
Abstract
Background
The American College of Surgeons Trauma Quality Improvement Program recommends a lower threshold for trauma activation on geriatric patients. We implemented the Modified Geriatric Trauma Activation Criteria (MGTAC) and assessed the clinical impact on geriatric trauma patients.
Methods
Geriatric trauma patients aged 65 years and over presenting between 1/1/2014 and 12/31/2020 were identified through the Trauma Registry. MGTAC were implemented on 3/1/2017, where patients aged 65 and above were rendered as Highest Level activations when presenting with no prior work-up. Those presenting from 1/1/2014 to 2/28/2017 were grouped as Standard Activation Criteria (SAC), and those presenting between 3/1/2017 and 12/31/2020 were grouped as MGTAC. Patient demographics, mechanism of injury, level of activation, operative intervention, intensive care unit (ICU) admission, length of stay, survival, and undertriage rates were reviewed. Chi square, ANOVA, and unpaired t-test were used for analysis to compare SAC and MGTAC patient outcomes.
Results
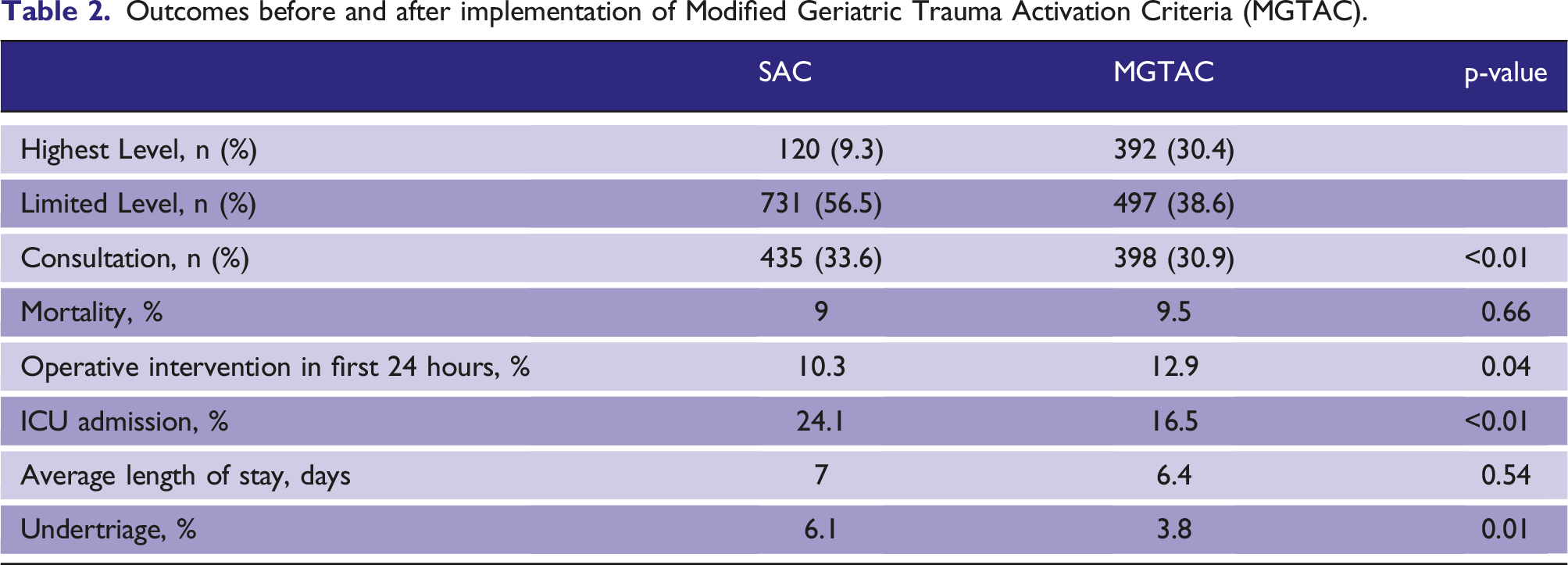
2582 patients were identified: 1293 (50.1%) in SAC and 1289 (49.9%) in MGTAC. Highest Level trauma activations for SAC vs. MGTAC were 9.3% vs. 30.4%, p < .01. Between SAC and MGTAC, ICU admission was 24.1% vs. 16.5%, p<0.01; operative intervention was 10.3% vs. 12.9%, p = .04; undertriage rates were 6.1% vs. 3.8%, p = .01; and average length of stay was 7 days for SAC vs. 6.4 days for MGTAC, p = .54. Overall mortality was 9% for SAC and 9.5% for MGTAC, p = .66.
