
Abstract
Background:
Modified early warning score has been validated in many uses in the emergency department. We propose that the modified early warning score performs well in predicting the need of lifesaving interventions in the emergency department, as a predictor of patients who are critically ill.
Objective:
The study aims to evaluate the use of modified early warning score in sorting out critically ill patients in the emergency department.
Methods:
The patients’ demographic data and first vital signs (blood pressure, heart rate, temperature, respiratory rate, and level of consciousness) were collected prospectively. Individual modified early warning score was calculated. The outcome was a patient received one or more lifesaving interventions toward the end of stay in emergency department. Multivariate logistic regression analysis was utilized to assess the association between modified early warning score and other potential predictors with outcome.
Results:
There are a total of 259 patients enrolled into the study. The optimal modified early warning score in predicting lifesaving intervention was ≥4 with a sensitivity of 95% and specificity of 81%. Modified early warning score ≥4 (odds ratio = 96.97, 95% confidence interval = 11.82–795.23, p < 0.001) was found to significantly increase the risk of receiving lifesaving intervention in the emergency department.
Conclusion:
Modified early warning score is found to be a good predictor for patients in need of lifesaving intervention in the emergency department.
Introduction
Background
The reliability of identifying critically ill patients has an utmost importance in the emergency department, including pre-hospital service, triage and in-hospital management. Over years, the ability to triage these ill patients as early as pre-hospital care or at triage has always been an area of research interest.
A triage system in the form of standardized scale has been considered ideal for emergency departments.1,2 So far, there are four standardized, validated triage scales that have been used worldwide, including the Manchester Triage, the Canadian Triage Assessment Scale (CTAS), the Australian Triage Score (ATS), and the Emergency Severity Index (ESI). However, these triage scales required extensive training, and it is time consuming in triage each patient. In order to build up a simple system where only little training is required, Burch et al. 3 have brought up the idea of adding a physiological scoring system (modified early warning score (MEWS)) to facilitate the triage process.
MEWS was first validated in identifying critically ill patients in the medical ward, surgical ward, and intensive care unit.3–7 The scoring system is also found to have high sensitivity of pre-hospital detection of critical illness. 8 It correlates the severity of the patient’s illness to changes of their physiological parameters. The parameters outlined by MEWS are illustrated in Table 1.
Modified early warning score (MEWS).
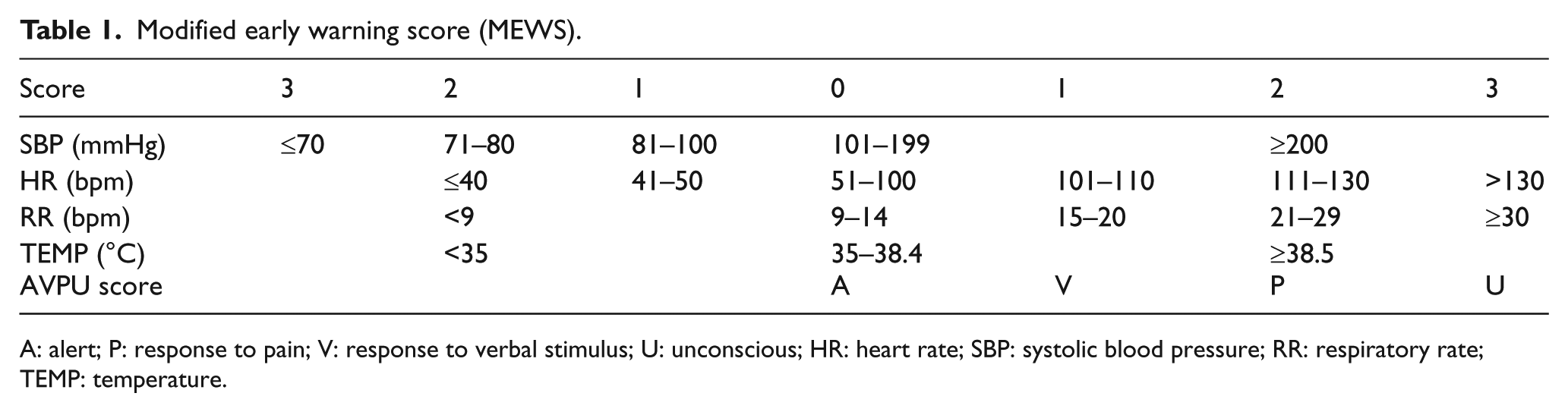
A: alert; P: response to pain; V: response to verbal stimulus; U: unconscious; HR: heart rate; SBP: systolic blood pressure; RR: respiratory rate; TEMP: temperature.
