
Abstract
Introduction
Outdoor activities offer physical and mental health benefits. However, incidents can occur requiring ambulance transport to hospital. This study aimed to describe the epidemiology and severity of traumatic and medical incidents for mountain bikers and hikers transported by ambulance within Western Australia.
Methods
This was a retrospective cohort study of ambulance-transported mountain bikers and hikers within Western Australia from 2015 to 2020. Data were extracted from ambulance electronic patient care records. Multivariable analyses were undertaken to identify variables associated with higher patient severity based on the National Early Warning Score 2 (NEWS2).
Results
A total of 610 patients required ambulance transport to hospital while mountain biking (n=329; 54%) or hiking (n = 281; 46%). Median age of mountain bikers and hikers was 38 (24–48) y and 49 (32–63) y, respectively. Paramedics reported a fracture in 92 (28%) mountain bikers and 78 (28%) hikers. The predominant injury locations for mountain bikers were upper limbs and for hikers, lower limbs. Cases were trauma related in 92% of mountain bikers and 55% of hikers. A significant association (P<0.001) between the etiology of the ambulance callout and patient severity was found. In trauma etiology cases, the frequency of medium-risk+ NEWS2 severity was 21.4%. In medical cases, the frequency of medium-risk+ severity was 40.8%.
Conclusion
Both mountain bikers and hikers experienced incidents requiring ambulance transport to hospital. Incidents of a medical etiology had a higher clinical risk, as determined by the NEWS2 scores, regardless of activity being undertaken.
Introduction
Around the world and within Western Australia (WA), mountain biking is a popular recreational and sporting activity, with an estimated 468,000 participants in Australia undertaking mountain biking at least once in 2021.1,2 Previous work has attempted to document injuries sustained by mountain bikers in a competitive race environment who were attended by first aid staff3-5 and in emergency department presentations6-9 but has not investigated ambulance attendances. Mountain biking injuries are commonly reported as being minor, and most injuries are often abrasions, contusions, and lacerations in both recreational and competitive settings.4,10,11 Lower limb fractures are often the second most common injury presentation when all injuries are reported.6,12 Where only more severe injuries are reported, such as involving admission to an orthopedic ward or trauma registry, fractures are common, the majority being reported as upper limb fractures, lower limb fractures, or spinal injuries.6,13 Hiking injuries are also commonly reported to be minor but are dominated by lower limb injuries such as blisters and soft tissue complaints such as ankle sprains.14-16
Studies have examined the rescue of hikers from alpine regions, but little work has been undertaken on subalpine trail users at lower altitudes.14,17-19 One study attempted to categorize all incidents occurring within protected area boundaries within WA. 20 This study included only incidents reported to park personnel and, as such, did not include all ambulance-transported cases. No previous work has used ambulance records to describe mountain bikers’ and hikers’ medical events and injuries. Additionally, no previous comparison of injury patterns between mountain bikers and other trail users was found.
Mountain biking within WA is undertaken on trails that are centered around trail hubs, which are areas where multiple trails are in close proximity. There are 6 main trail hubs within WA in addition to a 1000 km long-distance mountain biking trail. Hiking within WA is spread across multiple trails with at least 365 recognized walking and hiking trails within the state. Hiking trail surfaces are similar to the surfaces on many mountain biking trails and often within the same areas. 21
Aim
This study describes and compares the epidemiology and severity of medical conditions and traumatic injuries of mountain biking and hiking patients transported to hospital by ambulance. The primary aim of this study was to characterize the injury locations and medical events of ambulance-transported mountain bikers and hikers using prehospital data. A secondary aim was to determine whether mountain bikers transported by ambulance had a higher severity level of presentation than hikers.
Methods
This study was approved by the Curtin University Human Research Ethics Committee; additionally, the use of St John Western Australia (SJWA) data was approved by the SJWA research governance committee.
All mountain biking and hiking trails available from the Trails WA website were downloaded.21,22 These trails were then buffered by 50 m to ensure that any cases logged with inaccurate Global Positioning System coordinates were captured, and any cases falling within these buffers were then added to the dataset. Finally, a manual review of the electronic patient care record (ePCR) examination text was undertaken in Microsoft Excel v2206 (Microsoft Corp, Redmond, WA). For each record identified by these search methods, a manual review ensured that each included case was related to either mountain biking or hiking and involved trails. Competitive and recreational activities were included.
Participants
This study was a descriptive retrospective cohort study of mountain bikers and hikers transported by ambulance to hospital. For mountain biking, all types of off-road trail cycling were examined, including downhill and cross-country cycling. Hiking was considered to include any activity on an off-road trail that was self-powered (without a vehicle). This included bushwalking, orienteering, and trail running.
Exclusion Criteria
Cases were excluded if the mountain biking or hiking was not undertaken on a trail (eg, incidents on a paved cycle path or road). Patients who called an ambulance on returning home also were excluded from the dataset. For any cases where two ambulances were sent, only the primary treating crew was included. Similarly, cases were excluded where an ambulance was called but did not treat or transport the patient. Cases in metropolitan Perth were excluded because walking trails within this region are within parks or other urban settings.