Conclusion
Implementation of MGTAC did not improve geriatric trauma patient mortality. However, it decreased ICU admission and undertriage, and increased operative intervention during the first 24 hours.
Background
Individuals over 65 years of age made up approximately 22% of the population in the 2020 United States Census, and that percentage is only expected to grow annually. 1 Trauma is the 7th leading cause of death for those 65 years of age and over. 2 According to the National Trauma Data Bank, the proportion of trauma patients aged 65 years or over in level I and II trauma centers increased from 23% in 2003 to 30% in 2009. Moreover, geriatric patients triaged at non-designated trauma centers may not be properly reported, implying underestimation of true geriatric trauma patient prevalence.3,4
Specific to geriatric trauma patients, common mechanisms of injury including falls, motor vehicle collisions, and many low energy mechanisms lead to severe injuries. 5 Physiologic changes secondary to age-related compensatory adaptations of the musculoskeletal, cardiovascular, respiratory, and renal systems in the geriatric population lead to subsequent suboptimal responses to traumatic injuries. Frailty, medical comorbidities, and medication use alter baseline vital signs in this population.2,6–12 These factors increase the likelihood for undertriage, defined as failure to transfer patients to appropriate trauma centers, proportion of avoidable negative outcomes as a result of being denied access to high resource, and having major injuries but not triaged with inappropriate teams.13–15 Previous reports describe undertriage of geriatric trauma patients to be associated with a two-fold increase in the risk of death.16–20
Currently, there are no standardized guidelines for geriatric trauma activation. The American College of Surgeons Trauma Quality Improvement Program (ACS TQIP) recommends a lower threshold for trauma team activation for older trauma patients and this recommendation has led to the use of different geriatric trauma activation criteria at multiple tertiary centers.21,22 At our level 1 trauma center, we implemented a set of activation criteria specifically for geriatric patients. These trauma activation criteria were designated as the Modified Geriatric Trauma Activation Criteria (MGTAC).
To investigate the effects of MGTAC on geriatric trauma patients, our primary outcome was to determine the impact of MGTAC on patient survival; and secondary outcomes included the impact on undertriage rates and different interventions provided to patients before and after implementation of MGTAC. We hypothesized that MGTAC, which was based on the ACS TQIP Geriatric Trauma Management Guidelines, would improve patient outcomes. 21
Methods
Study design
The study is a retrospective, cohort investigation on prospectively collected data on trauma patients at a 720 bed, level 1 trauma center. The study protocol was approved by the Institutional Review Board and Institutional Scientific Review Committee. Approval for the protocol, entitled “Impact of modified geriatric trauma activation criteria at a level 1 Trauma Center on patient outcomes, a Retrospective Cohort Study” with reference number 1527985, was issued on October 23rd, 2020.
