
Abstract
Introduction:
The psychomotor skill of cardiopulmonary resuscitation emphasized the importance of high-quality chest compression. This investigation examined the effect of self-debriefing and the different materials of debriefing during hands-on cardiopulmonary resuscitation practice for healthcare providers.
Methods:
This was a randomized controlled trial of a cardiopulmonary resuscitation training program involving emergency medical technicians in northern Taiwan. Participants were blinded to the study purpose and were allocated randomly using the black envelope method. All participants completed a 2-min pre-test of hands-only cardiopulmonary resuscitation using a manikin. Those who were allocated to the control group received self-debriefing with knowledge of pre-test result. Those who were allocated to the experimental group received self-debriefing with an additional biomechanical information of performance of chest compression. A post-test was performed 30 min after the pre-test.
Results:
A total of 88 participants were enrolled with 44 in each group. There was significant difference of cardiopulmonary resuscitation quality after self-debriefing among all participants (pre- vs post-test adequate rate, 54.7% vs 67.5%, p = 0.028; adequate depth, 41.2% vs 69.5%, p < 0.001; full recoil, 35.9% vs 54.5%, p = 0.001). The analysis of effects of self-debriefing with additional knowledge of performance revealed no significant difference in any of the measurements (improvement in adequate rate, 11.3% vs 14.2%, p = 0.767; adequate depth, 29.6% vs 27.0%, p = 0.784; full recoil, 23.0% vs 14.1%, p = 0.275).
Conclusion:
Self-debriefing improved hands-only cardiopulmonary resuscitation quality whether or not biomechanical information of performance of chest compression was given.
Introduction
Resuscitation plays an important role in emergency medical services. 1 Psychomotor skills are important in achieving high-quality chest compressions.2,3 High-quality chest compressions are those done at a rate of 100 compressions per minute,4,5 with a depth of 5 cm,6,7 with full chest recoil with each compression,8,9 and with minimal interruptions.10,11 Studies have shown that debriefing improves cardiopulmonary resuscitation (CPR) quality.12,13 However, CPR skills decay rapidly at 3–12 months after training.14,15 Thus, frequent refresher courses are required. To address this need, self-instructed CPR training has been proposed, which has greater convenience and a lower cost. 16 Based on previous reports, the effectiveness of self-instructed CPR training is promising.16,17
By focusing on motor skill learning, information provided during debriefing can improve understanding of results and performance (e.g. in terms of movement and posture).18–20 Traditional instructor-led CPR training includes biomechanics-related debriefing to improve understanding of movement. Biomechanical debriefing is concerned with the performer’s posture, which should involve taking a kneeling position close to the patient’s side, leaning forward and pressing with the weight of the upper body, with the arms perpendicular to the palms, and keeping the elbows straight to transmit force during chest compressions. Those who are unable to attain full recoil are instructed to avoid excess leaning. In contrast, the structured debriefings described in previous reports were based on the transcripts of actual CPR procedures, in accordance with resuscitation training guidelines.12,13 To facilitate self-instructed CPR training for healthcare providers, the effects of different debriefing components should be explored. This investigation explored the effects of different types of self-debriefing for hands-only CPR training; the debriefings focused on results and performance. We hypothesized that self-debriefing focusing on performance may improve the efficacy of CPR training.
Methods
Study design and setting
This study was a randomized controlled trial of a CPR training program for emergency medical technicians (EMT) in northern Taiwan. The study was conducted at the fire departments of Taoyuan and Hsinchu County in July 2014 and August 2014, respectively. The study was approved by the ethics committee of Chang Gung Memorial Hospital, Linkou, Taiwan. Informed consent was obtained from each participant.