Study Setting
Mountain biking trails within WA are predominantly narrow single tracks on loose gravel and dirt with low overall elevation. Typically, the trails are either downhill or cross country and at a maximum elevation of 350 m. Downhill trails were between 500 m and 2 km in length with an elevation loss between 50 and 150 m. Trails were a mixture of difficulty, with easy, intermediate, and advanced levels. 15 Hiking trails were of similar topography and in similar locations to those described for mountain biking trails.
Within WA, the state ambulance service is run by SJWA, which is the only organization contracted to provide emergency ambulance cover across all areas of WA. Ambulances are staffed by a mixture of registered paramedics, ambulance officers, and, in some rural locations, ambulance volunteers. The Medical Priority Dispatch System 23 is used to triage ambulance dispatch. In this study, participants included all patients transported to hospital by ambulance for incidents experienced while mountain biking or hiking within WA between January 1, 2015 and December 31, 2020. Cases were identified using the SJWA ePCR completed by the attending paramedic/ambulance officer at the time of the incident. The ePCRs include patient vital signs, medical conditions treated, medications administered, any identified injuries, and injury locations. Both medical and trauma-related events were included if they prevented the patient from continuing the activity by requiring them to be transported to hospital. In all cases, the etiology of the condition was defined by the treating officer at the time of treatment and could include medical or traumatic etiologies. Only one etiology can be recorded in the ePCR, and this is recorded as the main presenting complaint.
Variables
The following data were extracted from the ePCRs: date, age, sex, activity being undertaken (mountain biking or hiking), prehospital contact interval (time from ambulance dispatch to arrival at a hospital), dispatch priority, transport method (air or road), paramedic-reported injuries, etiology of each case, and patient vital signs. Dispatch priority is classified as priority 1 to 3, with priority 1 being the highest with lights and siren. Etiology was dichotomized into trauma related or medical etiology using the problem code recorded by the ambulance officer/paramedic in the ePCR. For estimating patient severity, National Early Warning System 2 (NEWS2) scores were calculated. Patients’ physiologic characteristics were given a numerical score following the guidelines of the Royal College of Physicians, and those scores were aggregated to gain an overall NEWS2 score. 24
The NEWS2 score was then characterized by risk level from low to high using the Royal College of Physicians NEWS2 score thresholds and triggers. 24 This classifies a score of 0 to 4 as low, 5 to 6 as medium, and 7 or more as high. 24 Additionally, any patient who had a vital sign that returned a value of 3 in any parameter was classified as low to medium risk. 24 We further classified patients into either low risk or above low risk. Under NEWS2 guidelines, any classification above low risk requires the patient to be reviewed by a medical team, whereas any low-risk score does not. 24 While NEWS2 scores are traditionally used in hospitals to identify patient deterioration, they have been shown in the prehospital environment to correlate strongly with in-hospital mortality and hospital admission to intensive care units and to identify high-risk patients.25-29 Prehospital NEWS2 scores found good predictive capability of 3 d mortality but less so for mortality at 30 days. 30 This suggests that NEWS2 scores are suitable for indicating acute clinical severity in the short term. To meet our secondary aim of whether mountain bikers have a higher severity of presentation than hikers, we compared activity undertaken, age, sex, dispatch priority, prehospital interval, etiology, and ambulance officer/paramedic-reported suspected fracture or dislocation between low- and high-risk NEWS2 scores.
For injuries, the data were extracted from ePCRs, where bodily injury location and type of injury were selected from a dropdown list. For an injury to be included, it must have been recorded by the on-scene paramedic or ambulance officer. A single patient may have had multiple injuries recorded. The final list of bodily injury locations was summarized into 5 separate aggregated locations: head, spine, torso, upper limbs, and lower limbs. The head included skull, face, eyes, ears, and nose. The spine included cervical, thoracic, and lumbar spine. Torso included chest, back, abdomen, and groin. Upper limbs included the shoulder girdle, arms, wrists, and hands. Lower limbs included legs, knees, ankles, and feet. Interventions performed were extracted from the ePCR and included medications administered, intravenous cannulation, and whether cardiopulmonary resuscitation was performed. Medications were recorded as total dose administered in addition to how many patients received each medication because single patients may have received multiple doses of the same drug.
Data Analysis
Data were analyzed using Stata 17.0, (StataCorp LLC, College Station, TX). Data were described with medians and interquartile ranges or with counts and percentages using Mann-Whitney U or χ2 tests as appropriate. Where small data numbers could potentially lead to the identification of individual patients, this was reported as <5 rather than the actual number to comply with our Human Research Ethics Committee approval requirements. We compared patients who had low clinical severity (as defined by NEWS2 criteria) with patients who had above low clinical severity. We tested for differences in age, sex, dispatch priority, categorized prehospital patient care interval, activity undertaken (biking or hiking), recorded etiology of the presenting complaint, and paramedic/ambulance officer–reported suspected fracture or dislocation. Age was treated as a continuous variable; categorized prehospital patient care interval and dispatch priority were treated as categorical variables; and sex, activity undertaken, etiology, and reported presence of fracture or dislocation were treated as binary variables. Most NEWS2 calculation variables are required to be completed by paramedics, but some variables, such as temperature, are optional. Where these values were not recorded, they were treated as a zero score in the NEWS2 score calculation.