Selection criteria
From January 1st, 2014 to February 28th, 2017, trauma patients aged 65 and above were evaluated using the same set of trauma activation criteria as all other trauma patients when determining the level of activation. Patients were designated as either Highest Level or Limited Level dependent on mechanism of injury, anatomical injury or physiology (Figure 1). These procedures were designated Standard Activation Criteria (SAC). Trauma activation criteria implemented before and after March 1st 2017 at an academic, level 1 trauma center. Criteria for Highest Level trauma activations and Limited Level trauma activations for both Standard Activation Criteria (SAC) and Modified Geriatric Trauma Activation Criteria (MGTAC) are listed.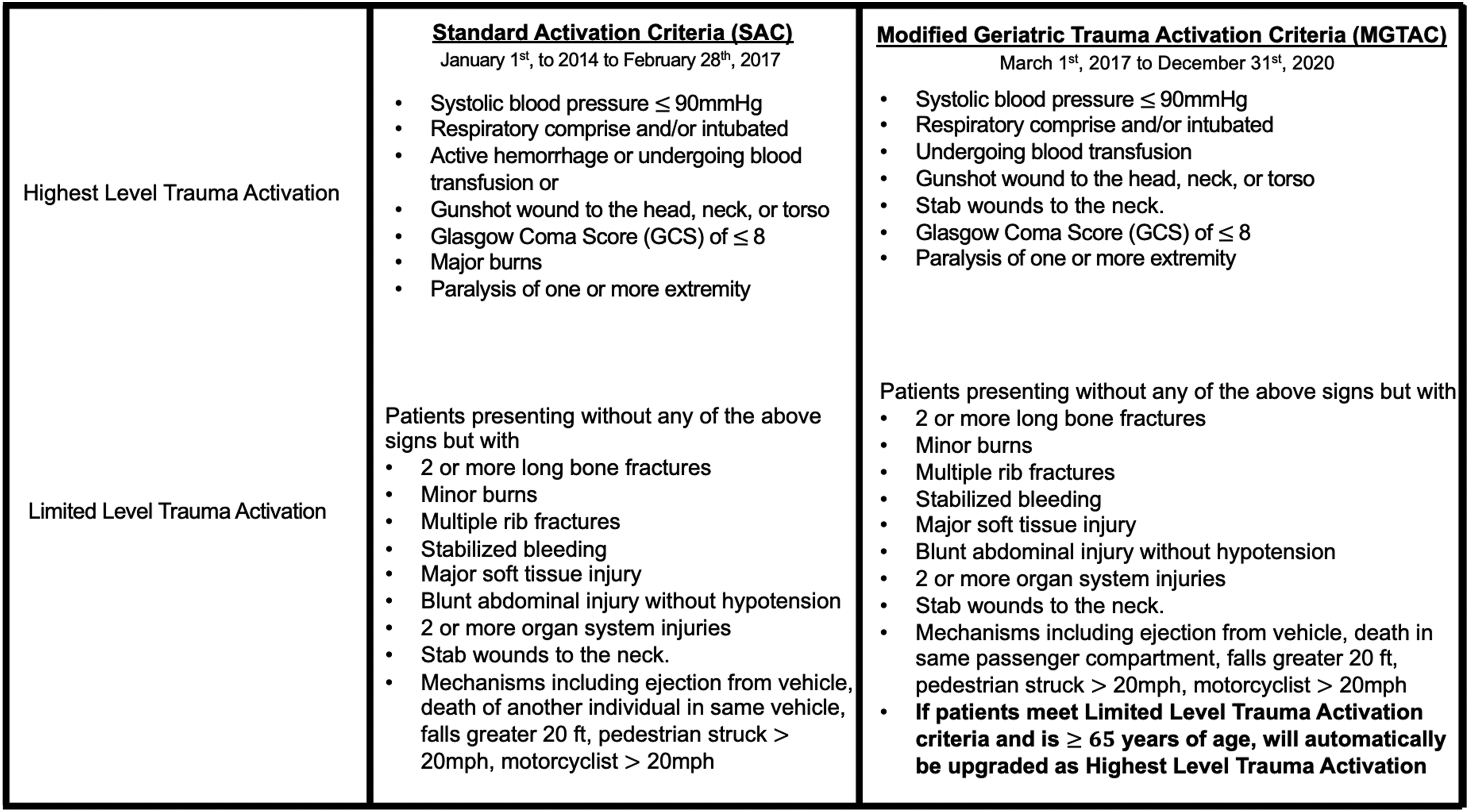
MGTAC were implemented on March 1st, 2017, where patients meeting the Limited Level trauma activation criteria and without prior work-up were rendered as Highest Level trauma activations if they were aged 65 and over. (Figure 1)
Highest Level activation and trauma consult designation requirements remained unchanged with MGTAC. The institution’s Trauma Registry, Trauma One, database was queried from January 1st, 2014 to December 31st, 2020. Eligible patients included adults 65 years and over seen as Highest Level trauma activation, Limited Level trauma activation, or as trauma consultations during the study period. Exclusion criteria include dead on arrival patients as defined by the American College of Surgeons Committee on Trauma (ACS COT), and patients with missing data.