Randomization and group allocation
Figure 1 provides a flow chart of the study design. Participants received no information regarding the study prior to the test. All participants were allocated to groups randomly using sealed black envelopes. All participants completed a 2-min hands-only CPR pre-test using a manikin (Resusci Anne QCPR; Laerdal Medical Corp., Wappinger Falls, NY, USA) after the study assistants had recorded the participants’ characteristics using a standardized form. Participants allocated to the control group (self-debriefing with test results provided) received transcripts of their pre-test results (computer records generated by the manikin pertaining to hand position, depth of compressions, rate of compression, full recoil, and hands-on time; all in terms of % correct). A printout of current CPR guidelines was also generated. Participants who were allocated to the experimental group (self-debriefing with test and performance results provided) received an additional printout of biomechanical information for chest compression (with figures) as follows:
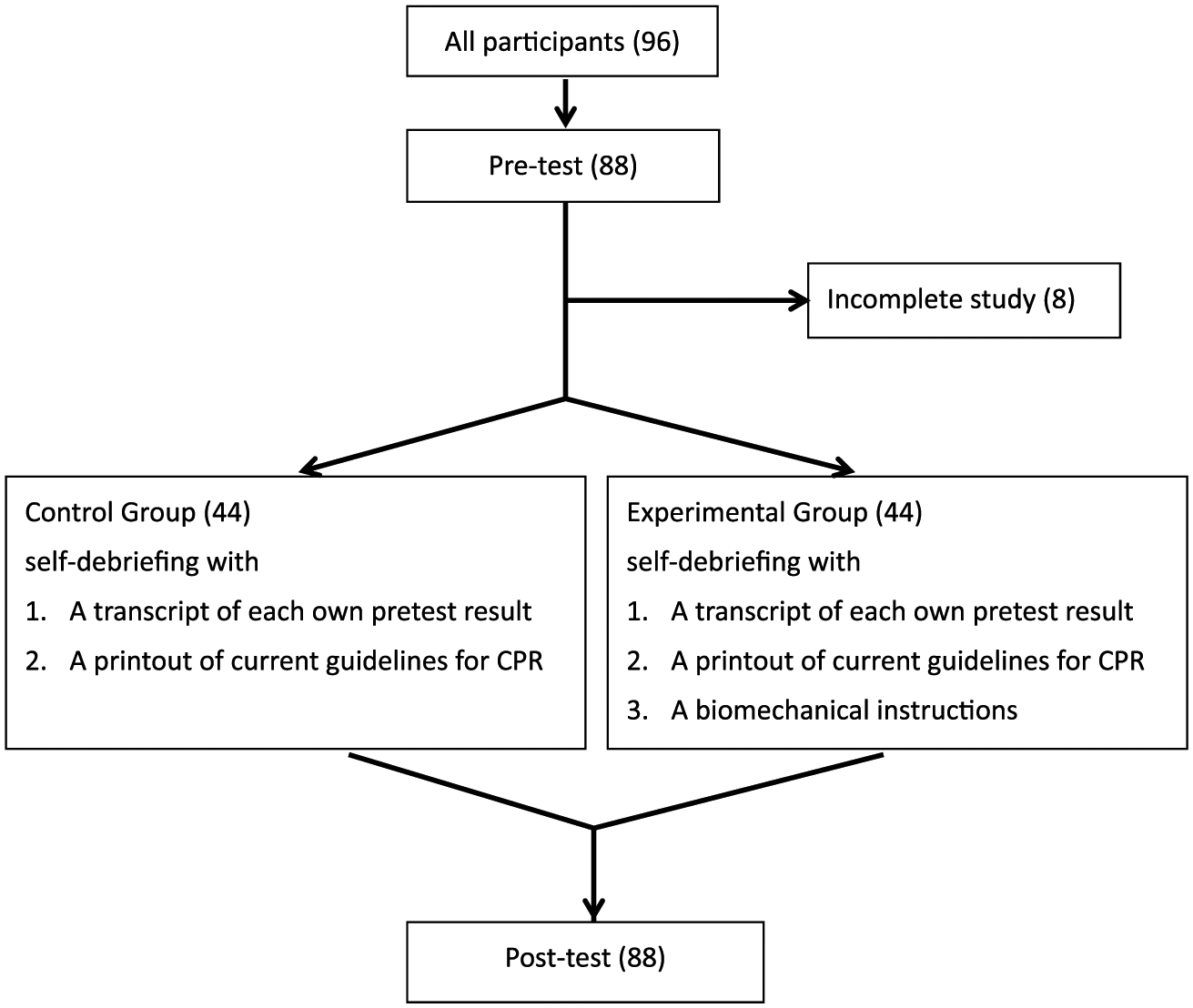
Study design and flow chart.