A multivariable logistic regression model was derived to identify factors associated with patient severity. We used the dichotomized NEWS2 score as a dependent variable and age, sex, dispatch priority, prehospital patient care interval, activity undertaken, etiology of the presenting complaint, and paramedic/ambulance officer–reported suspected fracture or dislocation as independent variables. Where an interaction was deemed clinically plausible between 2 independent variables, then that interaction also was included in the multivariable analysis; this included patient age and activity being undertaken. Backward elimination was then used to optimize the model, where a likelihood ratio test confirmed at each step that the new model was not significantly worse than the previous model. Elimination ceased when all remaining independent variables were significantly associated with the primary outcome. After optimization, the model was assessed for goodness of fit with a Hosmer-Lemeshow test. Statistical significance was declared in all cases at P < 0.05.
Results
A total of 610 patients met the inclusion criteria and required ambulance transport while mountain biking (n=329; 54%) or hiking (n=281; 46%) on a trail. Median age of all trail users was 43 (27–55) y, with the median age of mountain bikers being significantly younger at 38 (24–48) y than hikers at 49 (32–63) y (z=6.535; P<0.001). Overall, 339 patients (56%) were male, and 271 (44%) were female. Most mountain bikers were male (n=274; 83%), whereas more hikers were female (n=166; 59%). The median prehospital contact interval for all cases was 98 (66–138) min, with mountain bikers having a significantly (z=6.325; P<0.0001) lower prehospital interval at 90 (63–117) min than hikers at 111 (77–177) min. The attending paramedic/ambulance officer reported the presence of a suspected fracture or dislocation in 170 (28%) cases, with 92 (28%) mountain bikers and 78 (28%) hikers having at least 1 suspected fracture or dislocation. Considering the etiology of the condition, 304 (92%) mountain bikers and 154 (55%) hikers were transported by ambulance for trauma-related causes. Of the patients who had a medical etiology (n=157), most were from environmental (mountain bikers, n=4; hikers, n=40), neurologic (mountain bikers, n=6; hikers, n=36), and cardiac causes (mountain bikers, n=7; hikers, n=14). The remaining medical etiologies included respiratory problems (n=20), allergies (n=7), abdominal pain (n=6), and unspecified illnesses (n=12). Of all trail users requiring transport to hospital by ambulance, 213 (35%) were dispatched under priority 1 conditions; 292 (48%), priority 2; and 105 (17%), priority 3. A total of 26 (8%) mountain bikers and 19 (7%) hikers were transported by air ambulance, with the remainder transported via road ambulance. The median prehospital interval for air ambulance cases was 134 (98–152) min and for road ambulance cases was 95 (65–152) min. The length of prehospital interval was significantly greater for air ambulance than for road ambulance cases (P<0.001).
The number of cases where the first observed vital signs were found to be out of the normal range, as defined by the NEWS2 classification, are presented in Table 1. The bodily locations of injuries recorded by on-scene ambulance officers/paramedics are summarized in Table 2. Mountain bikers predominantly sustained injuries to the upper limbs (38%), whereas hikers predominantly sustained injuries to the lower limbs (54%). Mountain bikers had a higher proportion of spinal injuries recorded (15%) than hikers (6%). There was a significant difference in the bodily location of injuries between mountain bikers and hikers (χ2[4, n=610]=177.39; P<0.001).
Physiologic measurement of ambulance-transported mountain bikers and hikers outside of normal range according to the NEWS2 classification system.
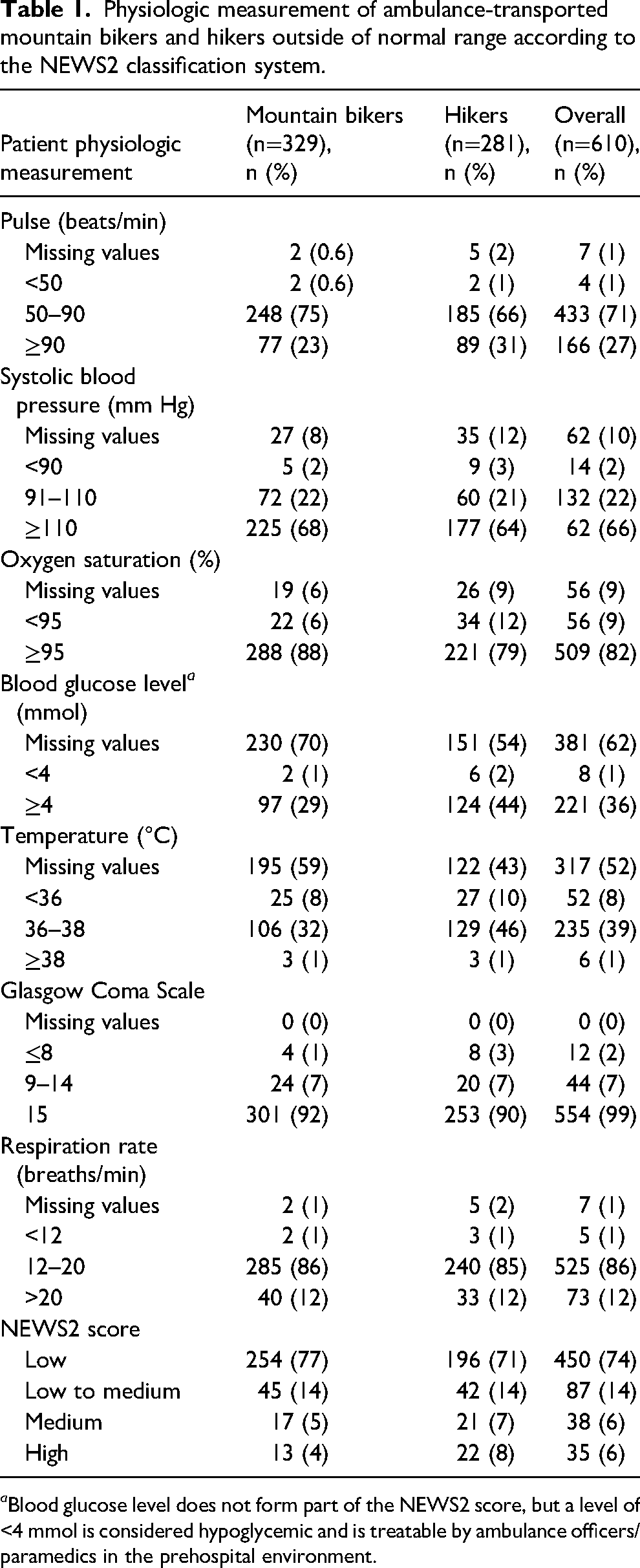
a Blood glucose level does not form part of the NEWS2 score, but a level of <4 mmol is considered hypoglycemic and is treatable by ambulance officers/paramedics in the prehospital environment.