In the emergency department, MEWS has been validated to predict hospital admission, 9 observation ward admission, 10 in-hospital deaths, 11 and requirement of higher level of care. 12 However, the scoring system is not recommended for trauma patients due to underscoring 13 and finding that it did not statistically reduce mortality in trauma patients. 14 Currently, MEWS has been modified and used in the triage system in hospitals in Western Cape, South Africa. 15 The effect of MEWS in triage has been found to reduce waiting time 16 and improve overtriage and undertriage rates. 17
Objectives
The purpose of this study is to evaluate whether the MEWS performs well in predicting the need of lifesaving interventions in the emergency department, as a predictor of patients who are critically ill. If MEWS is proven to have good predictive strength to identify critically ill patients, it may incorporate as an adjunct to our triage system in the future.
Methodology
Study design
The study was designed as a cross-sectional observational study.
Venue
The study was conducted in Emergency Department, Hospital Tuanku Ja’afar, a level IV state hospital in Negeri Sembilan, Malaysia. The department has an annual visit of about 135,000 patients per year. According to department census in year 2013, approximately 6% of cases were triaged red (critical), whereas 32% and 62% were triaged yellow (semi critical) and green (non-critical), respectively.
Sample population
Adult non-trauma patients (age 18 years old or more) who presented to the emergency department during the study period were recruited into the study using convenience sampling method. Non trauma patients were defined by patients who were triaged using department non-trauma clerking sheet. Exclusion criteria involved patients who were referred from other centers or pregnant patients because of their deranged physiological parameters at presentation. Patients who had incomplete documentation of the physiological parameters, brought in death (BID), refused for lifesaving intervention, discharged home against medical advice, and absconded from the hospital were also excluded from the study due to inability to assess the study outcome.
Study protocol
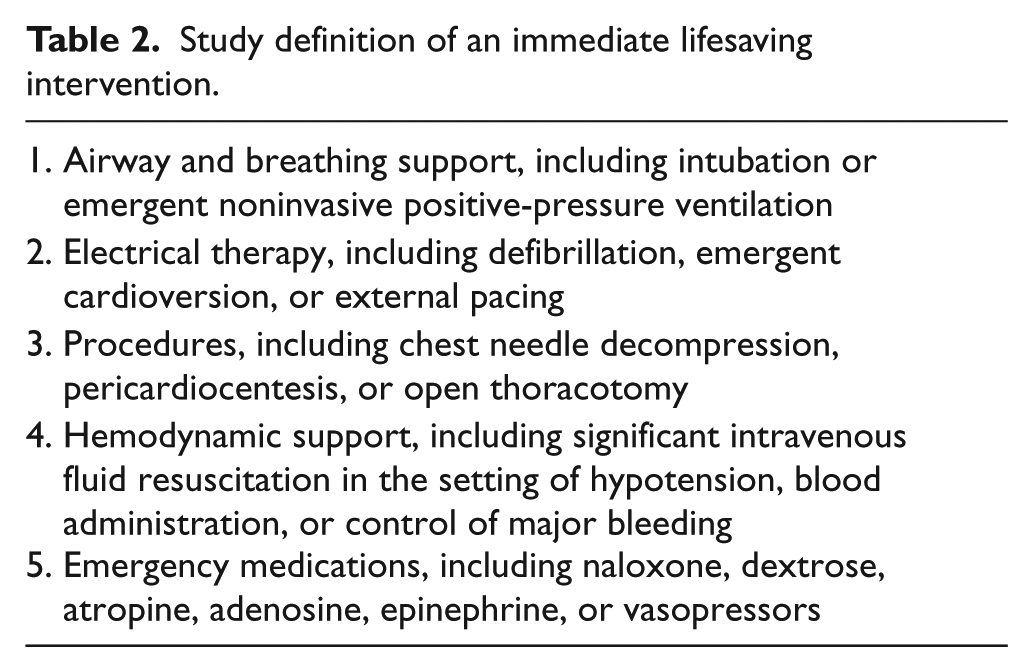
Within the study period, adult patients who visited the emergency department and met the inclusion criteria were enrolled in this study using convenience sampling method. A data collection sheet was enclosed for all the eligible samples. The MEWS was calculated for each patient using patient’s blood pressure (mmHg), heart rate (beats per minute), temperature (°C), respiratory rate (breaths per minute), and level of consciousness (AVPU scale) documented in the patient’s case note. Only the first parameters taken in the emergency department were collected for data analysis. The patient’s demographic data were also collected. Toward the end of emergency department stay (prior to discharge, admission, or death), the patient’s case note was studied to see whether the patient has received any lifesaving intervention (defined as patient received one or more lifesaving interventions). Definition of an immediate intervention was illustrated in Table 2.18,19 All the data sheets were collected prior to patient’s discharge from the emergency department.