For those who did not achieve adequate depth during the pre-test, please
1. Assume a kneeling position close to the patient’s side;
2. Lean forward and press with the weight of the upper body;
3. Keep the arms perpendicular to the palms, with the elbows straight to transmit force during chest compressions.
For those who did not attain full recoil, please
4. Keep your head up and back straight without bending over, hunching, or looking down.
Participants were asked not to discuss the content of the self-debriefing during the study period. A post-test including a further 2 min of hands-only CPR, performed using the same manikin, was done 30 min after the pre-test.
Participant selection
The enrolled EMTs were board-certified in Taiwan and classified as EMT-1 (EMT-basic in the United States), EMT-2 (EMT-intermediate in the United States), or EMT-Paramedic (EMT-P in the United States). EMT-1, EMT-2, and EMT-P personnel receive 40, 280, and 1280 h of training, respectively, before certification, as well as additional tuition (for 24, 72, and 96 h, respectively) every 3 years. Board-certificated EMT-1s enrolled on the 45th EMT-2 training course held in Taiwan, at the fire department of Taoyuan County. EMTs from six fire stations nearby to the central fire department of Hsinchu County, Taiwan, participated in this study. EMTs who were unwilling to participate, did not provide written informed consent, lost to follow-up, or had incomplete data were excluded.
Study protocol and data collection
Two study assistants collected the data using a standardized form. The participant characteristics recorded included sex, age, and whether a CPR training course had been completed in the past 3–12 months. Components related to the quality of CPR, including the use of the correct hand position, adequate compression depth (i.e. a depth of at least 5 cm), adequate compression rate (i.e. a rate of 100–120 compressions per minute), full recoil, and hands-on time (all in terms of % correct ) were the focus of a practice session. In addition, the “kneeling distance” (i.e. distance from the manikin to the kneeling pad) during CPR was recorded by a study assistant using a tape measure. A Likert-type scale, applied previously to evaluate exertion-related attitudes, was used to evaluate the perceived difficulty of the CPR for all participants (recorded after pre- and post-tests). The response options on the scale were as follows: (1) very difficult, (2) difficult, (3) neutral, (4) easy, and (5) very easy.21,22 Injuries relating to CPR performance were followed-up by telephone after 1 week, with the injured body part recorded (arm, shoulder, back, waist, leg, or other), as well as whether the injury affected daily activities ((1) no effect, (2) minor effect, (3) neutral, (4) moderate effect, and (5) major effect). For a true difference in the extent of improvement in CPR quality (± standard deviation (SD)) between groups (i.e. an improvement of at least 10%), 76 subjects (n = 38 per group) were required with a power of 0.99 and type I error of 0.05.
Primary data analysis
The primary outcome was extent of improvement in CPR, before versus after self-debriefing. Improvement was indexed by adequate depth and rate of compressions, and achievement of full recoil (all in terms of % correct). The secondary outcomes were any difficulties in performing CPR after the tests, and any CPR-related injuries (recorded at 1-week follow-up). The data were analyzed using SPSS for Windows software (version 13.0; SPSS Inc., Chicago, IL, USA). Categorical variables are presented as numbers and percentages and were compared using the chi-square or Fisher’s exact test, as appropriate. Continuous variables are presented as means and SD. Student’s t-test was used to assess continuous variables. In all analyses, a p-value less than 0.05 was considered statistical significant.
