
Abstract
Background:
Trauma was the fifth leading cause of death in Hong Kong in 2013.4 Injuries caused by falls ranked first in traumatic brain injury (TBI) cases among older adults (51%).5 Elderly trauma patients face an increased risk of adverse consequences6 from trauma compared with their younger counterparts, as advanced age itself is already a well-recognized risk factor for less favorable outcomes following trauma. Therefore, identifying factors associated with significant brain injury in geriatric patients in A&E triage is crucial in providing timely care to these patients.
Objectives:
To identify the risk factors for geriatric patients with significant brain injury from ground-level falls and to formulate their association of risk factors with significant brain injury as a consequence from ground-level falls.
Methods:
This was a retrospective study with data collected from the Clinical Data Analysis and Reporting System of Queen Mary Hospital from 1 January 2013 to 31 December 2015. A total of 1101 cases were identified.
Results:
There were 76% of the recruited patients with a normal computed tomography scan. However, the remaining 24% had computed tomography scans indicative of brain injury. Severe head injuries were scored 3 -8 on the Glasgow Coma Scale and moderate head injuries were scored 9 -12. Respectively, these were 20 times (p = 0.005) and 5 times (p = 0.002) more likely to have positive computed tomography findings than patients with a Glasgow Coma Scale score from 13 to 15. Patients with loss of consciousness were two times more likely to have a positive computed tomography result than those without loss of consciousness (p = 0.001). Although warfarin use is a well-established risk factor for intracranial hemorrhage after head injury, in our dataset, the result was not statistically significant. However, the use of new oral anti-coagulants was associated with positive computed tomography findings with patients taking new oral anti-coagulants 2.3 times more likely to have positive computed tomography findings compared with those with no anticoagulant use (p = 0.033).
Conclusions:
Early detection of patients with significant brain injury and aggressive management may prevent secondary injury from the complications of brain injury, hence improving patient mortality and morbidity, and reducing hospital stay and health care costs.
Introduction
There are no doubts that the aging population is increasing worldwide and Hong Kong is no exception. Population age is expected to increase rapidly in the coming 20 years. 1 As the number of elderly in the general population grows, the demand for geriatric emergency care rises. 2 Thus, improved healthcare services are required for this specific group. Although there is no well-established consensus on a cut-off age for geriatric patients, the age of 65 is frequently used in the literature. 3
Trauma was the fifth leading cause of death in Hong Kong in 2013. 4 Injuries caused by falls ranked first in traumatic brain injury (TBI) cases among older adults (51%). 5 Elderly trauma patients face an increased risk of adverse consequences 6 from trauma compared with their younger counterparts, as advanced age itself is already a well-recognized risk factor for less favorable outcomes following trauma. 7
Atypical presentation of symptoms, polypharmacy, comorbidity, communication problems, and altered mental status impede the ability of healthcare workers to gather relevant information. 8 Common health conditions such as diabetes mellitus (DM), previous cerebrovascular events, hypertension (HT), heart disease, chronic obstructive pulmonary disease (COPD), and dementia complicate the management of care. 5 Moreover, elderly patients are easily under-triaged due to lack of awareness among healthcare workers of their potential major injuries. 9 In addition, nurses may neglect the harmful consequences of geriatric trauma as they misinterpret patient symptoms as the effect of co-morbidities. All these factors lead to increased morbidity and mortality in geriatric trauma patients when compared to the younger population. 7
Although there is an in-hospital trauma activation protocol in each trauma center of Hospital Authority Accident and Emergency Departments (A&E) in Hong Kong, the protocol is not age specific. A well-organized trauma activation pathway for TBI in the elderly has not been developed. Due to age-related biological differences, it is always challenging to determine the severity of injuries in geriatric patients during triage in A&Es. 6 Also, the activation criteria of trauma call for adults may not be appropriate for the elderly. 10 Therefore, identifying factors associated with significant brain injury in geriatric patients in A&E triage is crucial in providing timely care to these patients. Establishment of standard guidelines for local geriatric trauma team activation could also be considered.
Aim
The aim of this research is to identify risk factors for significant brain injury in geriatric patients from ground-level fall in a local A&E in Hong Kong.
Objectives
To identify the risk factors for geriatric patients with significant brain injury from ground-level falls;
To formulate their association of risk factors with significant brain injury as a consequence from ground-level falls.
Research question
What risk factors identified at triage are related to significant brain injury of geriatric head injury patients from ground-level fall in A&E?
Methodology
Study design
This was a retrospective study using data collected from the Clinical Data Analysis and Reporting System (CDARS) of Queen Mary Hospital (QMH), Hong Kong, from 1 January 2013 to 31 December 2015.
