
Abstract
Background:
We are facing an ageing population in Hong Kong. In response to the surge in service demand resulted from Silver Tsunami, a six-bed frailty unit was established in the Emergency Medicine Ward of Queen Elizabeth Hospital in December 2015. Frailty unit offers a bundle of multi-disciplinary approach for geriatric patients with an aim for early supported discharge.
Objective:
To evaluate whether this novel frailty care pathway, compared to the conventional general care pathway, would improve the outcome of the local elderly who were living alone.
Method:
This is a retrospective cohort study. Patients who were admitted from 1 September 2015 to 31 October 2017 were included in this study. Data were retrieved from the electronic patient record (ePR) of Hospital Authority. The outcome measurements are lengths of stay in acute and convalescent hospitals, transferral rate to a convalescent hospital and 28-day re-attendance rate.
Results:
A total of 190 patients were recruited (150 frailty vs 40 general). Baseline characteristics, including age, gender distribution, vital signs, laboratory results, use of mobility aids, Morse fall risk scale, Norton ulcer scale and Barthel Index were similar in both groups; except a higher diastolic blood pressure in novel frailty-care pathway. The length of stay in the acute hospital is significantly shortened (2.38 vs 3.27 days, p = 0.00018). The transferral rate to a convalescent hospital was less in frailty group (21.3% vs 42.5%, p = 0.00655). There was no significant difference in terms of total (7.10 vs 10.99 days, p = 0.09638) and convalescent (22.09 vs 18.16 days, p = 0.48183) length of stay between frailty group and general group, respectively; while the 28-day re-attendance rate was similar (26.7% vs 15.0%, p = 0.12589).
Conclusion:
This is a pilot study to first report a novel frailty-care model for the local geriatric population. It has shown a reduction in length of stay in acute hospital and transferral rate to convalescent hospitals, while introducing a non-significant reduction in total hospital stay, maintaining 28-day re-attendance rate and at an expense of a probable increase in the convalescent stay.
Background
When the Hospital Authority (HA) was established in December 1990, the median age of the population in Hong Kong was 31.6 years, and it rose to 43.4 years in 2016. The life expectancy at birth has increased from 74 and 79 years for men and women, respectively, to 81 and 87 years. 1 The number of people above 65 years was 490,500 in 1990, occupying 15.9% of the population; 2 and it has doubled to 1,117,300 and 15.9% when HA celebrated its silver jubilee. 3 In 2016, about one in six people will be aged over 65 years; 4 and it is anticipated that by 2044, it would be one in four. 5
Queen Elizabeth Hospital (QEH) was established in 1963 and has been the flagship hospital in Kowloon Central Cluster. Her catchment area includes Yau Tsim Mong, Kowloon City, To Kwa Wan, Hung Hum, Tsz Wan Shan, and Wong Tai Sin, with a total population of 1,174,500, of which 180,400 are above 65 years. 6
The Accident & Emergency (A&E) Department of QEH catered for 184,433 new case attendances in 2016/17. 7 In view of the growing demand, a six-bed frailty-care unit dedicated to the community-dwelling elderly was established in December 2015 within the Emergency Medicine Ward (EMW) of QEH. It is based on the British National Health Service (NHS) frailty model and is the first of its kind in Hong Kong.
Frailty-care unit aims at early identification and intervention of medical, functional and social problems of the patient and aims at early discharge or transferral to a convalescent hospital within 72 h of admission. Elderly patients who are previously having an independent activity of daily living, presented with acute deconditioning due to an acute illness (e.g. influenza, gastroenteritis and dizziness), increasing fall with balancing deficiency and required post-discharge community support service are our care targets. They will be assessed by EMW doctor and nurses for clinically indicated investigations and treatment care. A proactive and integrated referral would be made to a bundle of resources, such as pre-discharge service (PDS) nurse, physiotherapist, and occupational therapist on admission. They will be provided with mobility and cognitive training by physiotherapist and occupational therapist. Liaison with non-governmental organisation (NGO) services and community nursing services (CNS) will be conducted by PDS nurse.
Within 24 h of admission, a consultant or specialist in emergency medicine will conduct a daily assessment with a geriatrician, nurse case manager, physiotherapist and occupational therapist. Treatment care plan will be developed in a multi-disciplinary approach. The patient may be discharged home with various community support or transferred to convalescent hospitals for a short course of rehabilitation or temporary placement while arranging for a residential care home for the elderly (RCHE).
The frailty-care model, as a bridge between in-patient and community care, is to aim at an early supported discharge to reduce the length of in-patient stay in acute hospitals and avoid complications of prolonged hospitalisation. It is also to prevent unscheduled re-attendances and unnecessary hospital readmissions.
Literature review
An acute geriatric unit, or frailty unit, is characterised by patient-centred care, frequent medical review, early rehabilitation, early discharge planning and prepared environment. A frailty team is comprised of physicians, geriatricians, nurses, physiotherapists, occupational therapists, and social workers. Multi-disciplinary teams met regularly to plan patient care. 8 A meta-analysis found that frailty-care unit was associated with fewer falls, less delirium, less functional decline at discharge from baseline, shorter length of hospital stay, lower costs and more discharges to home. 9
In the United Kingdom, some hospitals operate dedicated ‘Frailty Units’ within the NHS. In the University Hospital of Leicester, patients who are 70 years or more who live at home with the presence of dementia or delirium, falls or a high Waterlow frailty score were admitted to such units for a comprehensive geriatric assessment (CGA). 10
A study on a 15-bed frailty unit involving 72 patients has shown that frailty-care model could result in shorter length of stay, lower 3-month mortality and a higher proportion of patients being discharged to their usual residence. 11
A prospective systems redesign study at a 1920-bed teaching hospital in the United Kingdom showed that a frailty unit can reduce bed occupancy and mortality without affecting readmission rates or requiring additional resources. 12 One randomised controlled trial in Sweden showed that the elderly who received a structured, systematic interdisciplinary CGA-based care at an acute elderly care unit were less likely to present with a functional decline after 3 months. The care in a CGA unit was also independently associated with lower mortality, at no higher cost. 13 A pre–post cohort study of the impact of embedding CGA within an A&E found that CGA is associated with a fall in readmission rate and acute ward admission rate, with an expense of a slight increase in in-patient day use and mean length of stay. 14
Previously, many frail older people who attend acute hospital settings and who are discharged home within short periods (up to 72 h) have poor outcomes. A systematic review was conducted by Conroy et al. to assess the role of CGA for such people. No clear evidence of benefit for CGA interventions in terms of mortality, readmissions, subsequent institutionalisation, functional ability, quality-of-life or cognition was demonstrated. However, they criticised that the five trials they included have an overall poor quality, and they called for further well-designed trials. 15
Lowthian et al. conducted another systematic review and meta-analysis, which compared community transition strategies with usual care and found no differences in terms of unplanned A&E re-attendance, hospital admission or mortality. They commented that there are limited high-quality data to guide confident recommendations. They also expressed the need for better design and evaluation to evaluate the efficacy and effectiveness of these innovative models of care. 16
Frailty-care model in QEH is the first novel care model for the elderly in Hong Kong. There is currently limited research study to guide our future care on the local ageing population. This study is conducted to assess the effectiveness of this care model in this locality.
Methods
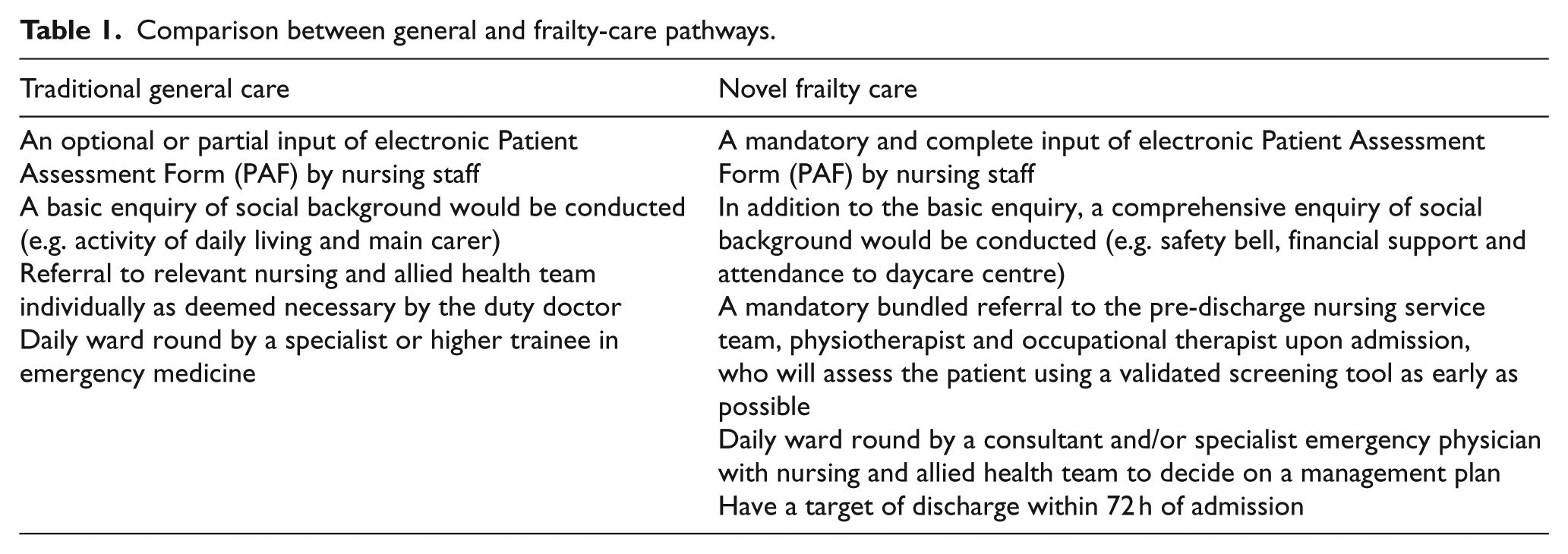
This was a retrospective, single-centre, parallel group cohort study to compare superiority of novel frailty-care model to conventional care model. The research was to focus on the community-dwelling elderly who were living alone, whether could a newly established multi-disciplinary approach frailty-care model led by an emergency physician, compared to existing care model, reduce the length of stay and re-attendance rate (Table 1). Research Ethics Committee (Kowloon Central/Kowloon East) had granted ethical approval for this research study on 25 October 2017 (Ref: KC/KE-17-0153/ER-2).
Comparison between general and frailty-care pathways.
A list of patients who were (1) 65 years or above; (2) living alone and (3) admitted to Emergency Medical Ward (EMW) through A&E of QEH from 1 September 2015 to 31 October 2017 were retrieved from Clinical Data Analysis and Reporting System (CDARS). Data collection was done by reviewing physical medical records in the medical records office and electronic records in Clinical Management System (CMS).
These patients were subjected to either one of the pathways on their attending doctor’s discretion – the general-care pathway and the novel ‘frailty’ care pathway. Their baseline characteristics, including gender, age, vital signs and laboratory investigations on admission, Mosby fall scale, Norton ulcer scale, Barthel Index and use of mobility aids were collected. Their discharge destination, length of stay in the acute and convalescent hospital and the 28-day re-attendance rate were measured.
Exclusion criteria to both novel frailty-care and conventional general-care pathways included sudden onset of unconsciousness, unstable vital signs, medical emergencies which cannot be managed in EMW setting, required mechanical ventilatory support, expected procedures within 24 h that cannot be safely performed in EMW or any clinical deteriorations that warrant transferral to acute ward as determined by the attending doctor in EMW. The analysis also excluded patients who had switched pathways after initial admission.
Continuous and dichotomous outcomes were analysed using a random-effects model to calculate weighted mean differences (WMDs) and risk ratios (RRs), respectively, with 95% confidence intervals (CIs). P < 0.05 was considered statistically significant for an overall effect. Analysis of variance (ANOVA) model was used to control for baseline characteristics. Student’s t-test was employed to detect differences in outcome.
Result
A total of 190 patients were recruited for the analysis, 150 were admitted to novel frailty-care pathway, and 40 were admitted to conventional general-care pathway. Women occupied 62.0% and 62.5% in frailty and general pathway, respectively. Their mean age was 82.1–83.5 years. No statistically significant differences were detected in vital signs, laboratory investigations, Morse fall scale, Norton ulcer scale, Barthel Index and walking mobility; except there was a higher difference in diastolic blood pressure in novel frailty-care pathway (79 vs 72 mmHg, p = 0.0150). The baseline characteristics were shown in Table 2.
Baseline characteristics of the study population (mean ± standard deviation).
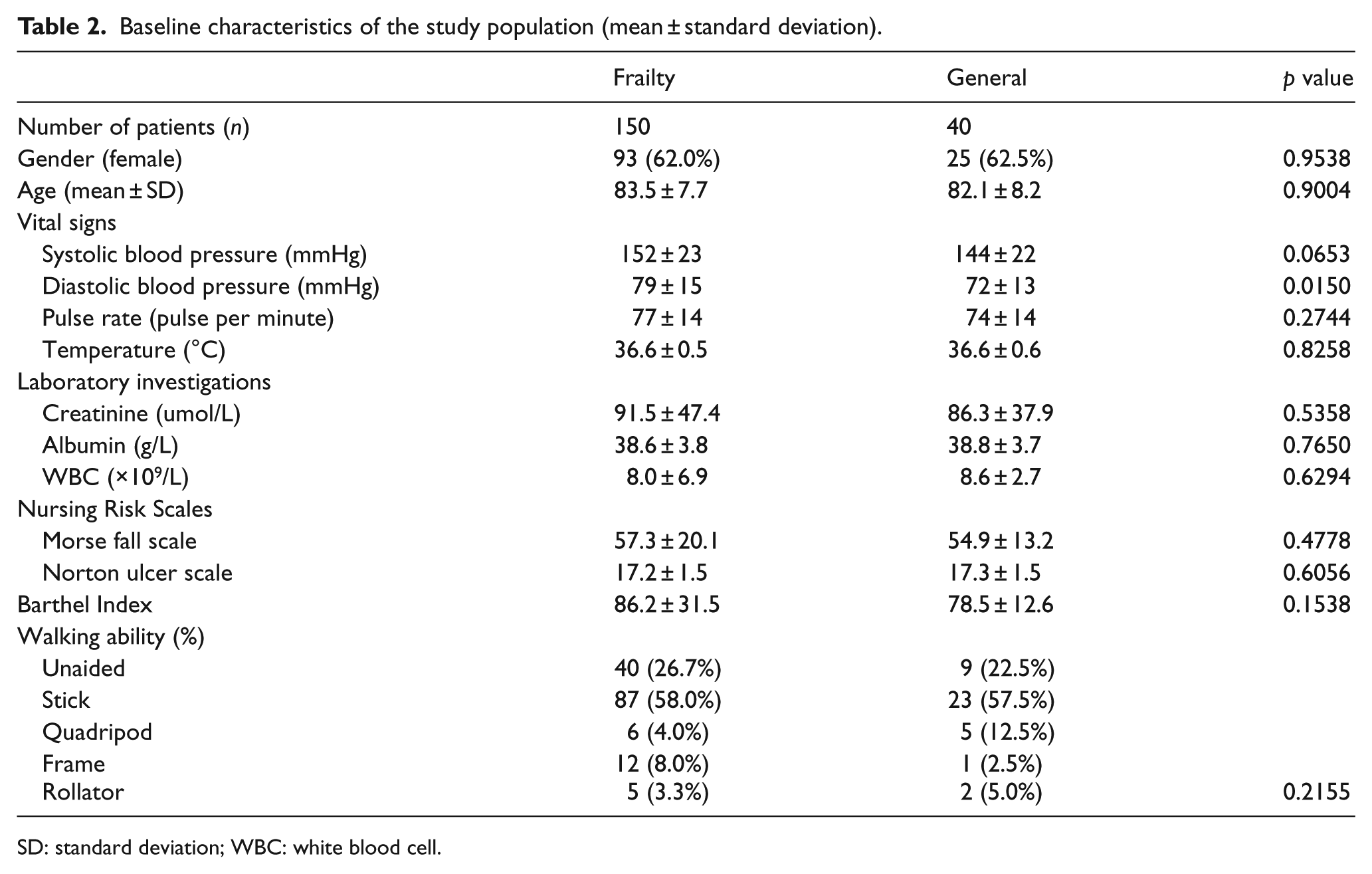
SD: standard deviation; WBC: white blood cell.
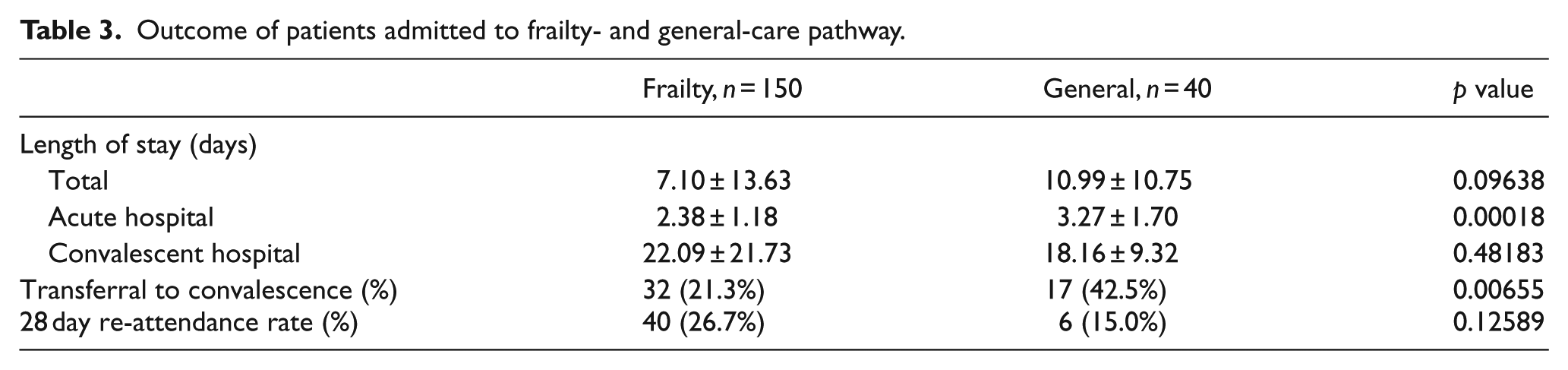
The length of stay in acute hospital was significantly shortened in the frailty group than in the general group (2.38 vs 3.27 days, p = 0.00018). There was no significant difference in the total length of stay (7.10 vs 10.99 days, p = 0.09638) and convalescent length of stay (22.09 vs 18.16 days, p = 0.48183) between frailty group and general group, respectively. The transferral rate to convalescent hospital was less in the frailty group (21.3% vs 42.5%, p = 0.00655), while the 28-day re-attendance rate was similar (26.7% vs 15.0% p = 0.12589). The results were shown in Table 3.
Outcome of patients admitted to frailty- and general-care pathway.
Discussion
The purpose of this retrospective cohort study was to evaluate whether this novel frailty-care pathway, compared to the conventional general-care pathway, would improve the outcome of the elderly who were living alone.
Modern medicine had utterly transformed our healthcare system and needs. However, as people age, they are more likely to live with complex comorbidities, disability and frailty. In people over 65 years of age, 28.3%, 21.0% and 11.6% had one, two and three kinds of chronic diseases, respectively; 17 the top three common chronic diseases were hypertension, diabetes and arthritis. 18 Elderly patients often present in a non-specific fashion or with frailty syndromes such as falls, delirium, immobility, incontinence and carer stress. 19
In Hong Kong, the primary care of the community-dwelling elderly is provided mainly by government general outpatient clinics (GOPC); and for those in RCHE, the service is provided by community geriatric assessment team (CGAT). In cases of acute deterioration which cannot be managed in the primary-care setting, these ill elders will be sent to Accident & Emergency departments (A&E) of the respective catchment areas. A&E will then provide initial management and decide on whether to admit or discharge the patient. Selected patients who are expected to require a short stay will be admitted to EMW.
Frailty care is a novel-care pathway in Hong Kong, with the first frailty unit established locally in QEH. Although studies in the United Kingdom has shown promising results, whether these advantages can be extrapolated to Hong Kong is still a question. This study was the first of its kind to assess the effectiveness of the first frailty-care model in this locality.
This study had shown that the novel frailty-care pathway can significantly reduce the mean length of stay in an acute hospital by 0.89 days. The total length of stay, inclusive of acute and convalescent in-patient care, was non-significantly reduced by 3.89 days. Although patients admitted through frailty-care pathway has 3.93 days longer convalescent stay, the transferral rate to convalescent hospitals was reduced by half. The 28-day re-attendance rate was not affected.
There were more patients recruited in the frailty-care group than in the general-care group. It could be due to a sampling bias from CDARS and attending doctors. On admission, nurses will enter the household members of the patient into the CMS, including whether the patient is living alone or not. This entry was mandatory for patients under frailty-care pathway but optional for patients under general-care pathway. Therefore, it was expected that when a list of patients who are living alone was retrieved from the CDARS, more patients from frailty-care pathway were recruited than the general group. Meanwhile, upon the establishment of frailty-care unit, attending doctors may tend to admit patients to the novel-care pathway than the general pathway. All these increased the sampling bias towards frailty-care group. Any future retrospective studies shall be designed as a pre- and post-implantation cohort and a full review of all paper medical records will be necessary in order to improve the recruitment rate for the general group.
The admission to either care pathways was neither randomised nor blinded and was solely dependent on the discretion of attending doctors. The retrospective nature of this study implied that data collection solely relied on the documentation by different staff. The data available might not be complete, and there might be inter-observer differences in assessing self-care, mobility and cognitive functions. This might hamper sufficient and accurate data analysis.
Because of the great heterogeneity of patients admitted to EMW, only patients who were living alone were included in this study. Therefore, the results may not be generalised to patients who are living with a spouse, domestic helper, or with other family members. Frailty-care unit aims not only to serve patients who are living alone but elders who have care need.
Future studies, particularly a prospectively designed cohort study, would be required to accurately assess the effectiveness of this novel frailty-care unit compared to the conventional general care pathway.
Conclusion
This is a pilot study to first report a novel frailty-care model for the geriatric population. It has shown a reduction in length of stay in acute hospital and transferral rate to convalescent hospitals, while introducing a non-significant reduction in total hospital stay, maintaining 28-day re-attendance rate and at an expense of a probable increase in the convalescent stay.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all staff members who dedicated their service to our emergency physician–led frailty unit, Queen Elizabeth Hospital. This is to confirm that all listed authors have (1) made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data, (2) drafted the article or revised it critically for important intellectual content, (3) approved the version to be published and (4)ach author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. The authors had full access to all the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data
The primary data generated during and/or analysed during this study, including but not limited to statistical data files, replication code, text files, audio files, images, videos, appendices and additional charts and graphs necessary to understand the original research are available from the corresponding author on reasonable request.
Informed consent and ethical approval
This study was approved by Research Ethics Committee (Kowloon Central/Kowloon East) of Hospital Authority on 25 October 2017 (reference no.: KC/KE-17-0153/ER-2). Written informed consent for publication was not necessary because no identifying patient data have been included in this manuscript. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. The name and date of approval granted by the ethical board are included in the manuscript.