Results
The trial enrolled 96 EMTs. Eight were excluded due to incomplete test records or loss to follow-up. Table 1 shows the baseline characteristics of the 88 participants. In total, 63.6%, 30.7%, and 5.7% of the participants were board-certified EMT-1s, EMT-2s, and EMT-Ps, respectively. Over 90% of the participants were male. On average, participants had completed 1.7 and 4.3 CPR training courses over the previous 3–12 months, respectively. There was a significant difference in CPR quality (before vs after self-debriefing) across all participants (pre- vs post-test adequate rate of compression, 54.7% vs 67.5%, p = 0.028; adequate depth of compressions, 41.2% vs 69.5%, p < 0.001; and full recoil, 35.9% vs 54.5%, p = 0.001) (Table 2). Self-rated CPR difficulty was significantly different between the pre- and post-test (mean Likert-type scale scores = 2.0 and 2.4, respectively; p < 0.001). No injuries related to performance of CPR were reported at the 1-week follow-up, and thus daily activities were not affected in any participant.
Baseline characteristics of participants.
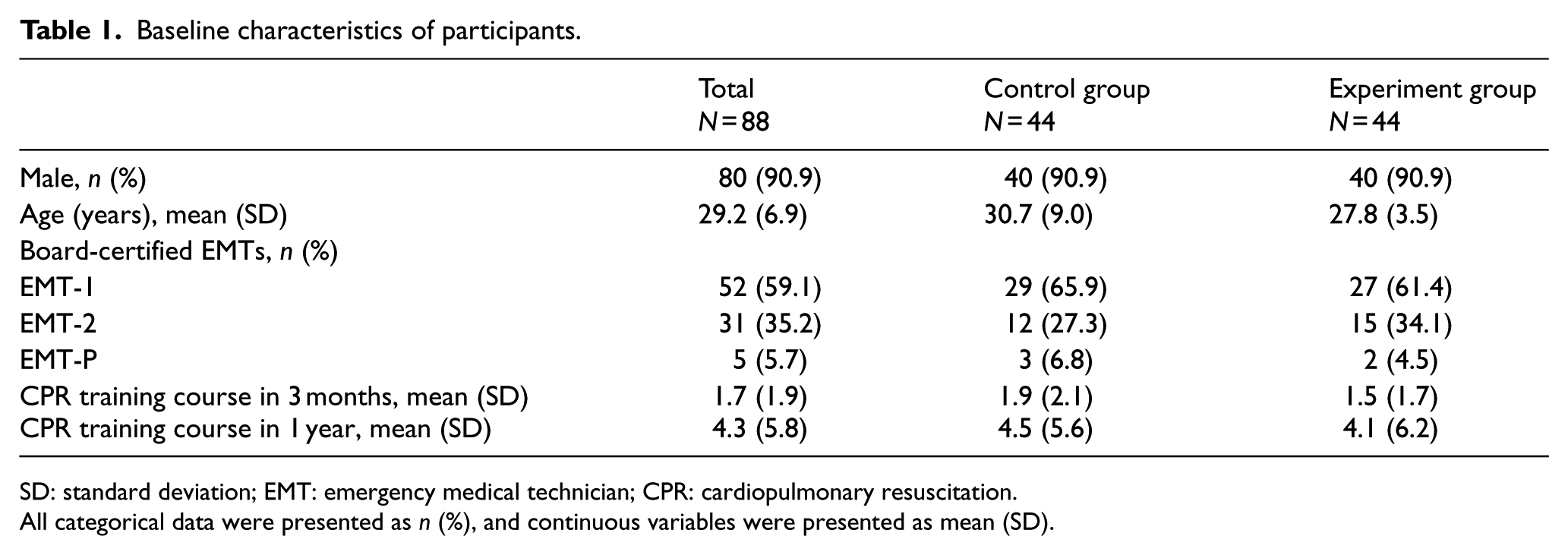
SD: standard deviation; EMT: emergency medical technician; CPR: cardiopulmonary resuscitation.