Definition of key terms
Patients aged 65 or above were regarded as geriatrics.11,12 Significant brain injury was defined as intracranial injury with a positive computed tomography (CT) brain finding (e.g. intracranial hemorrhage). CT imaging of the head was the primary investigation of choice in head injury. 13 This is a rapid and reliable tool to detect significant brain trauma.14,15 Our study used the patients’ initial CT scan result after their A&E admission as reference. Ground-level fall was defined as a fall from below 2 m. 11
Patient selection
Patients aged 65 or above with a blunt head injury due to a ground-level fall admitted through QMH A&E were recruited for this study. Patients were identified from CDARS using the International Classification of Diseases–10th Revision (ICD10 version 2010) codes (specifically S00.9, superficial injury of head, part unspecified; S02.0, closed fracture of vault of skull; S02.1, closed fracture of base of skull; S02.7, closed multiple fractures involving skull and facial bones; S02.9, closed fracture of skull and facial bones, part unspecified; S06.0, concussion, without open intracranial wound; S06.2, diffuse brain injury, without open intracranial wound; S06.3, focal brain injury, without open intracranial wound; S06.4, epidural hemorrhage, without open intracranial wound; S06.5, traumatic subdural hemorrhage (SDH), without open intracranial wound; S06.6, traumatic subarachnoid hemorrhage (SAH), without open intracranial wound; S07.9, crushing injury of head, part unspecified; S09.7, multiple injury of head; S09.9, unspecified injury of head; T00.0, superficial injuries involving head and neck; and T90.8, sequelae of other specified injuries of head). Patients with pre-hospital alcohol consumption and those transferred from other hospitals or units were excluded. The patient selection flow chart is shown in Figure 1.
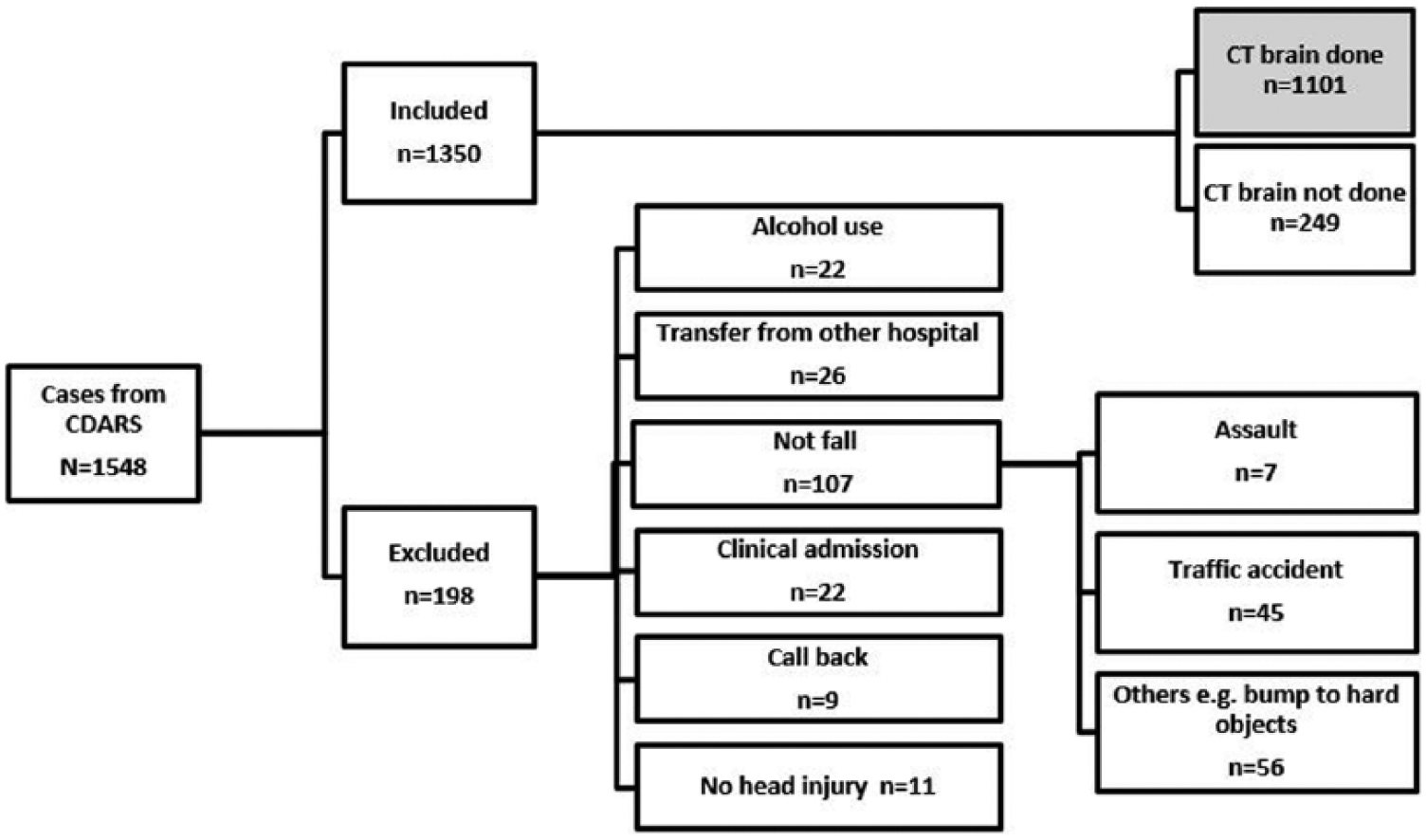
Patient selection flow chart.
