for COVID-19 mortality. Pairwise comparisons using DeLong’s test indicated that NEWS exhibited significantly superior predictive accuracy compared with those with MEWS and qSOFA score (p < 0.05), whereas no statistically significant difference was observed between MEWS and qSOFA (Table 2). At an optimal cutoff value of 5.5, NEWS predicted mortality with a sensitivity of 97.8% and a specificity of 74.0%.

ROC curves of NEWS, MEWS, and qSOFA for predicting mortality in patients with COVID-19.
Predictive performance of NEWS, MEWS, and qSOFA score for mortality in patients with COVID-19.

NEWS: National Early Warning Score; MEWS: Modified Early Warning Score; qSOFA: quick Sequential Organ Failure Assessment; COVID-19: coronavirus disease 2019.
Multivariable logistic regression analysis of factors associated with 30-day mortality in patients with COVID-19
In univariate analysis of all variables presented in Table 1, factors with p <0.05 were selected for multicollinearity assessment. The variance inflation factor (VIF) for MEWS and qSOFA exceeded 5, indicating significant multicollinearity. Therefore, these variables were excluded from the multivariate model. The final binary logistic regression model included comorbidities (respiratory diseases, diabetes mellitus, and cerebrovascular disease), clinical classification, and all laboratory parameters except ALT and pCO2. The Hosmer-Lemeshow goodness-of-fit test yielded a p-value of 0.986, indicating no significant deviation between the model’s predictions and the observed outcomes, thereby demonstrating good calibration. After adjusting for potential confounders, NEWS, WBC and PLT counts, D-dimer levels, comorbidities (respiratory disease and diabetes), and clinical classification were identified as independent risk factors for COVID-19 mortality (p < 0.05). Specifically, each one-unit increase in NEWS, WBC count, and D-dimer level was associated with a 2.134-fold (OR = 2.134), 1.173-fold (OR = 1.173), and 1.275-fold (OR = 1.275) increase in the mortality risk, respectively. In contrast, each one-unit increase in the PLT count was associated with a 0.7% reduction in mortality risk (OR = 0.993). Patients with preexisting respiratory disease had a 4.710-fold higher risk of death (95% CI: 1.618–13.712) and those with diabetes had a 4.413-fold increased risk (95% CI: 1.686–11.554). Using the “ordinary type” as the reference, the “severe type” (OR = 30.104, 95% CI: 2.487–364.326) and “critical type” (OR = 540.405, 95% CI: 25.793–11,322.493) were significantly associated with markedly elevated mortality risks. Detailed results are provided in Table 3.
Multivariable logistic regression analysis of factors associated with 30-day mortality in patients with COVID-19.
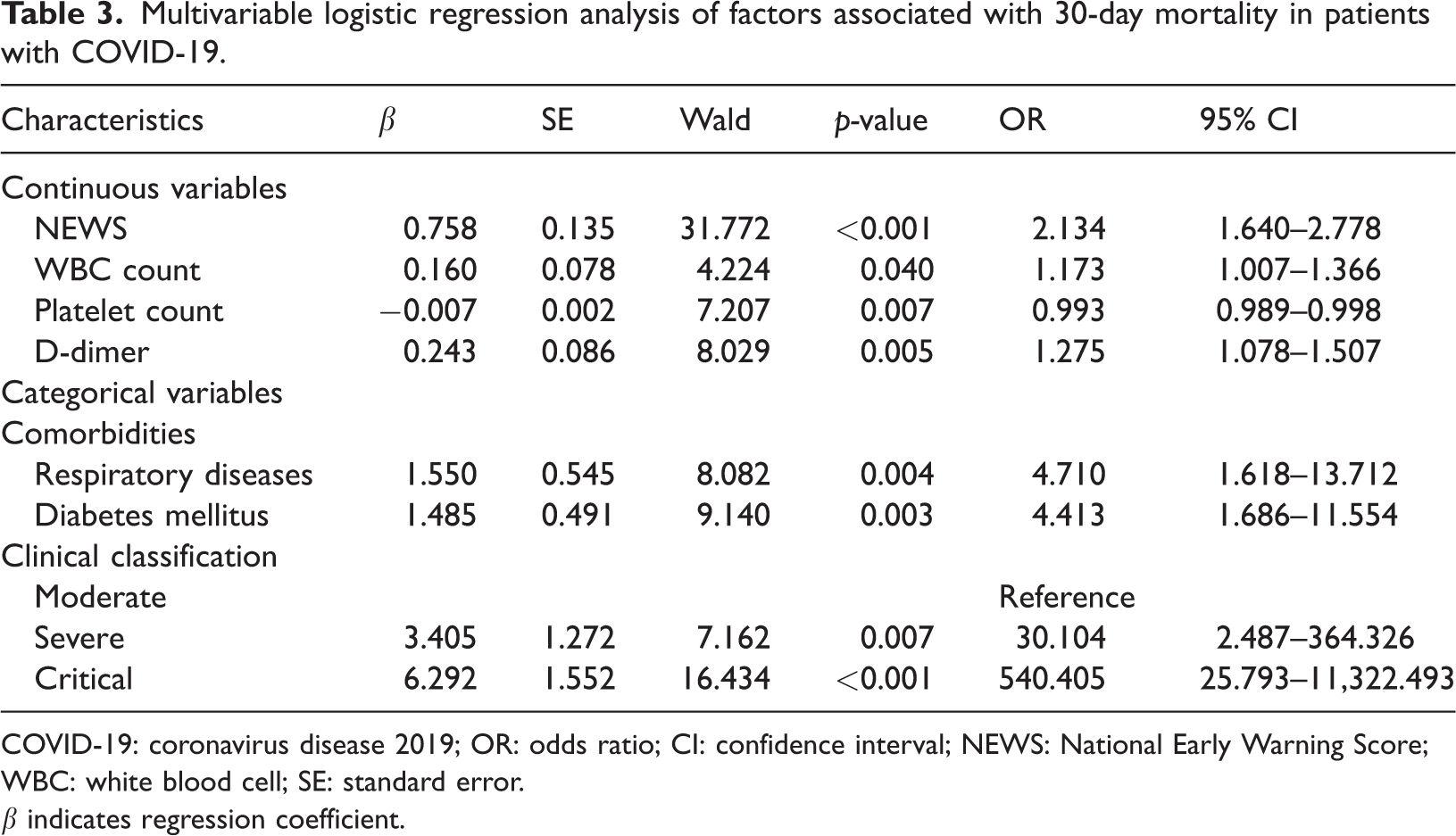
COVID-19: coronavirus disease 2019; OR: odds ratio; CI: confidence interval; NEWS: National Early Warning Score; WBC: white blood cell; SE: standard error.
β indicates regression coefficient.
For clinical interpretation, patients were categorized into high-risk (NEWS ≥ 6) and low-risk (NEWS < 6) groups based on an optimal NEWS cutoff of 5.5, derived from the ROC curve. Multicollinearity assessment confirmed that all VIF values were <5. After adjustment, the high-risk group had a 21.882-fold higher mortality risk than the low-risk group (adjusted OR = 21.882, 95% CI: 6.095–78.554, p < 0.001).
Comparison of chest CT findings between survivors and nonsurvivors with COVID-19
All pulmonary CT images were independently reviewed by two radiologists from our institution, each with more than three years of experience, according to the Fleischner Society guidelines. 8 The assessment focused on typical COVID-19 imaging features, including ground-glass opacities(GGO), linear/reticular opacities, interlobular septal thickening, alveolar consolidation, and the “crazy paving” patterns. 9 Overall lung involvement was calculated by summing the affected areas across the five lung lobes, and a threshold of 50% was used to categorize patients into high- and low-involvement groups. Forty-seven patients were unable to undergo CT because their oxygen saturation levels were <70% upon admission to the resuscitation room. Among these, 46 died and one survived. As shown in Table 4, compared with survivors, nonsurvivors had a shorter interval from symptom onset to admission, experienced more rapid disease progression, and a significantly higher proportion had lung involvement exceeding 50% (81.8% vs 9.4%, p < 0.001).