All categorical data were presented as n (%), and continuous variables were presented as mean (SD).
CPR quality before and after self-debriefing.
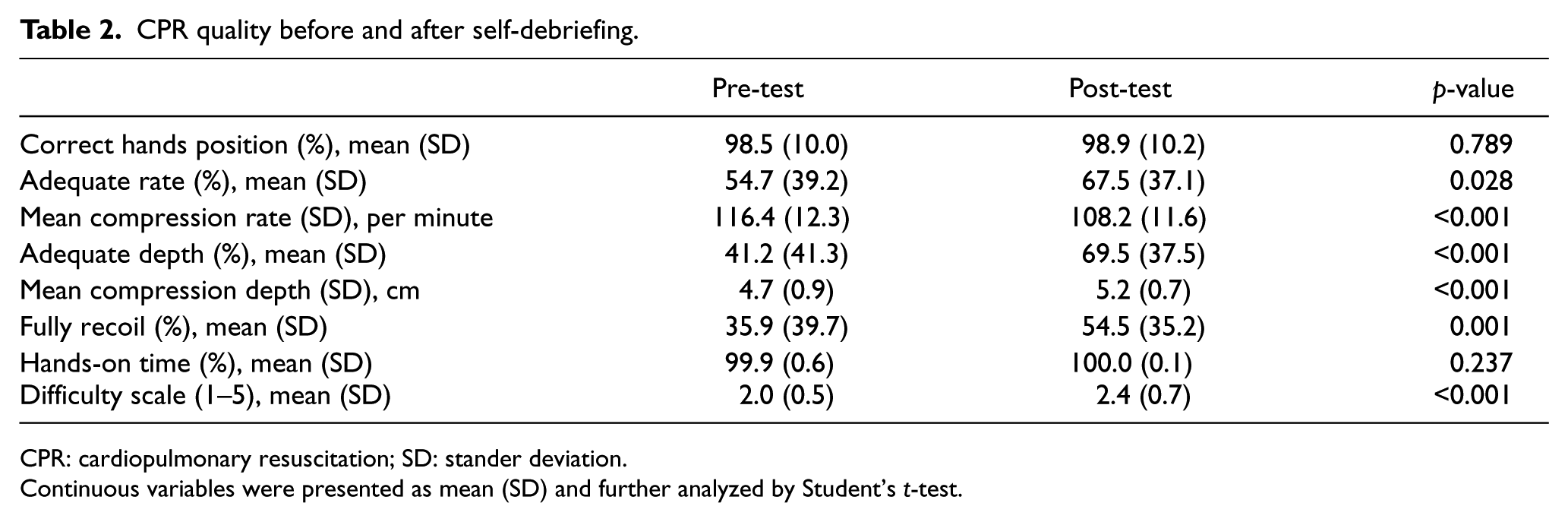
CPR: cardiopulmonary resuscitation; SD: stander deviation.
Continuous variables were presented as mean (SD) and further analyzed by Student’s t-test.
The difference between providing versus not providing biomechanical information during the self-debriefing was insignificant for any of the CPR quality indices (Table 3). There was a difference in kneeling distance from the manikin, as measured at the post-test, between the control and experimental groups (mean distance = 4.2 vs 2.2 cm, p = 0.013). Self-reported difficulty of CPR, measured pre- and post-test, did not differ significantly between the control and the experimental groups (pre-test = 2.0 vs 2.0, p = 0.878; post-test = 2.4 vs 2.4, p = 0.843).
Subgroup analysis: comparing the improvement of performance of self-debriefing with/without biomechanical instructions.
