
Abstract
Background:
Implementation of resuscitation training in school programs is a promising approach to improve rates of cardiopulmonary resuscitation use by trained bystanders. Unfortunately, theoretical cardiopulmonary resuscitation instruction alone is not sufficiently effective in developing practical skills.
Objectives:
This study aimed to investigate the effectiveness of traditional Basic Life Support training and alternative instructional methods to achieve learning objectives of Basic Life Support education.
Methods:
This quasi-experimental study was conducted in a secondary school in Ankara, Turkey. Eighty-three voluntary students were randomly allocated to theoretical (Group A), video-based (Group B), and mobile-assisted video-based instructions (Group C). All groups were led by the course teacher. Assessments were conducted in training and again 1 week later. Assessments were based on Basic Life Support knowledge and confidence performance scores.
Results:
Statistically significant difference was found for the groups’ Confidence Scale scores (F(2, 73) = 3.513, p = 0.035, ηp2 = 0.088); Group C (6.76 ± 1.70) scored higher than Group A. The groups’ Basic Life Support checklist scores were statistically significant (F(2, 73) = 28.050, p = 0.000, ηp2 = 0.435); Group C (32.32 ± 3.84) scored higher than the other groups. Statistically significant difference was found for the groups’ measurable Basic Life Support scores (F(2, 73) = 13.527, p = 0.000, ηp2 = 0.270); and Group C (23.76 ± 3.98) scored higher than the other groups.
Conclusion:
Our findings showed that all instruction methods led to increased Basic Life Support knowledge scores. The mobile-assisted program significantly increased knowledge scores. Same-group high-quality cardiopulmonary resuscitation parameters were more positive than the other instruction groups except for hand position. Group C students expressed higher confidence in their ability to act in an emergency when witnessing a victim collapse.
Keywords
Introduction
Cardiac arrest is an important public health issue and trained layperson is crucial in order to save lives and avoid its negative consequences. 1 Most sudden cardiac arrest (SCA) victims die outside of hospitals without receiving the interventions described in the Basic Life Support (BLS) Guidelines. Early bystander cardiopulmonary resuscitation (CPR) is extremely important for out-of-hospital cardiac arrest (OHCA), but most lay rescuers hesitate to perform CPR because of their concerns about resuscitation. 2 Implementation of resuscitation training in school programs is a promising approach to improve rates of CPR use by trained bystanders.
School CPR training requires different educational approaches and pedagogical principles because students’ ages differ, ranging from children to young adults. Most curricula in Europe are in accordance with the essential and simplified parts of adult BLS and include immediate recognition of SCA by checking vital signs and activating the emergency response system for calling for help and performing early CPR. Changing standard certification into large-scale BLS training is not sustainable for some programs because of the financial difficulties and time constraints. 3
As rates of bystander CPR use are unacceptably low, many schools try to find strategies to increase the percentage of the population trained in CPR. Schools are excellent places to access a large portion of the community. 4 International organizations also recommend that CPR training should be a standard part of the school curriculum. 5 For example, St John Ambulance, the British Red Cross, and the British Heart Foundation have campaigned for emergency first aid to be made a compulsory part of the curriculum. Many K12 schools worldwide follow this recommendation and implement CPR training in their health curriculum. In accordance with this approach, a Traffic and First Aid Course is compulsory for all final year students of high school in Turkey.
The CPR literature reveals that theoretical CPR instruction is not sufficiently effective in developing practical skills. 5 Other instructional methods including video-assisted instruction,6,7 simulation, multi-media learning, limited instruction, or a combination of self-directed learning and instructor-led teaching with hands-on training can be considered as an alternative for dissemination of BLS training.8,9 Cost-effective low-fidelity manikins for practicing CPR can be included in CPR training.10,11
Studies emphasize that giving effective feedback and guidance resulted in increased quality of CPR skills. International Liaison Committee on Resuscitation (ILCOR) offers use of CPR feedback-prompt devices to improve compression rate, depth, release, and hand position. These devices can be classified into two groups. True feedback devices give feedback about what students are actually doing, so students can make real-time adjustments to their CPR performance. However, prompt devices only give guidance information without measuring what the rescuer is doing. It is possible to combine both, and some devices serve this functionality in one solution. However, unit price is another barrier to including this in CPR education.