Injury locations for ambulance-transported mountain bikers and hikers.
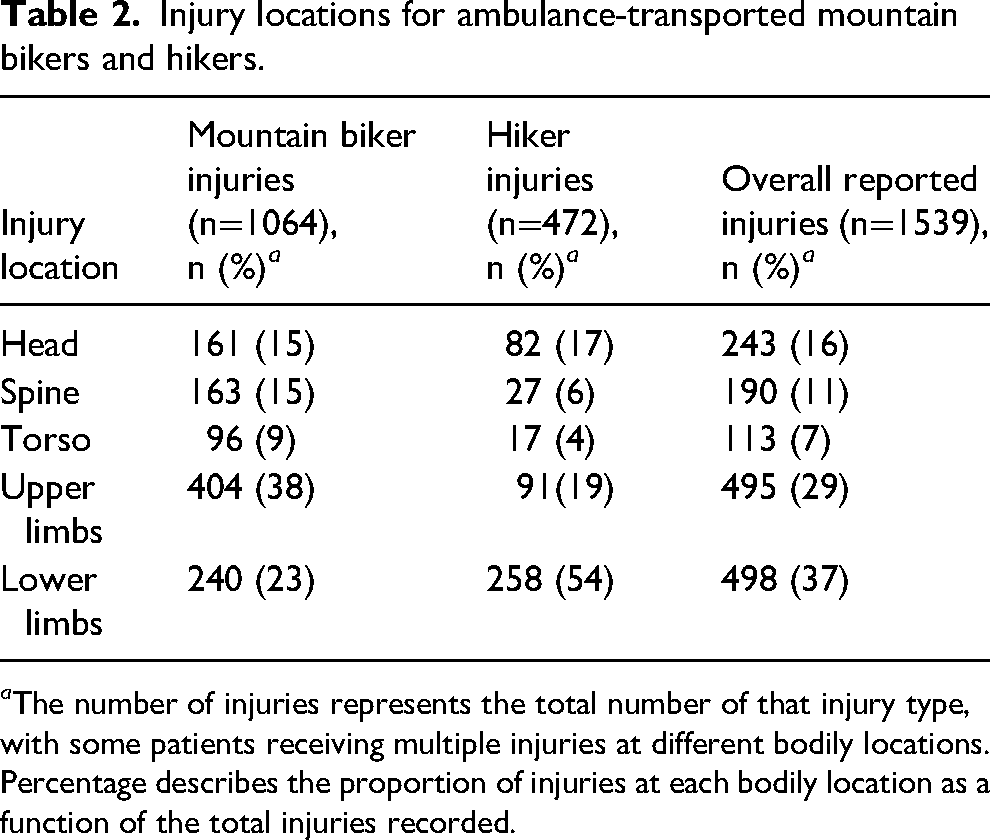
a The number of injuries represents the total number of that injury type, with some patients receiving multiple injuries at different bodily locations. Percentage describes the proportion of injuries at each bodily location as a function of the total injuries recorded.
The interventions administered to the study patients are presented in Table 3. A total of 245 (74%) mountain bikers and 190 (67%) hikers received analgesia. Of all analgesic doses administered, mountain bikers had a total of 886 (68%) doses administered, with hikers receiving 425 (32%) doses, a mean of 4 and 3 doses for mountain bikers and hikers, respectively.
Interventions and medications given to ambulance-transported mountain bikers and hikers.