Comparison of chest CT findings between survivors and nonsurvivors with COVID-19.

CT: computed tomography; COVID-19: coronavirus disease 2019; IQR: interquartile range.
Discussion
Since late 2019, COVID-19 has spread globally. Epidemiological data indicate that its infection and mortality rates are significantly higher than those of severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS). 10 Although the World Health Organization (WHO) declared on 5 May 2023 that COVID-19 no longer constitutes a public health emergency of international concern, 11 it continues to pose a global health threat. Patients of advanced age and those with chronic comorbidities such as hypertension tend to have poor outcomes. 12 As China’s population continues to age, the number of such high-risk individuals remains substantial. Given the virus’s high transmissibility, rapid mutation rate, and potential to cause future outbreaks, the risk of large-scale critical illness persists. Conventional triage algorithms may fail to reliably identify high-risk geriatric patients. Therefore, prompt assessment of disease severity, identification of prognostic factors for deterioration, and timely implementation of interventions are crucial for improving clinical outcomes.
NEWS and MEWS have demonstrated significant clinical value in early disease detection, severity assessment, and prognosis prediction. 13 However, MEWS and qSOFA have shown limited sensitivity in predicting outcomes for potentially critically ill patients. 14 NEWS incorporates two additional parameters, oxygen therapy administration and blood oxygen saturation, which enhance the NEWS framework and emphasize the importance of respiratory monitoring. NEWS has shown greater specificity than MEWS in older critically ill patients and accurately predicts admissions to the intensive care unit (ICU) and in-hospital mortality. 15 COVID-19 patients with critical illness exhibited more severe respiratory impairment, and hypoxemia was a predictor of critical illness and mortality. 16 Consequently, NEWS outperformed MEWS and qSOFA in early warning and mortality risk identification. NEWS integrates vital signs such as respiratory function, blood pressure, and heart rate, all of which have been associated with COVID-19 prognosis. 17 Therefore, this study aimed to evaluate the prognostic value of NEWS in patients with COVID-19. At a cutoff value of 5.5, NEWS predicted mortality with a sensitivity of 97.8% and a specificity of 74.0%. The AUROC of NEWS was significantly higher than those of MEWS and qSOFA, demonstrating its superior discriminative ability for predicting COVID-19–related mortality. Multivariate logistic regression analysis confirmed that NEWS was an independent predictor for poor prognosis in patients with COVID-19, with higher scores associated with increased mortality risk, suggesting its utility in assessing disease severity. These findings are consistent with those reported by Endo et al. 18 Considering that patients with COVID-19 are at risk of rapid progression to acute respiratory failure or shock 19 and that all patients in our cohort were critically ill with pronounced abnormalities in respiratory rate, hemodynamics, and mental status, the overlapping parameters between qSOFA and MEWS may explain their comparable performance and the lack of a statistically significant difference. Our study highlights the critical importance of the early NEWS implementation in emergency triage for COVID-19. A novel aspect of our study is that NEWS was associated with the ability to identify potential high-risk patients, possibly facilitating targeted interventions and optimized resource allocation.