For many years, mobile phones have been seen as a distractor in educational activities.12,13 The rate of phone possession among school children is huge, 14 and efforts to restrict it in the educational environment are ineffective. 15 Nowadays, researchers have focused on whether a smartphone be a tool for learning, and they comment that mobile phones can be used proactively if students are allowed to use them purposefully to focus and engage in a given task.
Smartphones are usually equipped with a number of sensors such as for acceleration, gravity, and global location. New CPR applications (apps) using these features have provided education and guidance for BLS. Studies have shown tolerable performance results for the algorithm used in the smartphone-based feedback app and appropriate compress rate, which is defined in the 2010 American Heart Association (AHA) guideline. 16 The high-quality CPR output from using the app may assist in improving the survival rate of victims in out-of-hospital settings. 17
In this research, we focused on the effective use of alternative instructional methods in CPR training for high school students. Evaluation of the effectiveness of instruction and detecting inadequate CPR performance 18 also required multiple testing methods based on observation and measurement with devices. 19 Considering this, we aimed to investigate the effectiveness of traditional BLS training and alternative instructional methods to achieve the cognitive, psychomotor, and affective learning objectives of BLS education. 18
Methods
Participants
We conducted this quasi-experimental study in a high school in the Kecioren Anatolian Health and Vocational High School. The study was approved by the ethics committee at Hacettepe University and by the Hacettepe Provincial Directorate of National Education. Informed written consent was obtained from the students and their families. All students were grade 12 (aged 17–18 years). For the comparison of the instructional methods, three voluntary classes were determined. Each class was randomly assigned to one of the three groups: Group A, theoretical instruction (28 students); Group B, video-based instruction and practice on manikin (29 students); and Group C, video-based instruction, practice on manikin, and mobile-assisted feedback (26 students). These students have not received BLS training by any of these three methods before.
Additional CPR training was provided to the course teacher for teaching the right techniques through video-based instruction and mobile-assisted feedback. All evaluators were certified BLS instructors and refreshed their evaluating skills by repeating the “AHA evaluating skills performance” video course before the study. They were informed about the CPR rating protocol to standardize the evaluation.
Study design
The study was completed in five steps (See Figure 1):
Step 1. At the beginning of the study, researchers introduced the aim and steps of the study and asked the students for informed consent. Students took the multiple-choice BLS test (knowledge pre-test).
Step 2. The students were instructed in three different groups, and it was explained in the consecutive subheadings of Instructional design and material. Students were informed that CPR could be practiced on the pillow or soft objects if they wanted to practice it after the course.
Step 3. 1 week after the training, all students received a post-BLS knowledge test in their classrooms.
Step 4. All students performed BLS using full-body manikin (Resusci Anne). They were provided with standardized verbal instructions before the performance. All participants were asked to perform BLS for at least 2 min. Three observers blind-evaluated the students using a BLS checklist, and they are not informed about which group the students belonged to. Performance outputs were also provided from the Resusci Anne Skill reporter.
Step 5. All students completed the Confidence Scale and answered open-ended questions.