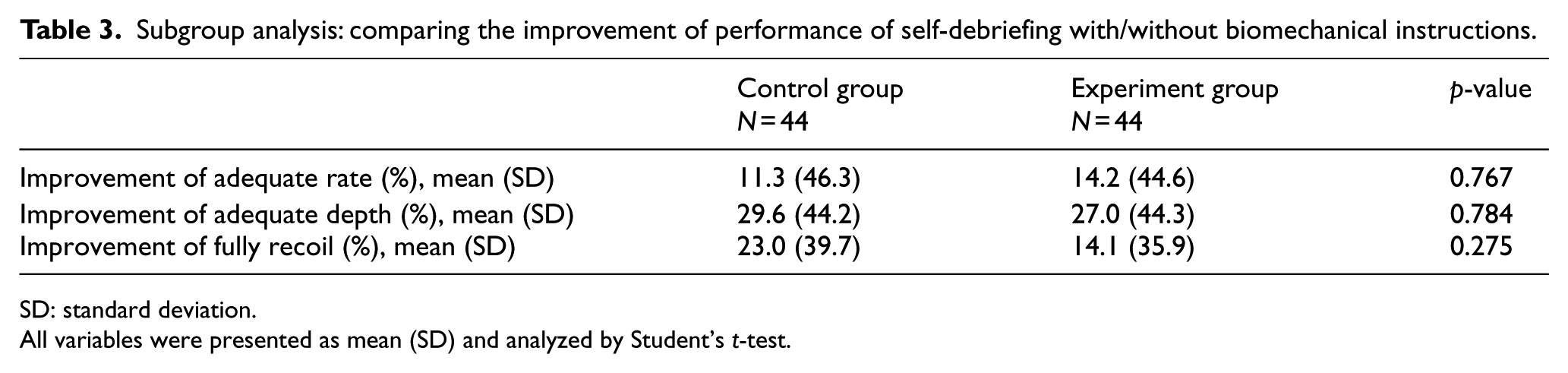
SD: standard deviation.
All variables were presented as mean (SD) and analyzed by Student’s t-test.
Discussion
This study was a simulation-based, randomized controlled trial that examined the effect of self-debriefing on the performance of experienced healthcare providers. The results showed a significant improvement in CPR quality after self-debriefing. There was no difference in the quality of chest compressions after self-debriefing with versus without biomechanical information given. Furthermore, there was no difference between the control and the experiment groups in the self-reported difficulty of performing CPR, or in the rate of CPR-related injuries, at the 1-week follow-up.
Based on the results, several issues should be discussed. First, this study supports previous studies in showing a significant improvement in chest compression quality after self-debriefing with CPR test results. Edelson et al. 12 showed that automated feedback improved CPR quality in a “before-and-after” cohort study. In a prospective, randomized, simulation-based study comparing the effects of audiovisual feedback and debriefing, Dine et al. 13 reported that performance was best using a combination of the two. The debriefings used in these two studies included the participants’ test results, transcripts of CPR quality downloaded directly from defibrillators or manikins, and counseling methods to comply with the guidelines.12,13 Our results showed no difference in the extent of improvement in CPR quality with or without provision of biomechanical information on compression performance. Feedback including information on the outcomes or quality of CPR performance may affect learning according to common principles. 20 Improvements in CPR quality through provision of information on test performance may be limited. Previous studies showed enhancement of motor skills by practicing a sport with an “external focus” (focus on the movement effect) compared to an “internal focus” (focus on movement), for golf, darts, and basketball.23–25 Instructions that directed the focus of attention to an implement, rather than to the participant’s own body, increased the accuracy of movements. 26 Wulf et al. 27 introduced the constrained action hypothesis, which posits that an internal focus of attention may interfere with automatic control processes in a dynamic balance task. In contrast, an external focus of attention facilitates automaticity. This was consistent with our results pertaining to the motor performance of healthcare professionals during CPR training.