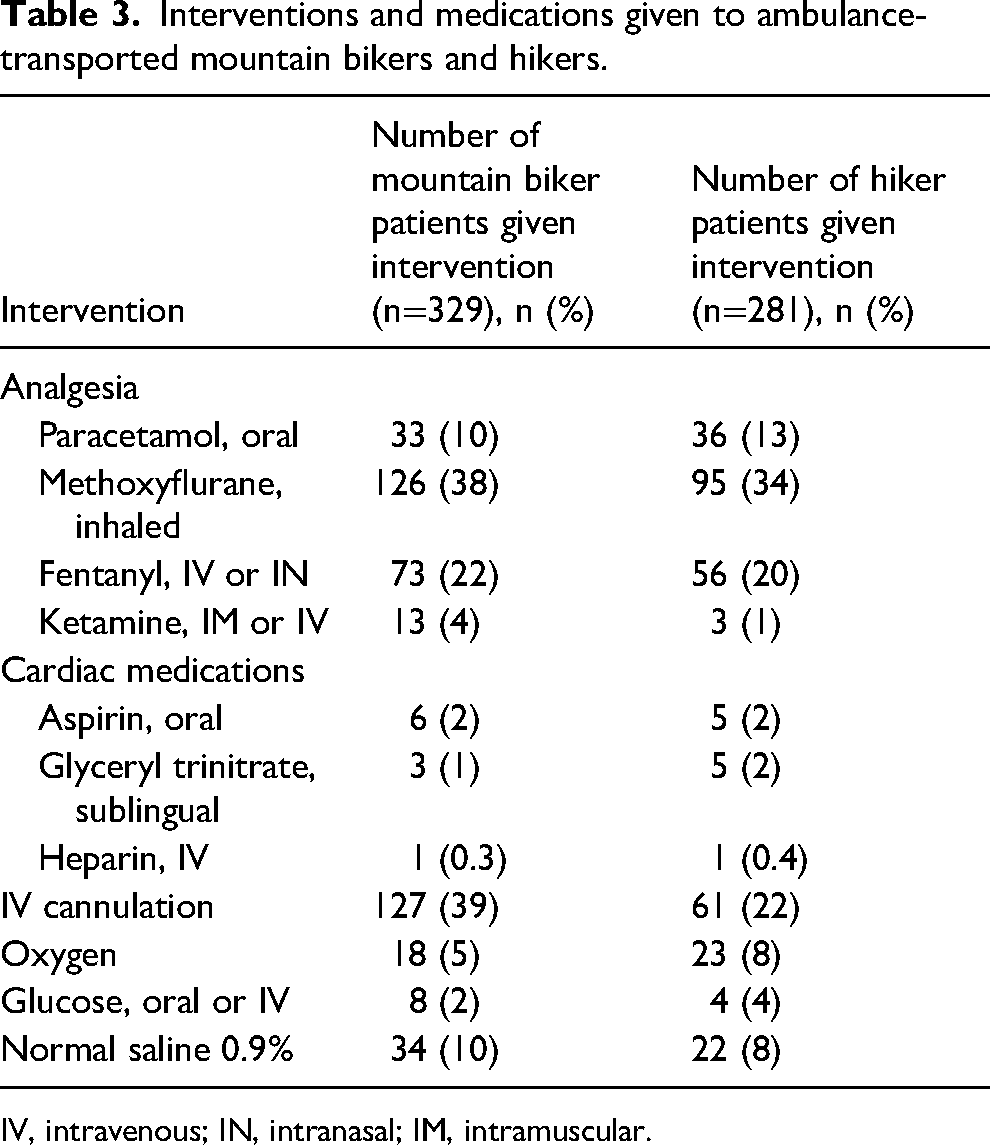
IV, intravenous; IN, intranasal; IM, intramuscular.
Unadjusted analysis showed a significant association (P=0.0372) between the primary outcome (ie, presence of more clinical severity as defined by having a NEWS2 score above low risk) and the activity being undertaken, with hikers being more likely than mountain bikers to have higher-severity NEWS2 scores (odds ratio [OR]=1.5; 95% CI, 1.02–2.1; P=0.037; Table 4). Patients with a medical etiology had an increased risk of having a higher NEWS2 score (OR=2.5; 95% CI, 1.7–3.7; P<0.0001) (Table 4). Ambulance dispatch priority 2 reduced the incidence of reporting more severe NEWS2 scores (OR=0.4; 95% CI, 0.2–0.5; P<0.0001), as did the age category being 20–39 y (OR=0.5; 95% CI, 0.3–0.97; P=0.038; Table 4). No association was found between the primary outcome of being of higher clinical severity and sex, total prehospital interval, or the presence of a suspected fracture. Results of all the univariate analyses are shown in Table 4.
Unadjusted odds ratios for ambulance-transported mountain bikers and hikers being of higher clinical risk as defined by NEWS2 score.