Data analysis
Baseline demographics and vital signs including the Glasgow Coma Scale (GCS), systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse rate, respiration rate (RR), and pupils equal and reactive to light (PEARL) at triage were collected. Their patterns of injury, episodes of loss of consciousness (LOC), amnesia, or vomiting were also documented. Patients’ medical co-morbidities (HT, DM, cardiovascular diseases (CVA), stroke, and dementia) and their use of anti-platelet or anti-coagulant medications were also retrieved. Outcome measurements included positive CT findings from initial brain scans, inpatient mortality, and whether craniotomy was performed. CT findings were categorized based on the predominant blood distribution of the scan report.
Categorical data were analyzed by descriptive statistics. The chi-square test was used to identify any difference between the variables with the CT results. Statistically significant variables were then processed to the univariate logistic regression to predict the association with the CT results as adjusted odds ratio (AOR). Some other parameters believed to be important in TBI identification were also entered for AOR calculations. A p-value of < 0.05 was considered as statistically significant. Statistical analysis was done using Statistical Package for the Social Sciences (SPSS) 24.0.
Ethical considerations
The Institutional Review Board (IRB) of the Hong Kong West Cluster of Hospitals Authority approved this research on 7 January 2016 (IRB reference number: UW 16-028).
Results
Study group physical characteristics
Patient demographics are shown in Table 1. In 1101 patients who had a CT scan, 56% were female and their mean age was 83 years. The mean SBP and DBP were 164 and 82 mmHg, respectively. Over two-thirds of the patient population had a mean atrial pressure (MAP) ranging from 100 to 149 mmHg, and the mean MAP was 110 mmHg. The RR ranged from 12 to 48/min and the mode of the RR was 16/min. The mean pulse rate was 80 bpm and ranged from 44 to 150 bpm.
Demographics and clinical data for 1101 elderly patients with TBI.
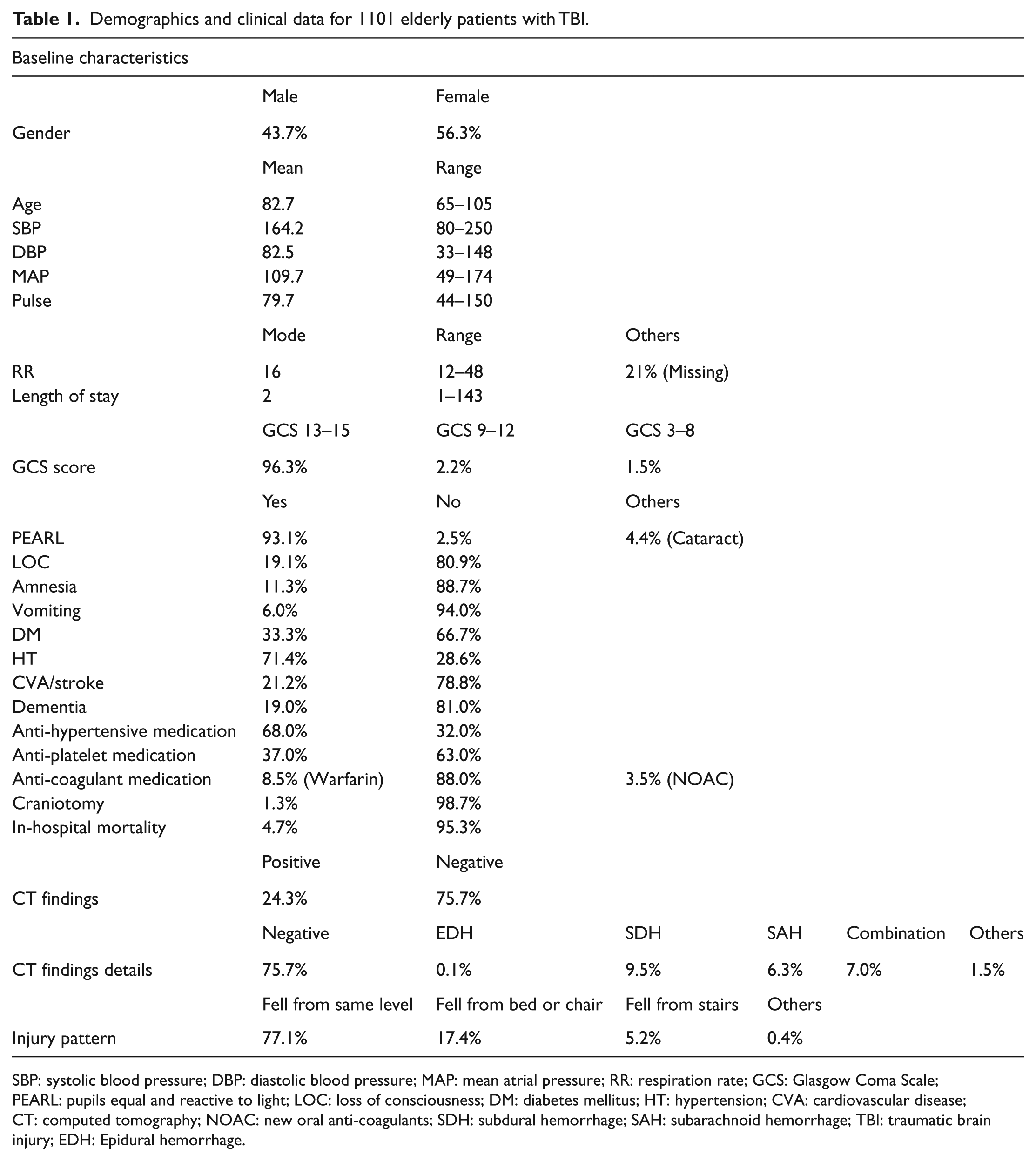
SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean atrial pressure; RR: respiration rate; GCS: Glasgow Coma Scale; PEARL: pupils equal and reactive to light; LOC: loss of consciousness; DM: diabetes mellitus; HT: hypertension; CVA: cardiovascular disease; CT: computed tomography; NOAC: new oral anti-coagulants; SDH: subdural hemorrhage; SAH: subarachnoid hemorrhage; TBI: traumatic brain injury; EDH: Epidural hemorrhage.
Around 96% of the population suffered from minor head injury with GCS score of 13–15. There were 93.1% of the patients with PEARL, no LOC (80.9%), no amnesia (88.7%), and no vomiting (94.0%). More than 3/4 of the patients fell from the same level, 17% from a chair or a bed and 5% from stairs less than 2 m in height.
Study group past health
Among the 1101 cases, 33% had DM and 71% had HT. There were 21% and 19% of patients who had CVA or dementia, respectively. There were 68% and 37% of patients taking anti-HT drugs and anti-platelet drugs, respectively. In total, 88% of patients did not consume any anti-coagulant medication; 8.5% and 3.5% were taking warfarin or new oral anti-coagulants (NOACs) such as rivaroxaban, dabigatran, and apixaban.
A normal CT finding was observed in 76% of patients. Of the remaining 24% with a positive CT result, SDH (9.5%) and SAH (6.3%) were ranked as the top two types of injuries. Multiple types of hemorrhage were seen in 7% of patients. Only 1.3% of patients underwent craniotomy during their stay and the in-hospital mortality was 4.7%. Most patients were discharged within 2 days and their length of stay ranged from 1 to 143 days.
Chi-square test
A chi-square test was used to identify significant differences between variables and the CT result as shown in Table 2. Several variables were identified to have statistically significant relationship with the CT result as follows: gender (p-value < 0.001), GCS (p-value < 0.001), PEARL (p-value < 0.001), LOC (p-value < 0.001), amnesia (p-value < 0.001), vomiting (p-value < 0.001), injury pattern (p-value = 0.012), other major injury (p-value = 0.001), history of dementia (p-value = 0.004), and the use of anti-coagulant medication (p-value = 0.007).
The difference between variables and the CT result in chi-square test.