Our results could be explained by reference to the study sample. The participants were experienced healthcare providers, that is, board-certified EMTs who had frequently received CPR training. Thus, they may have been familiar with the training drills, such that they could adjust their performance according to the pre-test results without employing a specific biomechanical method or changing posture. Chi et al. 28 performed a motion analysis study to explore the association between CPR quality and posture type, which included kneeling on the floor and being positioned adjacent to 37- and 63-cm-high tables. They found that CPR quality was high and similar across postures, although more experienced healthcare providers showed a significant difference in CPR kinematics. The authors concluded that no additional training on posture was required for experienced healthcare providers. This study did not perform a motion analysis and thus could not measure changes in posture and movement after self-debriefing definitively. The kneeling distance from the manikin during the pre-test was the only predictor of positional changes. Although the kneeling distance from the manikin was significantly shorter in the post- versus pre-test across all participants, in real terms, the difference was small, at only 2.0 cm. The effect on CPR quality of such a small difference in distance may be limited. This was supported by our study, where no difference in self-reported difficulty of CPR before versus after the self-debriefing was observed, and there were no injuries related to CPR reported at the 1-week follow-up. The majority of the participants rated the difficulty of performing CPR as neutral or easy. In a study that analyzed 205 questionnaires completed by healthcare providers working at three general hospitals and 20 nursing homes, 90% of the respondents reported discomfort during and after performing CPR. 29 Tsou et al. 30 measured the electromyographic activity of healthy experienced CPR practitioners for 5 min. They found that the erector spinae was one of three muscles showing marked activity during performance of chest compressions; in our study, the test involved 2 min of chest compressions, which is shorter than that in the previous report. 30 Our participants were all EMTs, who are likely to be capable of performing CPR without difficulty for 2 min. Although tests involving prolonged CPR may reveal differences between groups, such tests do not reflect daily practice or consensus resuscitation guidelines, which suggest switching compressors every 2 min, or after five cycles of compressions where possible.
Limitations
This study should be interpreted in the context of the following limitations. First, it was conducted in two county-based fire departments with small numbers of EMTs, which may limit the general applicability of the findings. The effects of the self-debriefing including information on test performance on lay rescuers warrant further investigation with a larger sample. Second, the duration of the test was only 2 min, which may be too short to reveal a difference between groups. As mentioned previously, use of a longer CPR test may reveal differences between groups, and any such differences could be too small to have clinical significance and thus may not reflect daily practice. Third, this study did not compare the degree of retention of CPR skills between groups at follow-up. Therefore, whether there was any difference in skill retention between the groups remains unclear. Fourth, the study was performed in July and August 2014, which complied with the American Heart Association 2010 guidelines. Therefore, our results may not comply with the 2015 guidelines, where the compression rate has increased from 100 to 120 per minute. 31
Conclusion
This study showed a significant improvement in CPR quality after self-debriefing including the test results, following a manikin-based training program completed by experienced healthcare providers. Self-debriefing including information on biomechanical posture and movement did not lead to an improvement in chest compression performance. Instead of biomechanics-related instructions, self-debriefing delivered during CPR training for healthcare providers should focus on the gap in individual CPR quality.
Footnotes
Acknowledgements
The authors are grateful for the support from the Chang Gung Memorial Hospital, Linkou (CMRPG3D0221). Special thanks to the Taoyuan and Hsinchu County fire departments, Taiwan, and all of the EMTs who participated in this study, especially Liang-Tien Chien, Bang-Wha Chen, Ching-Kuei Chang, and Tung-Hsiu Hung, who helped the authors arrange the trials.
Author contribution
H.-J.F. and S.-H.Y. contributed equally to this article. S.-H.Y., H.-J.F., and Y.-M.W. conceived the study. C.-J.S. and C.-J.N. supervised the data collection. S.-H.Y., C.-H.H., and C.-C.L. undertook recruitment of participating patients and managed the data, including quality control. W.-C.L. and H.-J.F. provided statistical advice and analyzed the data; C.-J.S. and C.-J.N. chaired the data oversight committee. Y.-M.W., C.-H.H., and H.-J.F. drafted the manuscript, and all authors contributed substantially to its revision. H.-J.F. takes responsibility for the paper as a whole.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the Chang Gung Memorial Hospital, Linkou, Taiwan (CMRPG3D0221).