Data Collection
Geriatric trauma patients presenting between January 1st, 2014 and February 28th, 2017 were categorized into the SAC group, and those presenting from March 1st, 2017 to December 31st, 2020 categorized into MGTAC group. Identifiers for eligible encounters were uploaded to a RedCap database, hosted by the institution’s Clinical and Translational Science Institute (Grant Number UL1TR001064) for abstraction from the electronic medical record. Records were randomly assigned to two co-investigators for abstraction. Variables collected included patient demographics, comorbidities, mechanism of injury, injury severity score (ISS), level of trauma activation, interventions provided, admission to intensive critical care (ICU), length of stay (LOS), survival, and undertriage rates. At our institution, we define undertriage using a triage assessment tool to review all trauma activations and compare triage decisions to patient outcomes. Specifically, we determined the number of Limited Level trauma activations and consultations that required high level resource utilization upon admission or those that resulted in early mortality.
Statistical analysis
All variables were checked for normality, completeness, and plausibility using frequencies for categorical variables and means for continuous variables. To compare patient characteristics and interventions provided, analysis of variance (ANOVA) was used for continuous variables and chi-square analysis was used for categorical variables. Unpaired t-test was used to compare LOS and ISS between groups, while chi-square and ANOVA were used to compare the frequency of level of activation, mortality, operative intervention provided, ICU admission, and undertriage. Statistical significance was set to alpha of 0.05. Data were analyzed using STATA 16 (StataCorp, College Station, TX). Continuous variables were reported using mean, standard deviation, and percentage. Categorical variables were reported using frequency and percentage.
Results
Characteristics of 2582 geriatric trauma patients under the Standard Activation Criteria (SAC) or Modified Geriatric Trauma Activation Criteria (MGTAC).
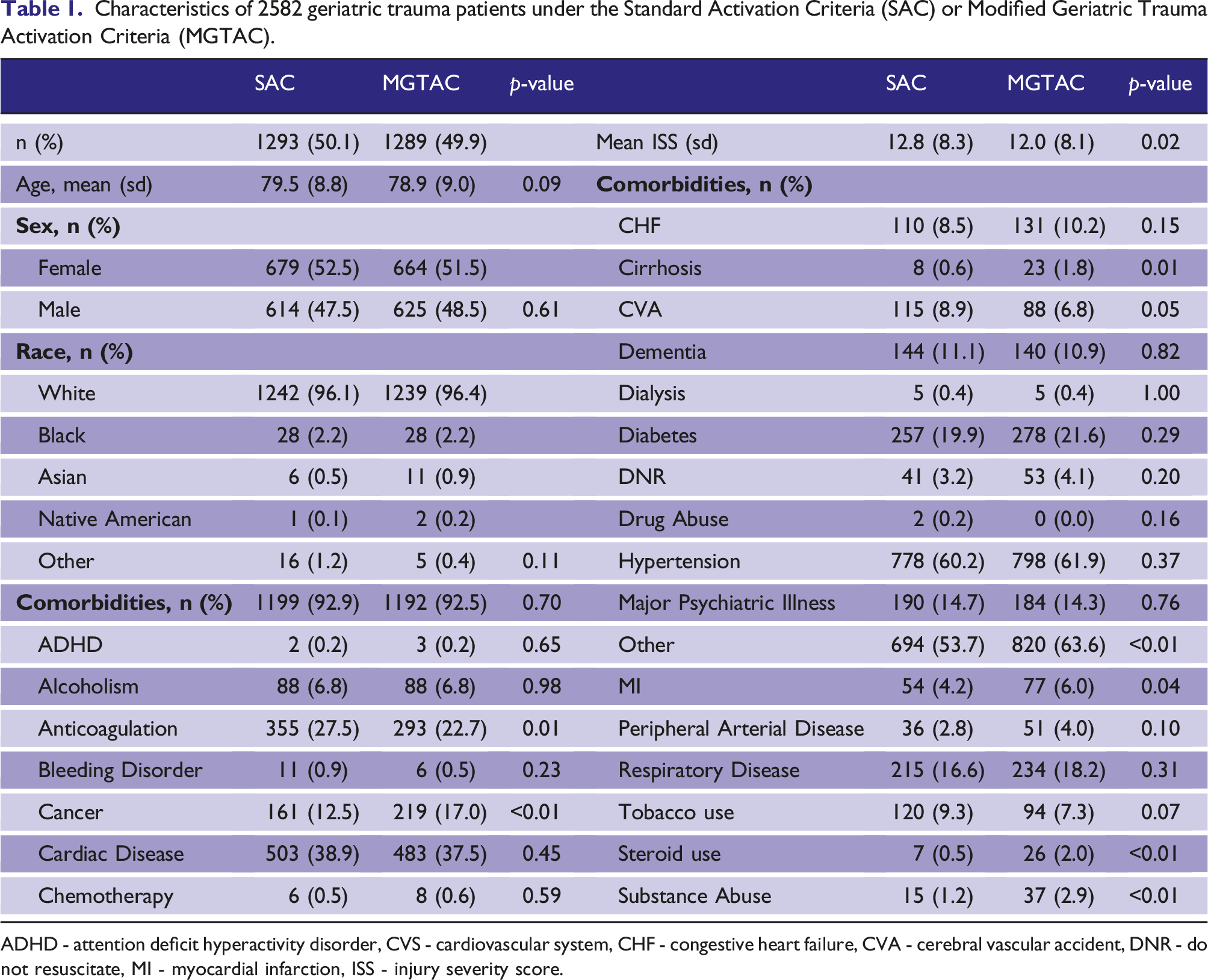
ADHD - attention deficit hyperactivity disorder, CVS - cardiovascular system, CHF - congestive heart failure, CVA - cerebral vascular accident, DNR - do not resuscitate, MI - myocardial infarction, ISS - injury severity score.
There were no differences between SAC and MGTAC for mechanisms of injury among blunt (98.6% vs. 97.8%), penetrating (0.5% vs. 1.3%), and others (0.9% vs. 0.9%); (p = .12). Comparing SAC vs. MGTAC, types of injury included motor vehicle crash (MVC) (16.4% vs. 17.3%), fall (76.3% vs. 75%), assault (1.4% vs. 1.4%), gunshot wound (GSW) (0.1% vs. 0.5%), burn (0.9% vs. 0.9%) and others (4.9% vs. 5%), and the differences between groups were not statistically different (p = .54). The rates of interventional radiology (IR) procedures (2.1% vs. 1.6%, p = .33), transfusion requirement (16.8% vs. 14.1%, p = .06) and multidisciplinary care with consultations to other specialties (84.5% vs. 86.7%, p = .11) did not differ between SAC and MGTAC.