Study definition of an immediate lifesaving intervention.
Study outcomes
The primary outcome of this study was patient who received one or more immediate lifesaving interventions according to Table 2.
Statistical methods
Data analysis was conducted using IBM SPSS statistics for Windows, version 21.0 (IBM Corporation, Armonk, NY). Descriptive analysis was carried out for patient’s demographic data using either mean ± SD (standard deviation) or median ± interquartile range (IQR) when appropriate for continuous variables and frequency + percentage for categorical variables. Univariate analysis was used to assess the difference between outcome groups using independent t-test for normally distributed continuous variables, Mann–Whitney test for non-normally distributed continuous variables, and chi-square test or Fisher’s exact test for categorical variables. A receiver operating characteristic (ROC) curve was utilized to determine the optimum cutoff points for MEWS. Finally, the optimum MEWS and other potential predictors are analyzed using multivariate logistic regression to assess the association with outcome. A difference with a p value of less than 0.05 was considered to be statistically significant.
Results
Patients’ demographic data and clinical characteristic
There were a total of 259 patients enrolled into the study and included in the analysis. Among them, 141 (54%) were male and 118 (46%) were female. The mean age was 47 years old (SD = 18.38). A total of 48 (19%) patients were triaged red, 68 (26%) and 143 (55%) were triaged yellow and green, respectively. Among these patients, 69 patients had diabetes mellitus, 93 had hypertension, and 16 had chronic kidney disease. The patients’ MEWSs were not normally distributed (Figure 1). It ranged from 0 to a maximum score of 9 with a median score of 2 (IQR = 3). Most of the patients scored 1 (n = 77) or 2 (n = 67). There were 22 patients (8%) who eventually received one or more lifesaving intervention during their stay in the emergency department.
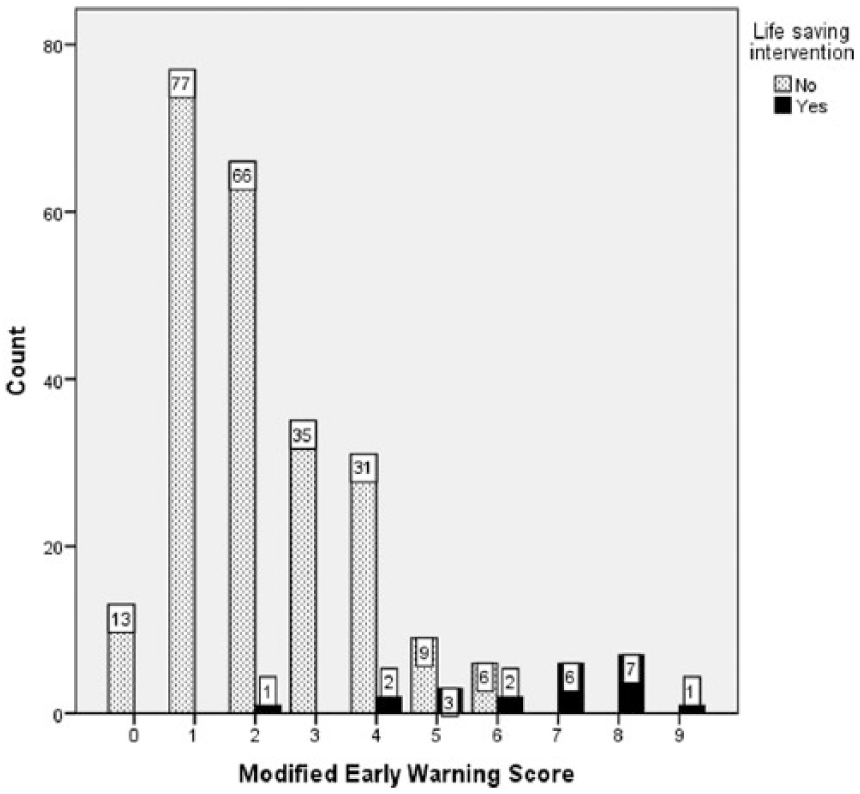
Modified early warning score.