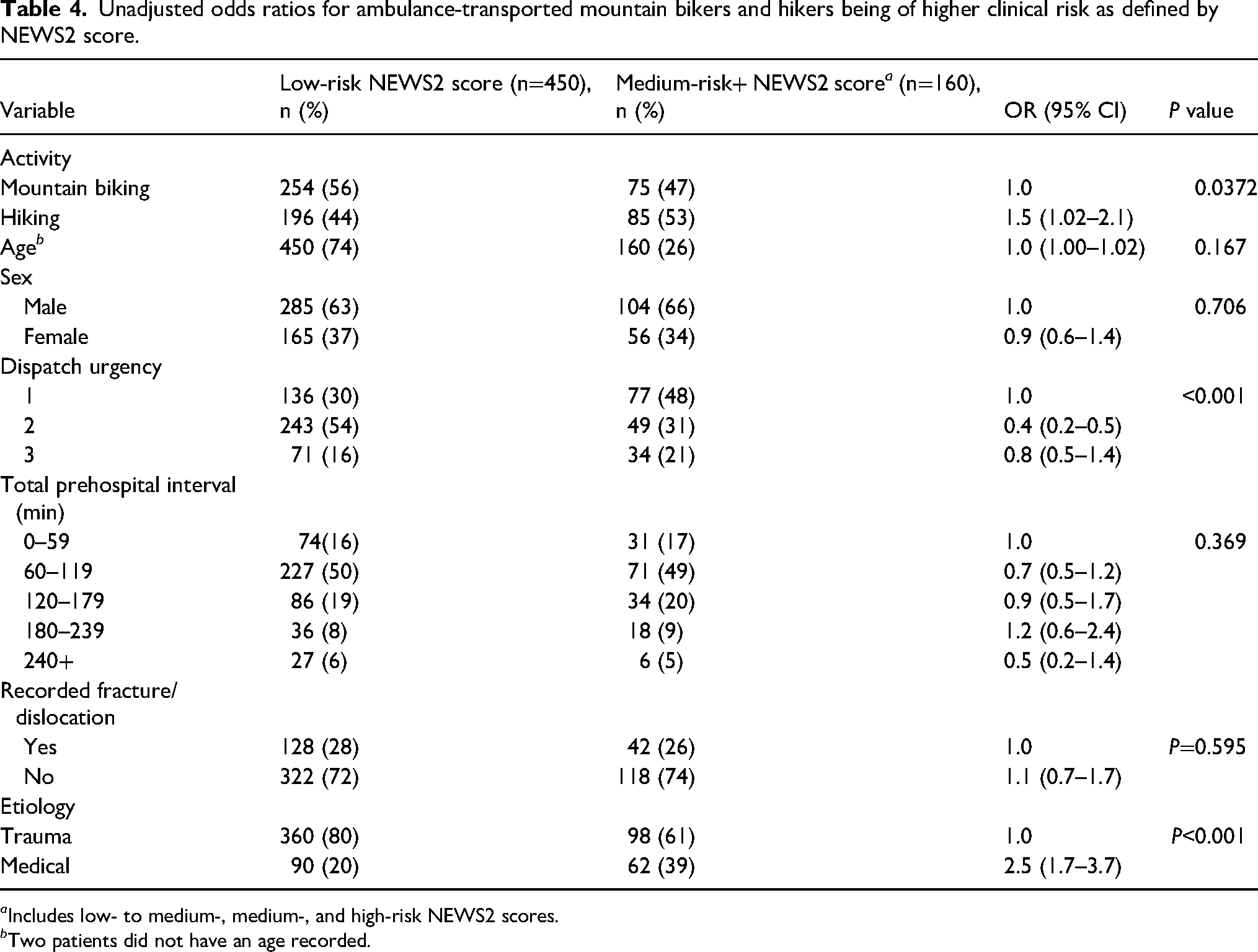
a Includes low- to medium-, medium-, and high-risk NEWS2 scores.
b Two patients did not have an age recorded.
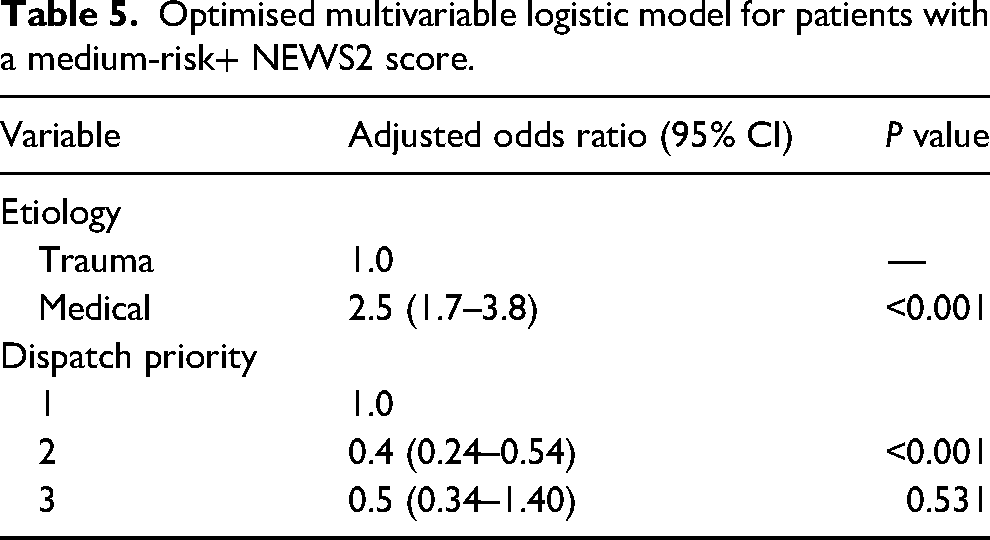
After post hoc variable selection, the final multivariate model included etiology of the condition and dispatch priority (Table 5). The Hosmer-Lemeshow goodness-of-fit test indicated adequate fit with a P value of 0.0358. Medical etiology was significantly more likely to result in higher NEWS2 scores, indicating higher severity of the condition than trauma-related injuries. Cases that were dispatched on a priority 2 had a significantly lower likelihood of having higher NEWS2 scores than cases dispatched on priority 1.