Outcomes before and after implementation of Modified Geriatric Trauma Activation Criteria (MGTAC).
Discussion
There are limited data on the effects of trauma activation level on geriatric trauma patient outcomes, and currently, there are no standardized guidelines for geriatric trauma activation. Literature agrees however, that undertriage leads to increase mortality in this patient population.16,17,19 In conjunction with reports on geriatric trauma patients, ACS TQIP encourages a lower threshold for trauma team activation for older trauma patients; specifically, elevating the level of activation by one tier based on age.7,8,21,22 Based on these recommendations, we implemented a set of criteria by which trauma patients aged 65 and above, and fulfilling the Limited Level trauma activation criteria, be categorized as Highest Level trauma activation. We chose 65 years of age to describe a geriatric trauma patient based on definitions set by the Eastern Association for the Surgery of Trauma, as previous studies distinguish specific physiologic changes associated with this particular age and above. 4
At the initiation of MGTAC, any trauma patient aged 65 or above, and without any work-up, was designated as a Highest Level activation. Those who received prior work-up from a non-tertiary center hospital and was subsequently transferred to our institution were given a Limited Level activation. Clinical procedures were shaped to optimize MGTAC. Specifically, upon Highest Level trauma activation and patient presentation to the trauma bay, a notification would be sent through our the paging system, alerting over 280 pagers throughout the hospital. An operating room is immediately reserved, the on-call anesthesiologist is notified, and the surgical ICU charge nurse is alerted. Additionally, an x-ray technician is dispatched to the trauma bay, a room is reserved in the Computed Tomography suite, and laboratory technicians are requested to immediately process for possible massive transfusions and urgent laboratory examinations. The trauma attending is expected to respond in person within 15 minutes. In the situation where the trauma attending is not available, the back-up trauma attending is contacted. For Lower Level activations, a notification would be sent via the same paging system, but only to the trauma attending, trauma surgery resident team, and emergency department, requiring them to present to the trauma bay for patient evaluation. The operating room is also alerted but does not need to be made available. In these activations, the trauma surgeon has a six-hour window to physically assess the patient. There is no immediate dispatch to our blood bank. Lastly, trauma consultations require only an on-call trauma surgeon to assess the patient bedside, with additional resources acquired on an as-needed basis. The trauma surgery service, emergency department, and triage personnel communicating with emergency medical services underwent training to adopt MGTAC. There was ongoing monitoring of geriatric trauma triage and feedback to providers under the direction of the Trauma Performance Improvement group.