Comparison between outcomes groups
The patients receiving lifesaving intervention had a slightly higher age (mean = 57 years) than the patients not receiving any lifesaving intervention (mean = 47 years; Table 3). There was no significant difference in patient’s gender between the two groups. In the group patients received lifesaving intervention, majority (n = 21, 96%) were triaged red initially compared to the other group whose majority were triaged green initially (n = 143, 60%). The lifesaving intervention receiving group also had a higher rate of having diabetes mellitus (n = 10, 46%), hypertension (n = 13, 59%), and chronic kidney disease (n = 6, 27%). The patients who received lifesaving intervention had a higher MEWS (MEWS ≥4; n = 21, 96%) compared to the other group, which overall had a lower score (MEWS <4; n = 191, 80%).
Demographic characteristic and MEWS between outcome groups.
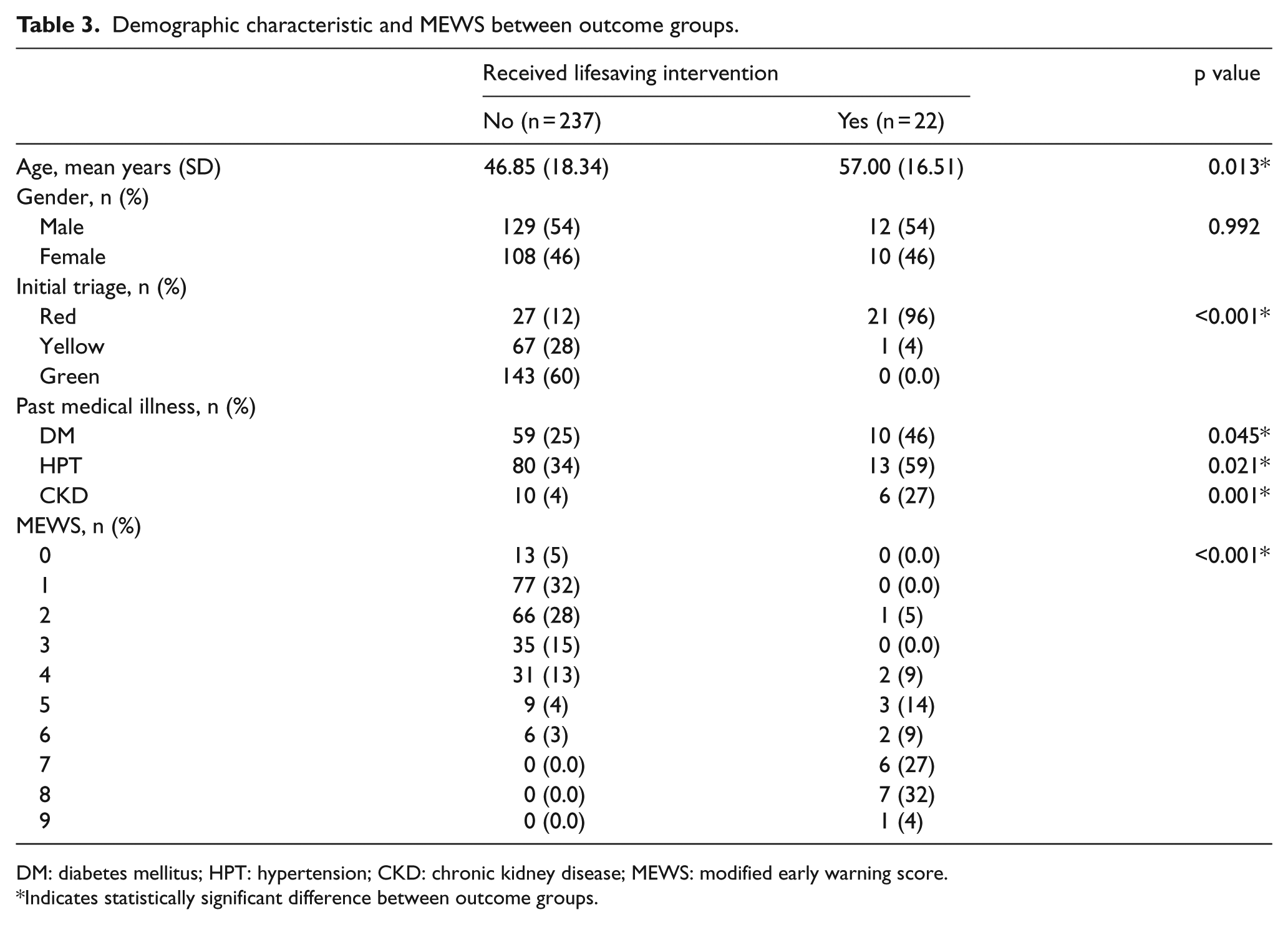
DM: diabetes mellitus; HPT: hypertension; CKD: chronic kidney disease; MEWS: modified early warning score.
Indicates statistically significant difference between outcome groups.
Optimum cutoff points for MEWS
A ROC curve was constructed for MEWS (Figure 2). The area under the curve (AUC) was 0.959 (95% confidence interval (CI): 0.91–1.00, p < 0.001). MEWS ≥4 was found most optimal in predicting lifesaving intervention in the emergency department with a sensitivity of 95% and specificity of 81%.
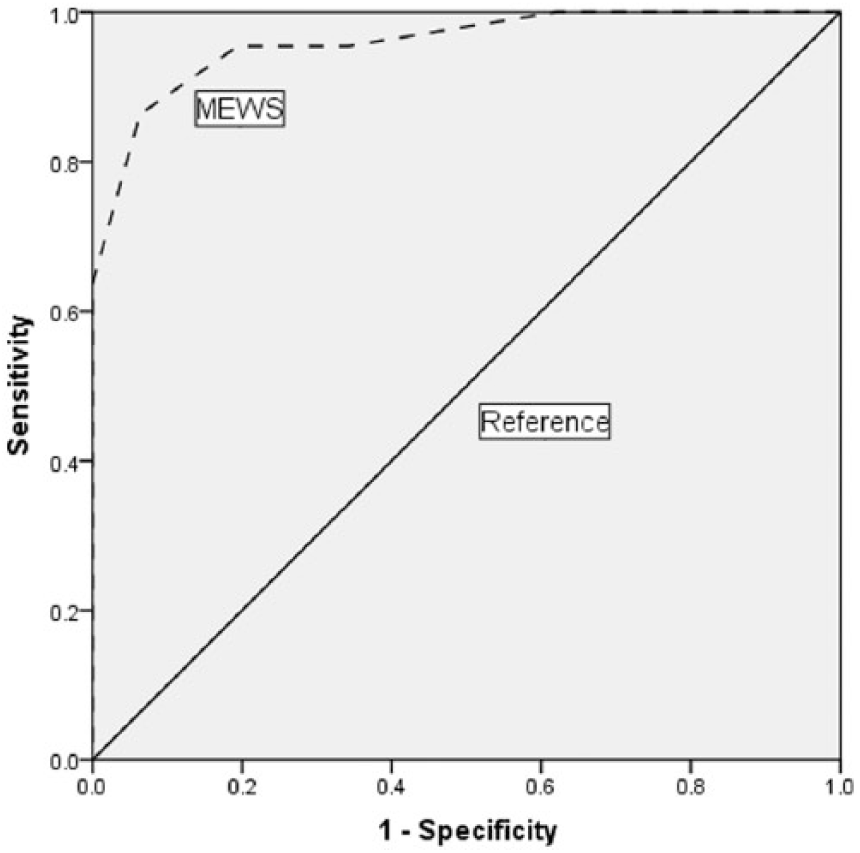
Receiver operating characteristic (ROC) curve for MEWS in predicting need of lifesaving intervention.