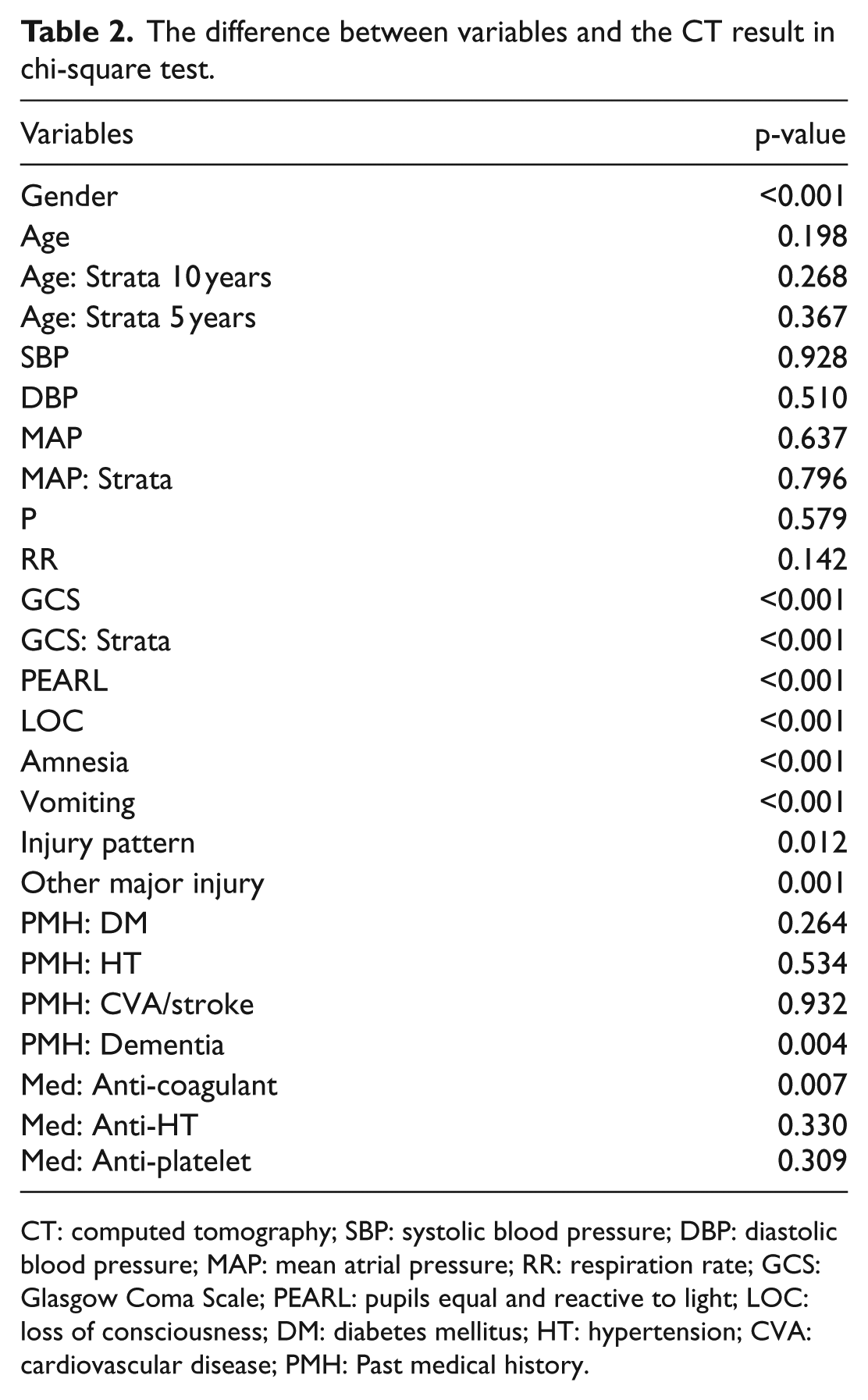
CT: computed tomography; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean atrial pressure; RR: respiration rate; GCS: Glasgow Coma Scale; PEARL: pupils equal and reactive to light; LOC: loss of consciousness; DM: diabetes mellitus; HT: hypertension; CVA: cardiovascular disease; PMH: Past medical history.
Association prediction
To further establish the association of each independent variable with the positive CT findings, AORs were calculated by logistic regression (Table 3).
Association prediction with logistic regression.