Our patient characteristics were comparable between the two groups in terms of age, gender, ethnicity, and overall comorbidities. The mechanism and type of injury remained similar with blunt injuries and falls assuming the highest rates, which is consistent with published data. 23 There was a statistical difference in ISS between the two groups, averaging 12.8 in SAC and 12.0 in MGTAC. While statistically different, the clinical difference between these values is minuscule since ISS is generally expressed in absolute values and grouped into three levels of severity. Our two patient populations would belong in the same severity level group (low severity).
Our outcomes were identified as the impact MGTAC generates on overall mortality, operative intervention within the first 24 hours of presentation, admission to the ICU, and undertriage rates. Mortality rates did not improve with MGTAC. These findings reveal that the decision to implement early aggressive interventions solely based on age does not address all the age-related physiologic derangements of geriatric trauma patients. MGTAC are therefore not sufficient to positively impact survival outcomes. Moreover, age by itself does not determine the overall clinical status of a geriatric trauma patient. To improve survival rates, a comprehensive assessment of the patient would be more appropriate. 9
More patients underwent operative interventions within the first 24 hours under MGTAC. We attribute this 2.6% increase in operative procedures to a correlation between Highest Level trauma activation and early aggressive interventions such as prompt provision of procedures. With any Highest Level activation, there is low threshold to proceed with operative intervention when patients present with hemodynamic instability after traumatic injuries. Consistent with the significant increase in Highest Level activations, operative intervention within initial 24 hours of presentation is likely to also increase as a result. However, a direct causation between Highest Level trauma activation and increased procedural intervention cannot be established in a retrospective review. Abiding by the ACS COT recommendation, interventional radiologists and IR intervention availability at all times are integral aspects of our trauma team. IR utilization rates are similar between groups and also consistent with other level 1 trauma centers.24,25 ICU admissions decreased following MGTAC. We speculate that escalating the level of activation yields aggressive early interventions in the trauma bay, with earlier stabilization of the patient’s physiology and therefore less need for ICU admission following initial triage.
Undertriage rates significantly decreased with MGTAC. This is inherent as the modified criteria were designed to decrease Limited Level trauma activations. Since our institution determines undertriage using an algorithm comparing the number of Limited Level trauma activations and consultations that results in high level resource utilization and/or early mortality, we factor the use of early high-volume blood transfusions, direct admission to the ICU, early interventional radiology procedures, early operative interventions, etc., into calculating undertriage.
The change in undertriage rates stems from the change in activation levels upon MGTAC. Highest Level trauma activations increased significantly after MGTAC, while Limited Level trauma activations decreased. This is expected as those who would have qualified as Limited Level trauma activations were ultimately categorized as Highest Level when presenting at or above age 65. The majority of Limited Level trauma activations during this period consisted of patients transferred from other institutions with completed diagnostic work-up and patients seen in the emergency department upgraded from trauma consultations to Limited Level activations. Understandably, consultation rates did not considerably change as MGTAC did not affect consults. As decreased proportion of patients were categorized as Limited Level activation, less patients were likely to be factored into undertriage calculations. From a clinical perspective, higher rates of Highest Level activation reduce chances of undertriage by providing early aggressive intervention.
To our knowledge, this is one of the largest studies to date looking at the impact of geriatric trauma activation criteria on outcomes of patients aged 65 or over. A study consisting of 2269 patients demonstrated a decrease in mortality and length of emergency department stay when trauma patients aged 70 and above were activated as Highest Level trauma activation. 8 Interestingly however, our study reveals contrasting results: mortality and LOS remained unchanged despite escalation of trauma activation criteria by a one tier based on patients’ age. A systematic review on benefits of early aggressive intervention for geriatric trauma patients, published approximately a decade ago, claims that such practice may benefit patients; however, specific outcomes were not described. 4 A more recent report states that a lower threshold for Highest Level trauma activation on geriatric trauma patients does not necessarily decrease mortality rates after the age of 65. While a lower threshold may benefit those with higher ISS and above 77 years of age, it generates significant concern for overtriage. 26 Another recent investigation demonstrated that age itself is not enough to designate the level of trauma activation and improve outcomes. 27 Comparing our results to published literature, we believe there is a trend towards reconsideration of the recommendation for a lower threshold for Highest Level trauma activations on geriatric trauma patients.