Association between MEWS and outcome
MEWS ≥4 and other potential predictors (age ≥65, medical history of diabetes mellitus, hypertension, and chronic kidney disease) were put into a multivariate logistic regression analysis to identify the confounding factors and the association between predictors and outcome (Table 4). MEWS ≥4 was found to significantly increase the risk of receiving lifesaving intervention in the emergency department (odds ratio = 96.97, 95% CI: 11.82–795.23, p < 0.001). Patient’s medical history of chronic kidney disease (odds ratio = 10.85, 95% CI: 1.55–75.79, p = 0.016) was also found to increase risk of outcome. Patient’s age ≥65 (odds ratio = 0.77, 95% CI: 0.20–2.93, p = 0.697), medical history of diabetes mellitus (odds ratio = 0.76, 95% CI: 0.20–2.90, p = 0.684), and hypertension (odds ratio = 1.73, 95% CI: 0.45–6.70, p = 0.426) were not significant in predicting the outcome.
Logistic regression analysis of predictors associated with outcome.
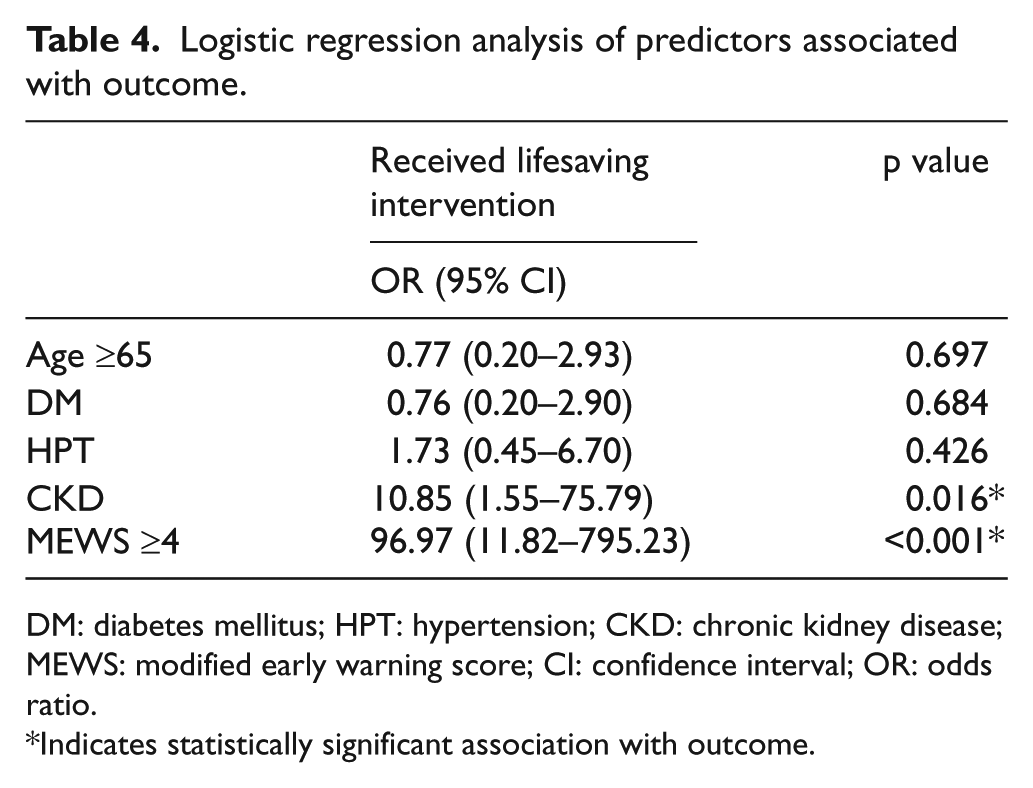
DM: diabetes mellitus; HPT: hypertension; CKD: chronic kidney disease; MEWS: modified early warning score; CI: confidence interval; OR: odds ratio.
Indicates statistically significant association with outcome.