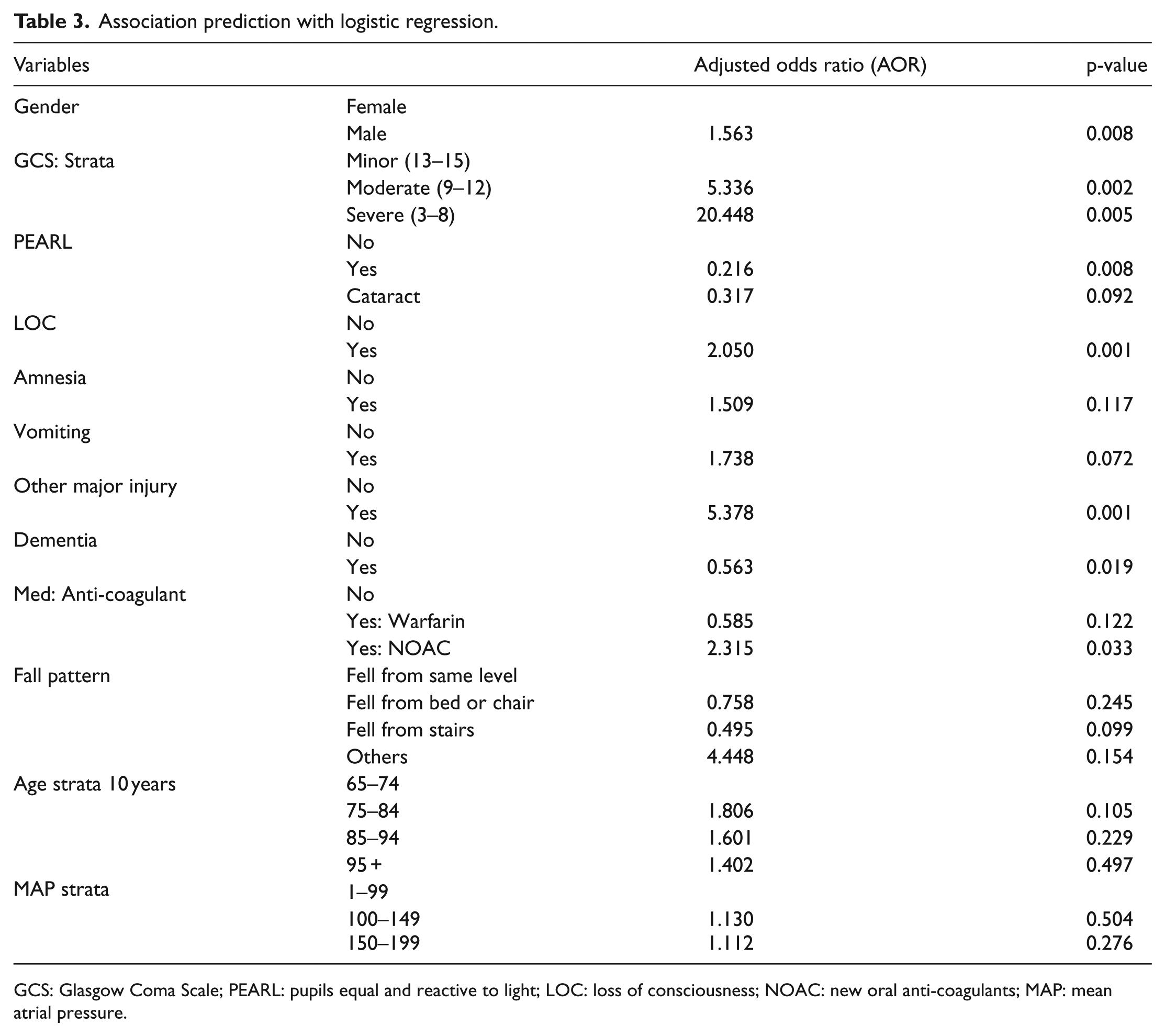
GCS: Glasgow Coma Scale; PEARL: pupils equal and reactive to light; LOC: loss of consciousness; NOAC: new oral anti-coagulants; MAP: mean atrial pressure.
Males were 1.6 times more likely to have a hemorrhage than females (p = 0.008). Patients who had a severe head injury with a GCS score of 3–8 and moderate head injury with GCS score of 9–12 were 20 times (p = 0.005) and 5 times (p = 0.002) more likely to have positive CT findings, respectively, than patients with a GCS score of 13–15. Patients with LOC were two times more likely to have a positive CT result than those without LOC (p = 0.001). Patients with a major injury other than head injury, mainly injuries with facial bone fractures or skull fractures, were 5.3 times more likely to have intracranial hemorrhage (p = 0.001). Although positive CT findings were 1.5 and 1.7 times more likely if the patients experienced amnesia and vomiting, they were not statistically significant. Dementia patients were 0.437 times less likely to have positive brain scans than those without dementia (p = 0.019). Although warfarin use is a well-established risk factor for intracranial hemorrhage after head injury, the result was not statistically significant in this study. However, the use of NOAC led to patients being 2.3 times more likely to have positive CT findings compared with those with no anti-coagulant use (p = 0.033).