Optimised multivariable logistic model for patients with a medium-risk+ NEWS2 score.
Discussion
Our study describes patients who required ambulance transport to hospital while using trails for mountain biking or hiking. In our cohort of 610 patients, we found that mountain bikers were most frequently injured in the upper limbs and that hikers were most commonly injured in the lower limbs. We additionally aimed to determine whether mountain bikers had a higher severity of presentation than hikers. We found that hikers had a statistically significantly higher clinical risk than mountain bikers, as defined by NEWS2 scores. However, activity undertaken was not found to be significantly associated with higher NEWS2 scores after analysis with multivariable logistic regression; only etiology of the condition and dispatch priority of the ambulance demonstrated a significant association.
Descriptive Epidemiology
Mountain bikers requiring ambulance assistance were significantly younger than hikers, and this is consistent with previously reported literature on the median ages of these cohorts.9,11,31 Previous literature has reported hikers requiring EMS assistance to be older than we found. 32 However, the median age of injured mountain bikers in our study (24–48 y) was slightly higher than that in other published studies (15–33 y).7-9,11,33 Our large predominance of males (83%) is consistent with both participation data for both WA and other mountain bike injury studies.5,7 Mountain bikers had significantly shorter overall prehospital contact intervals than hikers, at 90 min compared with 111 min. This may be explained by the nature of the trails in WA, with mountain biking trails designed around central hubs with proximal road access. Cases that were attended by air ambulance had significantly greater prehospital intervals. Air ambulances are used to access patients who cannot be reached by road ambulance through use of their winching capability, which led to longer prehospital intervals (134 [98–152] min vs 95 [65–152] min for road ambulance) due to the difficulties in locating these patients and the technical nature of winch rescues. Once access is gained to the patients, they are treated by a single clinician instead of the two found on road ambulances.
Bodily Injury Locations
The same proportion of mountain bikers and hikers had a suspected fracture or dislocation, with 92 (28%) mountain bikers and 78 (28%) hikers despite a higher incidence (92% vs 55%) of all mountain biking ambulance attendances being for trauma-related reasons. Previous work investigating mountain bike injuries found that fractures constituted between 30 and 43% of reported injuries.7,11,33 Our figure is likely lower because it only included 610 patients transported by ambulance and did not capture self-presentations to hospital. One prior report on the nature of hiking injuries reported 9% of rescued hikers to have sustained a fracture, 18 well below our reported figure of 28%. However, the previous work also included very minor injuries that normally would not result in an ambulance callout. 18 Additionally, hikers in our dataset sustained the same proportion of suspected fractures as mountain bikers, but only 55% of callouts were for trauma-related reasons as opposed to 92% for mountain bikers. People who are older than 50 y have been shown to sustain a higher incidence of fractures, which is likely true of hikers within our study, who had a median age of 49 y. 34
Mountain bikers sustained predominantly upper limb injuries compared with hikers, who sustained mainly lower limb injuries (38% vs 54% of all injuries transported). This is consistent with previous work that indicates that mountain bikers sustain mainly upper limb injuries and hikers lower limb injuries.3,7,15,17-19,31,32 Despite the fact that helmets are mandatory when cycling in WA, both mountain bikers and hikers recorded a similar proportion of injuries to the head (15% and 17%, respectively), likely due to the higher velocities involved in the mountain biking incidents. Previous work reporting injury epidemiology to mountain bikers found a similar proportion of injuries to the head.5,6,34
Patient Severity
We examined vital signs independently as well as in combination as part of the NEWS2 score. Of the patients who had a pulse recorded out of the normal range, only a small proportion were bradycardic, with the majority being tachycardic with a pulse >90 beats/min. Tachycardia may have been associated with pain given the proportion of patients with suspected fractures and vital signs being taken prior to analgesia administration. 35 While blood loss also may explain the presence of tachycardia, it is not a likely cause in our reported patients because none had external bleeding of >500 mL reported. Around 9% of mountain bikers and 19% of hikers had oxygen saturations below 95%, but only 7% of mountain bikers and 8% of hikers had oxygen administered. While the NEWS2 scoring system records oxygen saturations below 95% as being outside of the normal range, SJWA clinical practice guidelines indicate that oxygen should be applied when saturations are below 92%, which may explain the relatively lower proportion of patients being given supplemental oxygen. Hypothermia was reported in 25 (8%) mountain bikers and 30 (11%) hikers. While hypothermia (<36°C) in hikers may indicate exposure, it is more surprising to see a similar proportion in mountain bikers whose rides are on designated trails and mostly centered around trail hubs, making getting lost presumably less likely. It is possible that clothing choices for vigorous activity such as mountain biking leaves riders exposed when they are injured and stationary, with evaporative cooling from sweat therefore causing significant heat loss. 36 Previous work found that day hikers reported being underprepared for nutrition, hydration, and insulation. 37 One study reported that 18% of hikers indicated that they “felt cold” on their day hike, and were they to become injured or immobile, then this would leave them exposed to exertional heat loss and potential hypothermia. 38 We were unable to find previous work documenting the epidemiology or mechanism of hypothermia in mountain bikers. Similarly, we were unable to find previous epidemiologic studies on hypoglycemia in mountain bikers or hikers, but in this study we found 16 cases of hypoglycemia treated by 15 doses of glucose, either orally or intravenously, to 12 patients. A reduced Galsgow Coma Scale of <14 was seen in 28 (9%) mountain bikers and 28 (10%) hikers. There may be multiple potential causes for this, such as the hypoglycemia previously noted or a closed head injury causing concussion. To our knowledge, no work has previously assessed the vital signs of mountain bikers and hikers in the prehospital environment.