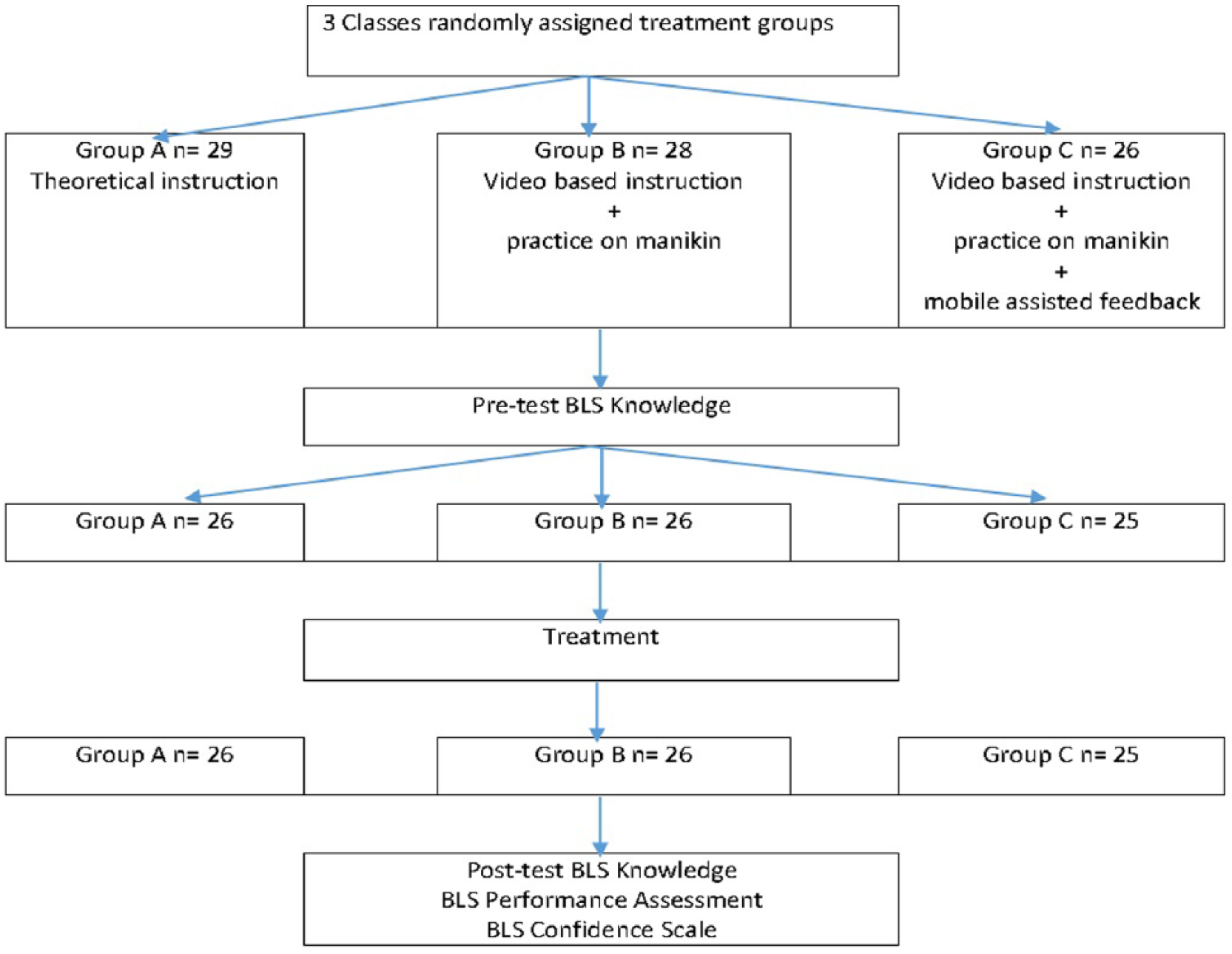
Study design.
Instructional design and material
All groups were led by the course teacher. The course took two lesson periods (40 min each):
Group A—theoretical instruction. The ongoing training in the Traffic and First Aid Course was conducted. A lecture enriched with a slide presentation was used for this group. The content of the lecture included the definition of SCA, patient and environmental safety, information on bystander BLS, and the chain of survival. There was no BLS practice in this group.
Group B—video-based instruction and practice on manikin. A video instruction was implemented. This structured video lasted 7 min and covered the step-by-step principles of BLS with a full demonstration on a full-size body manikin without automated external defibrillation (AED). The course teacher provided detailed information during the video demonstration. This part of the course took 20 min. Then, the students were divided into five groups (five students in each group) for practice. Each student self-practiced BLS skills with a Basic Buddy CPR Manikin for at least 2 min. The teacher served as the facilitator and assisted the students during the practical session. The practical part of the course took 60 min.