Discussion
Ground-level falls are traditionally regarded to have a relatively low energy impact to patients. Yet in our study, certain number of patients (24%) experienced TBI from ground-level falls. This number emphasizes that even this kind of low energy impact is a significant issue for elderly people.16,17
Both moderate (9–12) and severe (3–8) GCS scores were found to be a strong risk factor for positive findings in CT scans (p = 0.005 and p = 0.002, respectively). GCS is a well-established method and has been used in medical practice since 1974. The GCS is focused on the importance of central nervous system and is used to assess the extent and severity of neurological deficit. 18 Although GCS is helpful in the detection of brain injury, studies have shown that it may not be a sensitive indicator in geriatric trauma; elderly patients had poorer outcomes even if they had a relatively “normal” GCS score.10,18 In agreement, our data showed that patients with GCS score of 14 had nearly a fivefold greater risk of a positive CT finding compared to those with a GCS score of 15 (Table 4). The majority of elderly patients present to A&E with a high GCS score (96% had a GCS score of 13–15) in our daily clinical practice. Hence, triage nurses should maintain a high level of suspicion of an underlying brain injury even if the patient appeared to have a relatively normal GCS.
GCS score logistic regression.
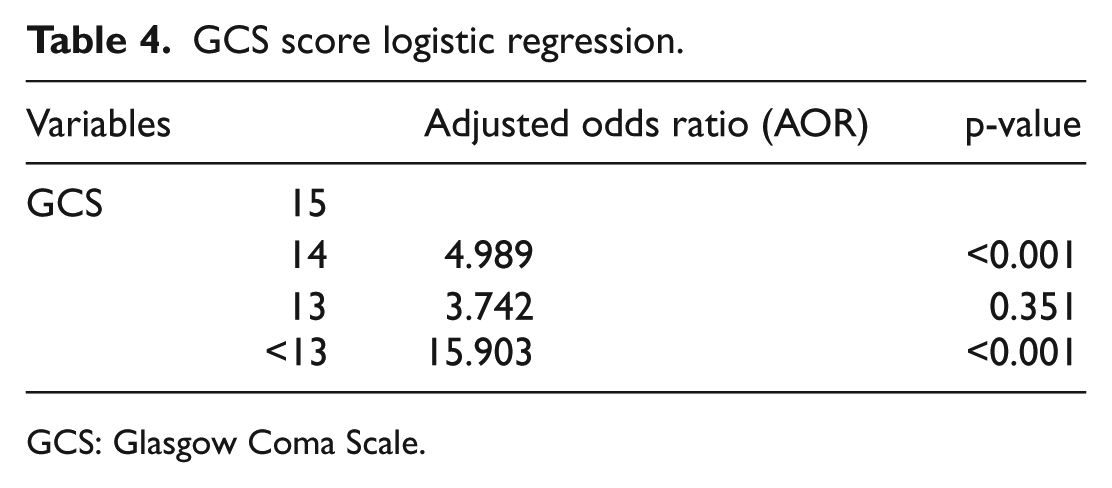
GCS: Glasgow Coma Scale.
Several countries have already developed guidelines for CT scan in minor head injuries. For example, LOC, amnesia, and vomiting have been adopted by the National Institute for Health and Clinical excellence (NICE) guidelines in the United Kingdom and also in the Canadian CT head rules. 13 Literature has also shown that a history of LOC is a significant predictive factor in intracranial injury.14–16 Our study is consistent with the literature (AOR of LOC = 2.05; p = 0.001).
In our study, signs and symptoms of facial bone fractures or skull fractures were counted as a major injury other than head injury. Barrow et al. 14 studied patients in an A&E in London, England, and identified injuries above the clavicles as one of the predictors of a positive CT scan result. Our project revealed similar findings.
Unlike many studies, we did not identify a statistically significant association between warfarin use and brain injury. However, we found that NOAC use was a risk factor in TBI (AOR = 2.3; p = 0.033). NOACs like rivaroxaban, dabigatran, and apixaban are relatively new medications compared to warfarin. There are limited studies which compare the effect of these medicines with warfarin in TBI. We could only identify two case reports documenting dabigatran and TBI published to date. Wassef et al. 19 reported three cases in which dabigatran may lower the threshold of energy required to cause intracranial hemorrhage. With increasing numbers of patients using these new medications, A&E nurses should pay more attention to this group in the context of minor head injury. There was no significant association between TBI and the use of anti-platelet drugs. This was consistent with published findings, showing that anti-platelet medication does not increase mortality in intracranial hemorrhage. 12
Fall patterns, age strata, and MAP were entered into the statistical calculations to show statistical significance (Table 3). Age itself is already an established predictor for mortality or adverse outcomes in head injury from ground-level falls.11,17 There were no differences in the risk of intracranial hemorrhage in different age groups in elderly patients. It is possible that increased blood pressure may be an indicator of intracranial hemorrhage risk, as MAP is closely related to intracranial pressure. However, our study did not identify statistically significant association between MAP risk and TBI (p = 0.276). The existing literature only shows that a history of HT leads to a higher chance of intracranial hemorrhage; however, the exact role of MAP was not examined. 16
There are three main applications which can be derived from the research findings: (1) the data broadens insights for the early recognition of geriatric patients at high risk of TBI after minor falls, (2) enhancement of triage questioning skills, and (3) enhancement of triage documentation. Our data indicated that 31% of the CT scan patients were categorized as semi-urgent at triage. These patients were at elevated risk as extended waiting times might delay their treatment.