Discussion
In addition to previous studies that prove MEWS use in predicting hospital admission, 9 observation ward admission, 10 and in-hospital deaths, 11 our study has proven another beneficial use of MEWS in identifying ill patient in the emergency department. Our study outcome was designed in predicting patient requiring lifesaving intervention in the emergency department. Compared to previous studies, we wish to study the ability of MEWS to sort out these ill patients as early as the patient arrives at the triage counter. A higher MEWS means the patient is more likely to receive resuscitation; thus, they should be promptly assigned to the highest level of care in the department. In comparison to that, previous studies’ outcomes may not reflect patients with a higher MEWS should be triaged to resuscitation zone immediately, but rather show that these patients require more resource utilization and close monitoring in the department. The ability to recognize acutely ill patient using MEWS in this study is very valuable for our triage system and pre-hospital care in our emergency care system.
In comparing the characteristic between outcome groups, the patients who received lifesaving intervention have found to be older. The initial triage was appropriate. Those who required lifesaving intervention has also significant higher rate of underlying premorbid diseases (diabetes mellitus, hypertension, and chronic kidney disease). However, our study reveals that although there are differences in the outcome groups, except for the history of chronic kidney disease, these factors are not found significant in predicting the outcome. In other words, identifying patients with underlying diabetes mellitus and hypertension does not help in predicting the need of lifesaving intervention in the department, nor does an older patient will have a higher rate of being resuscitated.
This finding is contradictory to our usual assumption that older age group and patients with comorbidities have a higher risk of getting lifesaving intervention in the emergency department. They are usually given a higher level of triage initially in the department. To our surprise, our result shows that the patient’s age, comorbidity of diabetes, and hypertension are not significant to predict them to be required in the resuscitation zone. In contrast to that, MEWS scoring system appears to be a good predictor to the outcome compared to other factors. This finding proves that MEWS can be utilized in the emergency department for identifying ill patients. The possible explanations for these findings are that the patient with underlying diabetes and hypertension may not actually contribute to the current presenting illness. The presenting illness will alter the patient’s current physiological state, eventually reflected by measuring the MEWS.
Our study shows that MEWS ≥4 found to be most optimal in identifying patients who required lifesaving intervention in the department (sensitivity: 95%, specificity: 81%). This finding corresponds well to Gardner-Thorpe et al., 6 which has a sensitivity of 75% and specificity of 83% (MEWS threshold score of ≥4) in identifying critical care unit admission for surgical patients. The finding also corresponds well with other studies on MEWS such as in predicting admission 9 and in-hospital deaths. 11 In comparison to other studies, our result has a higher sensitivity, as we are predicting patients who are receiving resuscitation; thus, the acute physiological changes are more easily identified by the scoring system.
Limitations
Our limitation in this study includes a relatively small sample size. This was because our emergency department, which is a tertiary center, receives most of the patients from other hospitals (patients who are referred from other centers were excluded from the study). Besides, the study only enrolled adult non-trauma patients. Patients less than 18 years old and trauma cases which had a significant number of visits to the department were not included in the study.
Another limitation is that the study was conducted in a single center. This had limited the results to a tertiary center and the data may not able to be generalized to other settings, such as in smaller district hospital.
A MEWS of 4 and above should be assigned in the front-lined triage system to sort out the patient who required resuscitation, and a further study is required to validate the use. However, looking at the high sensitivity of the MEWS in our study, a patient with a score of 4 and above should be given a close monitoring and assigned to a higher triage in the emergency department. We also suggest all patients should have a baseline MEWS. Any increase in the score by ongoing monitoring will be very helpful in identifying deteriorating patients in the department. Further references to the score can also be made when the patient has been admitted to the ward.
MEWS is a simple scoring system which is easy to use, objective, and reliable. To our knowledge, this is the first study for MEWS in Malaysia emergency department setting. Due to its simplicity and reproducibility, the study of MEWS as a triage tool in small busy district hospitals is valuable. We suggest future studies to include smaller district hospitals in a multicenter study setting. The use of MEWS in the triage system, ongoing monitoring of patients in the department, pre-hospital care, and referral system should be further evaluated in future studies. We also suggest that modification to the current MEWS in order to increase its ability to detect critical patients in trauma emergencies and younger pediatric patients.
Conclusion
The study has proven the usefulness of MEWS in identifying critically ill patients who required lifesaving intervention in the emergency department. We look forward for future studies to validate its further use in the emergency department.
Footnotes
Acknowledgements
The authors would like to thank the Director of Health Malaysia for permission to publish this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Medical Review and Ethics Committee (MREC), Ministry of Health Malaysia with waiver of informed consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.