Group C—video-based instruction, practice on manikin, and mobile-assisted feedback. The same video demonstration and practical session as in Group B was provided to the students in Group C. The main difference of Group C training was that the students used a smartphone app while practicing and used it for self-instruction. Students brought their smartphones to the course and downloaded the PocketCPR app from the Internet. PocketCPR estimated the chest compression depth and rate using the built-in accelerometer in the smartphone and provided a feedback function for chest compression depth training. 20 A simple apparatus was designed to easily hold the phone on the back side of the hand for hands-free use (See Figure 2).

Hand apparatus and demonstration of the application on the manikin.
Instruments
BLS knowledge test
We developed a test using the official course book of the Ministry of National Education and the latest AHA and Emergency Cardiovascular Care (ECC) guidelines. The test included 15 multiple-choice questions covering the safe approach (1), checking for breathing (2), checking responsiveness and calling for help (3), time span for starting compressions (4), chest location for applying pressure (5), hand location for applying pressure (6), pressure depth (7), doing 30 chest compressions (8), checking airway (9), ensuring two ventilations (10), effective breathing (11), compression and ventilation ratio per sequence (12), respiratory obstruction and CPR (13), checking for response every 2 min (14), and conditions for terminating CPR (15).
Observable BLS checklist
A checklist was developed to evaluate the students’ CPR performances. The checklist included the critical performance steps from the Heartsaver® CPR AED Skills Sheet except for AED-related items. In addition, evaluation was detailed by adding three technical skill items: keeping elbows straight, giving breath with the head-tilt chin-lift maneuver, and letting the chest return to the normal position. There were 14 factors (See Table 1) rated on a 3-point scale: correct (3 points), incomplete (2 points), or not observed (1 point).
Items of Observable BLS Skills Checklist.
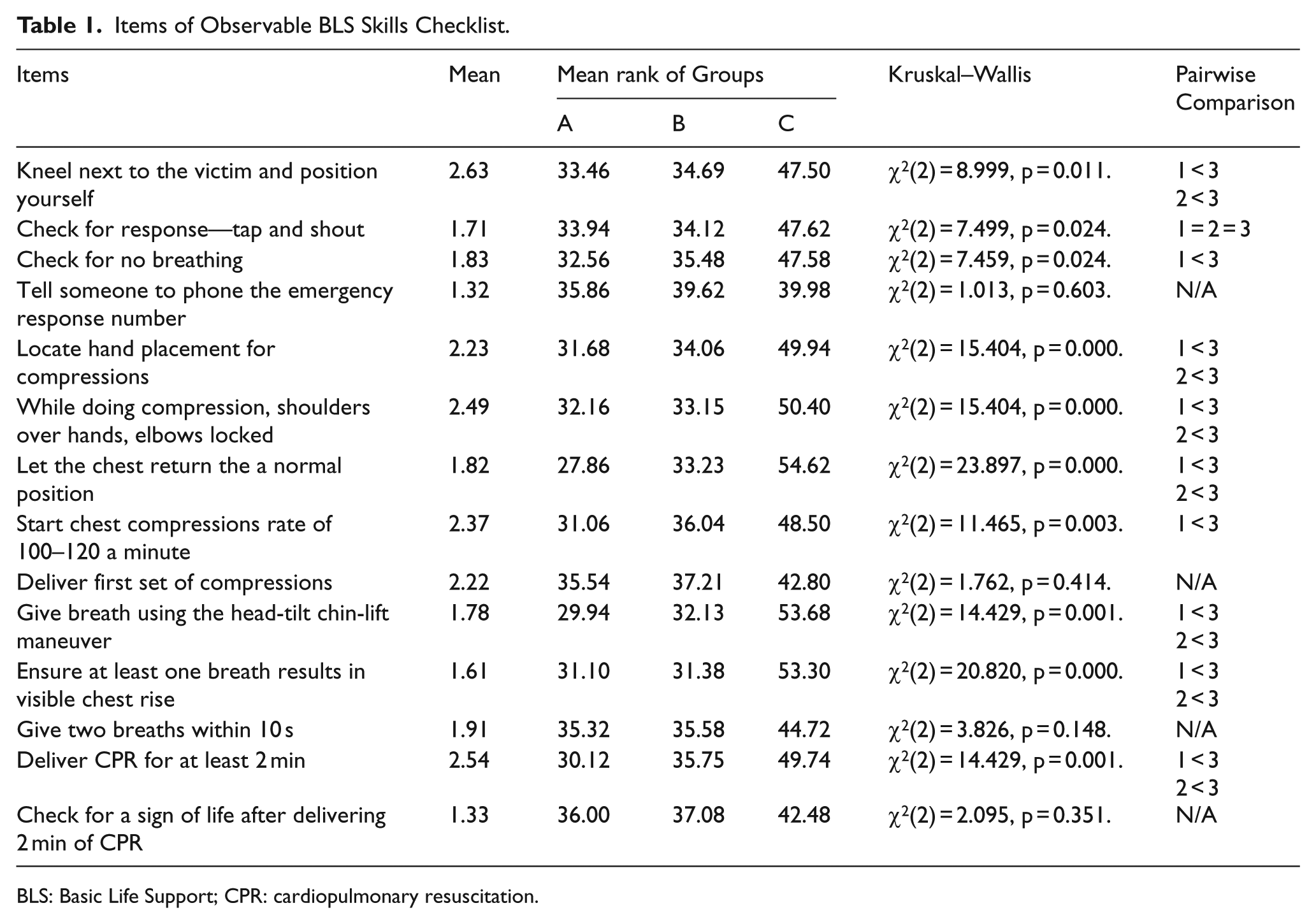
BLS: Basic Life Support; CPR: cardiopulmonary resuscitation.
Measurable BLS skill checklist
Laerdal Resusci Anne Skill Reporter measures CPR performance and provides clear information about the chest compression and ventilation. We used the overall performance scores and the summaries of the data from student BLS performances (See Table 1).
Confidence Scale