There are five action plans for the applications stated above. First, we will provide information sharing sessions for colleagues to inform them of the characteristics, pathophysiology, and physiological response of geriatric traumatic patients after head injury. Second, we will provide action cards with short and simple questions for the elderly as they often have difficulties in verbal expression and comprehension. These questions will be designed to identify specific signs and symptoms of significant brain injuries. The action cards also will list the prevailing NOACs for the triage nurses reference. Third, in order to have a clearer clinical picture, we will advocate nurse colleagues to document GCS in addition to AVPU (A: alert; V responsive to verbal stimuli; P: responsive to painful stimuli; U: unresponsive) on the A&E card when triaging geriatric TBI patients. Fourth, we will reinforce the importance of the PEARL exam at triage which was previously easily neglected. Finally, we will consider adding a checklist by ink chop on A&E cards for head injury patients. Using the checklist, we hope to alert nursing colleagues for the early recognition of geriatric patients at high risk, as appropriate triage is a key determinant of better outcome after brain injury. For example, if an elderly got head injury with GCS of 14 or lower, history of LOC, and use of NOAC, we should put him into an urgent category for faster consultation plus CT scan investigation.
Limitations
There are several limitations in our study. First, it was a retrospective design and therefore has selection and information bias. Second, the cohort data were used from a single site; the findings thus lack the power of generalizability. Third, several data were missing from A&E records. Nurses usually used AVPU scale instead of the exact GCS score in some cards, which made it difficult to predict the exact GCS value. Doctors’ notes or admission notes were used for reference in those patients with missing GCS data, yet they might not be the firsthand data received at triage. Documentation of the RR was only compulsory since mid-2013, thus this parameter could not be used for all patients. Moreover, our study did not identify all pre-injury conditions. Patients with heart problems or a history of repeated falls were not recruited. Finally, our project only recruited hospitalized patients from CDARS which include admitted patients only. Potential cases who were not admitted to hospital may have been missed.
Future prospects
Geriatric trauma guidelines
Our study provides new insights into current A&E nursing triage practice. In Hong Kong, specific geriatric TBI triage criteria have not yet been developed. In future, we aim to formulate geriatric-specific trauma triage guidelines to correct these deficiencies. In some places, such as Ohio Emergency Medical Service in the United States, reformed guidelines have already been adopted. 20 The new guidelines adopted an adjusted GCS score for elderly people as one of the trauma center admission criteria. Likewise, a lower threshold of GCS score for traumatic geriatric patients may be considered in Hong Kong. On the other hand, we hope the risk factors identified in our study will be useful in developing a new scoring system and ultimately form elements for geriatric trauma activation call development.
Fast track protocol
In order to examine whether there will be a decrease in mortality and morbidity in geriatric TBI patients, a prospective study of nursing fast track protocol for CT brain scans could be considered, using the risk factors identified in our study. This fast track may shorten the time to diagnosis and allow patients to receive prompt and appropriate treatment.
Conclusion
As stated above, fall injuries are the leading cause of fatal and non-fatal injuries among the geriatric population. In the coming years, the rapidly growing geriatric population poses a significant burden on our healthcare system. Increased A&E admission due to falls is expected and TBI is associated with serious consequences. It is necessary for nurses to be well-equipped with the related knowledge and triage skills for better care provision. Specialized triage guidelines for this patient population would be beneficial. Early detection of patients with significant brain injury and aggressive management may prevent secondary injury from the complications of brain injury, hence improving patient mortality and morbidity, and reducing hospital stay and health care costs. We hope the results from our study will inspire new insights to triage nurses for precise triage, ensuring the best care is given to our patients under limited available resources. By maintaining a high level of awareness of significant brain injury in this high risk group of geriatric patients, the number of cases miscategorized at triage could be minimized, and the survival rate of this group of patients maximized.
Footnotes
Declaration of conflicting interests
The authors declare that the manuscript has not been submitted to more than one journal for simultaneous consideration. The authors declare that the manuscript has not been published previously.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The authors declare that no data have been fabricated or manipulated (including images) to support your conclusions. The authors declare that no data, text, or theories by others are presented as if they were the authors own.
Informed consent
For this retrospective study, formal consent is not required.
Ethical approval
The Institutional Review Board (IRB) of the Hong Kong West Cluster of Hospitals Authority approved this research on 7 January 2016 (IRB reference number: UW 16-028).
Human rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.