Patients whose condition had a medical etiology had greater likelihood of a higher NEWS2 score (OR=2.5; 95% CI, 1.7–3.8) than patients who had a trauma-related etiology. Hikers had a greater proportion of medical complaints, with 45% of ambulance callouts being for medical causes compared with 8% of mountain bikers. In trauma etiology cases, the medium-risk+ NEWS2 severity was 21.4.%. In medical cases, the medium-risk+ NEWS2 severity was 40.8%. If the dispatch was priority 1, the medium-risk+ severity, as defined by the NEWS2 score, was 36.2%. For priority 2 and priority 3 dispatches, the relative risks were 16.8% and 32.4%, respectively. This possibly indicates an under-triage of priority 3 cases because the risk of them having a higher severity, as defined by NEWS2 score, is greater than that of priority 2 cases.
In the final multivariable logistic regression model describing the factors associated with higher NEWS2 scores, only etiology and dispatch priority remained, which is somewhat in contrast with the common perception of the risks of mountain biking. Medical (nontraumatic) etiology of the presenting condition was significantly more likely (OR=2.5; 95% CI, 1.7–3.8) to result in a higher NEWS2 score, indicating higher severity of the condition even after adjustment for age. This is a surprising finding considering the inherent selection bias of only including ambulance-transported cases and not capturing more minor hospital self-presentations or self-treatments. Patients who had an ambulance dispatched as a priority 2 were less likely to have higher NEWS2 scores than patients who had an ambulance dispatched under priority 1 (OR=0.4; 95% CI, 0.24–0.54).
Clinical Interventions
Mountain bikers had a higher proportion of intravenous cannulations than hikers at 39% vs 22%. Less than 39% of mountain bikers received intravenous medication interventions, so the reason for the high proportion of cannulations is unclear and warrants further investigation, particularly considering the high rate of infection from Staphylococcus aureus with prehospital cannulation.39,40 Normal saline boluses were given 41 times to 34 (10%) mountain bikers and 36 times to 22 (8%) hikers. Normal saline is indicated to be administered in a bolus dose when patients have demonstrated hypotension or in cases where patients require fluid replacement indicating the possibility of dehydration in these patients.
A total of 5 (1.5%) mountain bikers and 6 (2.1%) hikers were treated for possible acute coronary syndromes using aspirin, nitroglycerin, and heparin. While no research was available on whether cardiac complaints are common among mountain bikers, previous work has documented cardiac complications during hiking, including 50% of hiking deaths being sudden cardiac arrests. 41 We report fewer than 5 patients requiring cardiopulmonary resuscitation, none of whom achieved a return of spontaneous circulation. Gstaettner reported 30 fatalities within national parks in WA over a 6-y period, the majority of these either drowning or falls while rock fishing. 20 Two fatalities while hiking were reported by Gstaettner, but due to patient confidentiality, we were unable to determine whether these cases also were reported in our dataset. 20
There are multiple limitations of this study. It is retrospective and observational. Paramedics and ambulance personnel have limited ability to diagnose in the prehospital setting, and therefore, any reported suspected fractures or dislocations are subject to misdiagnosis. Patient outcomes and injuries, as reported by the treating personnel, were not verified with hospital data. The number of patients in the dataset did limit the potential for subgroup analyses. This study does not include patients who self-present to hospital and do not call for ambulance assistance. Mode of ambulance transport, air or ground, was not considered as part of this study. We investigated mountain bikers as a single cohort because it was not possible to determine the exact type of mountain biking being undertaken (downhill vs cross-country) given that paramedics do not routinely record this type of information. This meant that we could not compare the severity of outcomes for the different types of mountain biking.
Conclusions
In our cohort, mountain bikers sustained predominantly upper limb fractures and hikers sustained a larger proportion of lower limb fractures. These findings highlight the importance of correct protective clothing for both mountain bikers (eg, arm guards and shoulder pads) and hikers (eg, well-fitted, suitably soled, high ankle boots). The number of mountain bikers or hikers being hypothermic or needing fluid replacement suggests the importance of education around clothing choices and adequate hydration. 42 Trauma-related incidents were more common in mountain bikers, but hikers had a higher level of clinical risk, as determined by the NEWS2 scores. Overall, mountain bikers and hikers who are transported to hospital were more likely to have a higher NEWS2 score if the call was for a medical etiology than for a trauma-related one. Hikers new to the sport who have risk factors for cardiac conditions should consult with their general practitioners about their current fitness to undertake such an activity. Additionally, experienced hikers should consider their current health status, environmental conditions, and limited access to assistance before setting out on a hike in remote areas.
Footnotes
Acknowledgments
The authors thank St John Ambulance Western Australia for their support.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PJB is employed at St John Ambulance WA as a paid paramedic. DB is employed at St John Ambulance WA as the executive director of clinical operations. JF is an adjunct research professor at St John Ambulance WA who receives untagged research funds.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: St John Ambulance WA covers part of the salary of PJB and a full salary for DB.