In this study, the mortality rate among patients with COVID-19 treated in the resuscitation room was 41.4%, significantly higher than those observed in hospitalized patients (13%) and those in the ICU (37%). 20 Several factors may account for this discrepancy. First, during the pandemic control phase, most individuals lacked natural immunity to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Following the adjustment of control policies, older adults, particularly those with comorbidities and without COVID-19 vaccination, exhibited relatively weaker immune defenses. Second, all patients diagnosed with COVID-19 in the resuscitation room were classified as having at least moderate disease severity. These patients exhibited significantly impaired respiratory function, frequently progressing to respiratory failure or even multiple organ dysfunction. Some patients deteriorated too rapidly to be hospitalized in time, contributing to the high mortality rate. Previous studies have confirmed that comorbidities such as chronic kidney disease, chronic obstructive pulmonary disease, cerebrovascular disease, coronary heart disease, and diabetes are closely associated with COVID-19 severity and prognosis.21,22 Consistent with these findings, our study identified preexisting respiratory disease and diabetes as independent risk factors for COVID-19 mortality. Our results suggest the importance of early NEWS assessment in patients with such comorbidities, and it may facilitate the early detection of critical illness.
Our analysis revealed significant differences in most laboratory parameters between survivors and nonsurvivors. Easily accessible biomarkers provided early insights into disease severity. For example, markedly elevated CRP levels may trigger a cytokine storm. 23 Decreased LYM counts and an elevated NLR were significantly associated with severe disease and mortality. 24 Previous studies have identified LYM counts and CRP and D-dimer levels as prognostic factors for COVID-19,25,26 and our results further confirm that WBC and PLT counts and D-dimer levels are independent predictors. Specifically, higher WBC counts and D-dimer levels and lower PLT counts were associated with an increased mortality risk. Therefore, integrating these laboratory indicators into clinical practice may facilitate early identification of critically ill patients and enhance outcomes. Chest imaging also plays a vital role in COVID-19 diagnosis and management. Performing thoracic imaging enables confirmation or exclusion of pulmonary involvement. 27 Pulmonary consolidation on CT has been identified as an independent risk factor for COVID-19–related mortality, 28 and nonsurvivors commonly exhibit extensive lung involvement, including bilateral, diffuse, and multilobar lesions. 9 Consistent with these reports, our study found a significantly higher proportion of nonsurvivors with CT involvement exceeding 50%. These findings suggest the utility of chest CT for early detection in critically ill patients. Furthermore, classifying CT manifestations into patterns, such as negative, bronchopneumonia, organizing pneumonia, and diffuse alveolar damage, may contribute to early prognostic stratification. 29
The generalizability of our findings to similar inpatient settings in comparable healthcare systems is supported by three key factors: the recruitment of patients from tertiary hospitals, the inclusion of broad clinical spectrum of COVID-19 severity, and the use of the internationally standardized NEWS. Nevertheless, this study has several limitations. First, its single-center, retrospective design introduces potential selection and information biases, including inconsistencies in medical documentation. Additionally, the resulting limited sample size may have reduced the statistical power and restricted the robustness of subgroup analyses. Second, missing CT data for a subset of patients may have compromised the comprehensiveness of radiological assessments. Collectively, these limitations constrain the broader applicability of our conclusions and underscore the necessity to validate our results in future large-scale, multicenter prospective cohort studies.
Conclusion
Our results suggest that the application of a simple and effective scoring system in clinical practice is valuable. Early implementation of NEWS may help identify patients with COVID-19 who are at risk of critical progression, thereby facilitating timely and targeted interventions and improving prognosis.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Han Xue for her valuable assistance and guidance in the preparation of this manuscript.
Author contributions
Zhang X.Y.: Conceptualization; methodology; writing of the original draft, review, and editing of the manuscript.
Li F.J.: Supervision as well as review and editing of the manuscript.
All authors have read and approved the final manuscript.
Data availability statement
The clinical data used in this study contain sensitive patient information and are protected under the GDPR and institutional ethical approvals. Anonymized data may be made available to qualified researchers who enter into a data use agreement with the corresponding institution.
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.