MGTAC forces increased Highest Level trauma activations and resource utilization without improvement in patient survival or hospital LOS. In the current environment, the impact on resource consumption, provider dissatisfaction, and cost of care are difficult to justify. Frequent Highest Level trauma activations also contribute to provider burnout. 28 To improve outcomes, we recommend a focus on factors benefitting geriatric patients in general, such as pre-injury strengthening and exercise programs. We stress a collaboration between geriatricians, palliative care specialists, and trauma surgeons as part of a multidisciplinary approach to geriatric trauma care, with emphasize on care for the whole person and early identification of futility.29–31
We have revised MGTAC in light of our results. The revised activation criteria consider age-related physiologic derangements. Specifically, patients aged 65 and over are activated as Highest Level trauma activation when they present with systolic blood pressure less than 100 mmHg and/or heart rate greater than 90 beats per minute, not when they simply meet the age criteria. Moving forward, we plan to assess patient outcomes using higher age brackets within older populations to further elucidate effects of physiologic changes and frailty associated with aging. While we focused on 65 and over, we suspect correlation between older patients and poorer outcomes.8,32 Additionally, our current analysis reveals differences in several comorbidities such as history of malignancy, cirrhosis, steroid use, and substance abuse between groups. With a descriptive analysis, it was difficult to understand how such factors may affect mortality rates. We plan to evaluate the effects of these comorbidities on trauma patient outcomes by collaborating with our geriatrician colleagues. Lastly, we will continue our work in exposing the financial impact of MGTAC. Preliminary data demonstrated increased cost of care within the first 48 hours of patient presentation with MGTAC.
We must also discuss the limitations of this study. It is a single institution investigation, so our results reflect the local institutional culture and may not be representative of other level 1 trauma centers. We did not employ the Cribari Method to assess undertriage rates. While our undertriage algorithm is a valid method, our findings on changes in undertriage rates may be institution specific. The criteria used to categorize Highest Level versus Limited Level activations are also institution specific and may not be representative of activation criteria used elsewhere.
We recognize there are factors contributing to geriatric patient outcomes that could not be described in our design. For instance, we also conducted a statistical analysis to assess outcomes using trauma activation level as the exposure rather than MGTAC. We found that patients activated as Highest Level presented with higher ISS, required more interventions, and had higher rates of death in first 24 hours. However, mechanism and type of injury between levels of activation were significantly different. Additional research is needed to rationalize these findings. MGTAC resulted in other unexpected outcomes that were not reviewed in this article. While we did not elaborate on the impact on cost of care, effect on provider burnout, and influence on institutional resource utilization, they remain important considerations.
Conclusion
Implementation of MGTAC at a level 1 trauma center resulted in change in trauma activation status and decreased undertriage. However, it did not affect geriatric patient mortality or hospital LOS. A shift towards emphasis on early multidisciplinary approaches in caring for geriatric trauma patients may potentially improve outcomes.
Footnotes
Acknowledgements
We would like to acknowledge AG our Trauma Registrar and NC our Research Coordinator.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was approved by Institutional Review Board and Institutional Scientific Review Committee. Approval for the protocol, entitled “Impact of modified geriatric trauma activation criteria at a Level 1 Trauma Center on patient outcomes, a Retrospective Cohort Study” with reference number 1527985, was issued on October 23rd, 2020.
Informed Consent
Informed consent was not sought for the present study because this was a retrospective study where no direct intervention was provided to patients.
Guarantor
* MS
Contributorship
RA and MS serve as the primary authors, involved with study design, protocol drafting and submission, data collection and interpretation, writing, and final revisions. APC served as the Research Epidemiologist who conducted data analysis and interpretation. SR, TK, KK, EW, GR, AP, EK contributed with data interpretation and drafting of manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript