
Abstract
As the population ages, the incidence of osteoporotic fractures, including those of the pelvis and acetabulum, continues to rise. Treatment of the elder patients with an acetabular fracture is much more controversial than the treatment of younger patients with similar injuries, where prevention of posttraumatic arthritis and total hip replacement remains optimal to limit need for revision arthroplasty. Arthroplasty for fractures of the proximal femur is commonplace in an older population and is a mainstay of treatment to promote early mobilization and weight-bearing. However, even with acute total hip arthroplasty for a geriatric acetabular fracture, most surgeons do not permit immediate weight-bearing postoperatively. Therefore, controversy regarding optimal treatment of these challenging fractures persists. Four treatment options have emerged: nonoperative treatment with early mobilization, open reduction and internal fixation (ORIF), limited open reduction and percutaneous screw fixation, and acute total hip arthroplasty. The exact indications and benefits of each treatment remain unknown. This article serves as a review of these four treatments and the data existing to support them.
Keywords
Introduction
As our population continues to age, the incidence of osteopenic fractures associated with low-energy falls continues to increase. 1 Acetabular fractures are no exception.2,3 From 1980 to 2007, a large prospective database of 1309 acetabular fractures demonstrated a 2.4-fold increase between the first and second halves of the study with 24% of acetabular fractures presented being those of elderly patients in the latter half of the study. 2 The mainstay of treatment for younger patients with acetabular fractures remains open reduction and internal fixation (ORIF) in an attempt to minimize the need for subsequent arthroplasty and the accompanied risks.4–6 However, elders with osteopenia and an acetabular fracture often present with many fracture characteristics that portend higher rates of posttraumatic arthritis, including dome impaction, marginal impaction of the posterior wall, comminution of the quadrilateral plate, and damage to the femoral head.2,7,8
The gold standard for treatment of displaced femoral neck fractures in the elderly is hemiarthroplasty or total hip arthroplasty 9 because of failure rates upward of 30% with surgical fixation. 10 In addition, the benefit of immediate weight-bearing after arthroplasty permits faster mobilization than restricted weight-bearing used after ORIF of the proximal femur. 9 Mortality rates after proximal femur fracture in the elderly may be as high as 36%, 11 with treatments now focused on early fixation to allow immediate mobilization and full weight-bearing. Several studies suggest that prompt surgical treatment less than 48 hours from injury can lessen postoperative complications and mortality.12,13
In contrast, mortality rates in geriatric patients with acetabular fractures appear to be lower than proximal femur fractures with rates between 8 and 16%,14–16 and many patients with displaced fractures who meet operative criteria can be mobilized without surgery and may achieve similar functional results to surgical treatments. 17
However, treatment decisions must be individualized to each patient, according to the treating surgeon's abilities. A 60-year old active male with a displaced acetabular fracture merits different treatment considerations than a demented 90-year-old male who is non-ambulatory with a similar injury. Regardless, acetabular fractures in the elderly are a difficult problem, and four treatments are commonly used in trauma centers around the world: ORIF, acute total hip arthroplasty, limited open reduction and percutaneous screw fixation, and early mobilization without surgery.
Nonoperative Treatment
Traction and Bed Rest
Little is known about the results of traction and bed rest for elderly acetabular fractures. However, the complications of prolonged bed rest in the elderly population are well known and potentially life threatening. Bed sores, venous thromboembolic disease, pneumonia, and loss of bone mass are known morbidities of bed rest for geriatric patients. 18
Spencer published results of conservative management of acetabular fractures in elderly patients in 1989. His retrospective reviews of 25 patients demonstrated unacceptable functional result in 30% of patients, where they were unable to return to their pre-injury level of activity. 19 The proportion of patients treated with traction was unclear in this study; however, poor results were associated with posterior column fractures, injury to the femoral head, delayed recognition of injury, early weight-bearing, and a period of traction less than 6 weeks.
A study from India reported 83% good to excellent functional results with heavy lateral greater trochanteric traction and distal femoral or proximal tibial longitudinal traction if the dome of the acetabulum could be reduced within 3 mm of anatomic position. 20 The duration of traction averages nearly eight weeks. However, the study population was young with an average age of 42 years and a maximum age of 66 years, making an extrapolation to geriatric patients impossible. Further, greater trochanteric traction pins have been notoriously unsuccessful as maintaining the pins in osteopenic bone is difficult over a long period of time. 21
Immediate Mobilization
There are no functional outcomes published for nonoperative treatment with early mobilization in elderly patients with acetabular fractures, although this treatment is used at several centers.14,16,22 Nondisplaced or minimally displaced fractures are typically treated with partial weight-bearing and early mobilization; 21 however, late displacement and ensuing poor functional results have been reported. 19
Ryan et al presented a series of 24 patients with displaced fractures who met operative criteria and were conservatively managed with early mobilization and no traction at the 2011 Annual Meeting of the Orthopaedic Trauma Association. They found similar WOMAC and SF-8 scores in a control group of patients managed with operative fixation at the same institution. 17 These data await peer-reviewed publication, and more studies with larger numbers of patients are needed to delineate the benefits and limitations of this treatment.
Intuitively, fractures associated with unstable posterior dislocations of the hip are not amenable to nonsurgical treatment and are usually indicated for ORIF with or without concurrent total hip arthroplasty.21,23–26
Case example (Fig. 1): A male in his 60s, status post (s/p) mechanical fall with right associated both-column acetabular fracture and secondary congruence. He was treated nonoperatively with early mobilization and touch-down weight-bearing to his right lower extremity after an examination under anesthesia with fluoroscopy that demonstrated no loss of secondary congruence with manual axial loading with hip flexion and internal and external rotations.

(
Open Reduction and Internal Fixation
ORIF remains the gold standard of treatment for physiologically young patients who can tolerate the anesthetic and surgical risks associated with approaches needed to reduce and stabilize the fractures.4–6 In older patients, two questions arise:
Will the surgeon be able to obtain and maintain a reduction? Can the elder patient tolerate the anesthesia and blood loss anticipated?
Older age and osteopenia are factors known to increase the risks of malreduction and posttraumatic osteoarthritis, and there is a need for subsequent total hip arthroplasty.2,4,5,7,8,22,27–29 Tile et al commented, “if the patient is elderly, has poor bone that is unlikely to hold a screw, has comminution, and is in a questionable medical state, open reduction would be folly.” 6
Miller et al evaluated reduction quality with plain radiographs and postoperative computed tomography scans in a group of 45 patients and found that computed tomography was superior at identifying malreduction. 8 They also reported no anatomical reductions in their series, even in an experienced surgeon's hands. A total of 51% of patients had fair reductions (1–3 mm residual displacement) and 49% had poor reductions (>3 mm residual displacement). No correlation was found between accuracy of reduction and functional outcome, and the authors believed that reduction criteria need not be as stringent as in younger patients. 8 Another single surgeon series of 810 acetabular fractures over 26 years also showed that older patients had lower rates of anatomical reductions than their younger counterparts. 29
It is not surprising that the rates of posttraumatic arthritis necessitating subsequent total hip arthroplasty increase with longer follow-up and are consistently near 30% in the series with the longest follow-up.7,22,27–30 Multiple studies have shown that poorer articular reductions are a risk factor for worse radiographic outcomes and conversion to total hip arthroplasty.7,22,29,30
Still, some believe that the restoration of bone stock makes subsequent conversion to arthroplasty easier and lessens the need for revision-style acetabular components or bone grafting.8,22
Risk factors for failure conversion to arthroplasty include increasing comminution and initial displacement,22,29 marginal impaction in the posterior acetabulum22,29,31 or anteromedial dome, 7 associated femoral head lesion,32,33 and associated femoral head or neck fracture,21,22,26 leading some to suggest acute total hip arthroplasty with ORIF when these are present.22–24,26,29
Fractures of the posterior column and posterior wall are treated with the standard Kocher-Langenbeck approach.4–6,22,27,28 No limited approach has been described, and expected blood loss is generally less than the anterior approach(es). Matta averaged 900 mL blood loss (range 100–3500 mL) with a Kocher-Langenbeck approach and 1366 mL (range 300–6000 mL) with an ilioinguinal approach. 5 Higher blood losses can pose greater risk to older patients with less physiologic reserve.34,35
The traditional anterior approach uses all three windows of the ilioinguinal approach, 4 and is the workhorse for associated both columns and anterior column with posterior hemitransverse fractures, the two most common patterns in older patients.2,8,16,22,36 The anterior intrapelvic, or Stoppa, approach has also been added as a fourth window. 37 The modified ilioinguinal approach combines all of these windows and allows the surgeon access to the true and false pelvis for fracture reduction and implant placement. 38
Recently, authors have described limiting the number of ilioinguinal windows used to limit operative time and possible decrease blood loss associated with the anterior approach. An isolated Stoppa window allows placement of an intrapelvic plate that counteracts forces that contribute to medialization of the hip joint often seen in older populations, 30 but does not provide access to the iliac wing. The limited ilioinguinal approach (lateral and middle windows only) was shown to decrease blood loss and operative time in fractures that did not have injuries to the medial superior ramus, pubic symphysis, or contralateral superior ramus requiring fixation without an increase in need for subsequent arthroplasty. 39 The lateral window of the ilioinguinal is sometimes used in isolation, but no published series exists and this technique is probably similar to the limited open approach used for reduction with percutaneous fixation.15,36,40
Case example (Fig. 2): A male in his 60s, s/p fall off from a bicycle with left anterior column posterior hemitransverse acetabular fracture. The patient elected for ORIF because of dome displacement and his young physiologic age; this was performed through an anterior intrapelvic approach (Stoppa) and the lateral window of the ilioinguinal approach. Intrapelvic and pelvic brim plates were used for stabilization.

(
Acute Total Hip Arthroplasty
Conversion from failed ORIF has proven difficult with longer operative times, greater blood loss and transfusion requirements, and higher rates of acetabular cup loosening.41–43 Acute total hip arthroplasty has been presented as an option to perform a definitive surgery at the time of injury and obviate the risk for development of posttraumatic arthritis of the hip.23,24,26,44 Indications include articular comminution, femoral head damage or impaction, femoral neck fracture, acetabular dome impaction, preexisting arthritis, and severe osteoporosis.22–24,26 Still, these are not equivalent to standard primary total hip arthroplasty as soft tissue trauma, bone loss, and acetabular discontinuity make successful reconstruction more difficult. These procedures often require more time and have estimated blood losses greater than 1000 mL in the only series to report it. 24 In addition, open reduction of the acetabulum is usually still required to provide a stable bony platform for placement of the acetabular component. Most surgeons appear to restrict weight-bearing for 6 −12 weeks.24,26,44 However, a recent single surgeon series reported no implant migration associated with immediate weight-bearing when a tantalum acetabular component was paired with a cemented femoral stem and plate stabilization of both columns of the acetabulum 45 in the treatment of low-energy osteoporotic acetabular fractures in older patients. The exact indications are unknown, but this should be considered when the treating surgeon does not believe that obtaining and maintaining an anatomic reduction is possible.
Case example (Fig. 3): A morbidly obese female in her 60s, s/p motor vehicle collision with displaced left transverse/posterior wall acetabular fracture. She also sustained a contralateral pilon fracture treated with ORIF. Decision for ORIF with total hip arthroplasty was made because of osteopenia, posterior comminution and chondrocancellous impaction, obesity, and the desire to avoid a delayed hip replacement through scarring associated with a Kocher-Langenbeck approach. Patient has no pain in her left hip or right ankle, and is ambulating without assistive devices at one year post injury.

(
Limited Open Reduction and Percutaneous Screw Fixation
Percutaneous fixation of acetabular fractures with or without limited open reduction techniques is technically demanding and required intimate knowledge of the osseous anatomy and its relation to fluoroscopy to safely place reduction instruments and screws.15,36,40 Regardless, a reduction of displaced fractures must be obtained prior to screw fixation. In situ stabilization of nondisplaced on minimally displaced fractures may limit later displacement that has previously been described, 19 but exact rates of displacement are unknown.
Benefits include average blood loss less than 100 mL and 0% infection rates in the largest series of 80 fractures. 15 Conversion to total hip arthroplasty was required in 30% of patients at an average of 6.8 years of follow-up, 36 similar to rates in the series of ORIF with the longest follow-up. 22 Patient-derived functional outcomes have also shown no differences when compared to patients treated with ORIF. 36 Other benefits include preserving the soft tissue envelope with minimal scarring for later arthroplasty surgery.
Limitations still exist. All published series about elder patients are from one center with more than 20 years of experience and specialized instrumentation that have developed over time. It is unknown if the techniques and their reported results can be generalized to other centers. Osseous corridors for screw fixation are also limited, and screw fixation will be inherently less stable than well-applied and well-positioned plates. In addition, an unstable posterior wall, whether in isolation or associated with an associated fracture pattern is a contraindication to this technique. 15
Case example (Fig. 4): A male in his 60s with history of colon cancer s/p MVC with displaced left associated both columns acetabular fracture. Patient also had a history of colon cancer s/p colectomy with left upper quadrant colostomy and atrial fibrillation on Pradaxa. The patient chose limited open reduction and percutaneous screw fixation because of colostomy and risk of bleeding with Pradaxa. The patient has healed his acetabular fracture and walks two miles per day with no symptoms of pain or limitations in his left hip.

(
Mortality
Little attention has been paid to mortality associated with geriatric acetabular injuries until recently. Two recent studies have shown one-year mortality rates between 8% and 16%,14,16 significantly less than rates for the proximal femur. 11 Patients with isolated acetabular fractures have been shown to have lower mortality rates than polytraumatized elders who have an acetabular fracture as part of their injury. 14 Many factors play into the surgical decision-making for these patients, and it appears that patients with more medical comorbidities are more likely to be treated nonoperatively. 16 Once medical comorbidities are accounted for, there appears to be neither mortality benefit nor detriment, between nonoperative treatment with early mobilization, ORIF, limited open reduction with percutaneous screw fixation, or acute total hip arthroplasty.
Conclusions
Nonoperative treatment with early mobilization, ORIF, limited open reduction with percutaneous screw fixation, and acute total hip arthroplasty all appear to be viable treatment options for various acetabular fracture patterns seen in geriatric patients. It appears that no treatments have an impact on one-year mortality. Detailed algorithms are difficult to develop because of variations in surgeon experience, expertise and training with surgical fixation, and/or arthroplasty. My current treatment algorithm is shown in Figure 5. Regardless, a treatment plan must be individualized based upon patient factors, fracture factors, and the treating surgeon's abilities.
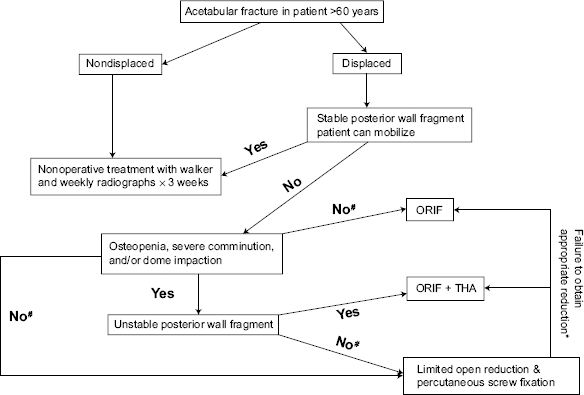
Treatment algorithm for elderly acetabular fractures.
Author Contributions
Conceived and designed the experiments: JLG. Analyzed the data: JLG. Wrote the first draft of the manuscript: JLG. Contributed to the writing of the manuscript: JLG. Agree with manuscript results and conclusions: JLG. Jointly developed the structure and arguments for the paper: JLG. Made critical revisions and approved final version: JLG. The author reviewed and approved of the final manuscript.