We used a visual analog scale to determine students’ confidence in performing BLS (How confident are you about your ability to perform BLS in a situation when you are alone and an adult needs your help?). The students marked a point on a continuous line between 0 (not being able to perform BLS at all) and 10 (being able to perform BLS confidently).
Thematic list of confidence statements
We also asked them to explain the reason for their choice on the Confidence Scale with an open-ended question. The answers of students about their reasons for the choice were coded thematically. Themes were derived from the literature before coding: Fear of doing something wrong (1), 21 reluctance to do mouth-to-mouth breathing (2), fear of disease transmission and legal liability (3), 22 and inability to do anything because of panic (4).2,3
Statistical methods
One-way analyses of variance (ANOVAs) were used to evaluate the data gathered from the Confidence Scale and BLS performance data. Kruskal–Wallis test statistics were used for items on the observable BLS checklist and manikin skill report. Repeated-measures mixed ANOVAs were used for pre-test and post-test BLS knowledge scores. Open-ended statements were summarized under the pre-determined thematic list.
Results
Results were reported under cognitive, affective, and psychomotor components of BLS skills. The difference between BLS knowledge pre-test mean scores of groups was not statistically significant (mixed ANOVA, F(2, 73) = 0.202, p = 0.817). This finding was interpreted as groups were balanced for the distribution aspect of BLS knowledge. There was significant interaction between teaching approaches and time, Wilks’ Lambda = 0.87, F(2, 73) = 12.16, p < 0.01, ηp2 = 0.13. There was a substantial main effect for time, Wilks’ Lambda = 0.23, F(1, 73) = 242.55, p < 0.01, ηp2 = 0.77, with all groups showing an increase in BLS knowledge scores across the test periods.
The main effect comparing the three types of intervention was significant, F(2, 73) = 4.61, p = 0.013, ηp2 = 0.11, suggesting differences in the effectiveness of the three teaching approaches.
The difference between Confidence Scale mean scores of groups was statistically significant (one-way ANOVA, F(2, 73) = 3.513, p = 0.035, ηp2 = 0.088). Post hoc multiple comparisons using Tukey’s test revealed that Group C (6.76 ± 1.70) mean scores were higher than those of Group A (5.54 ± 1.66, p = 0.028). Group B (6.23 ± 1:1.95) confidence mean scores were not significantly different from the other groups.
Students reported fear of poor knowledge and/or imperfect performance of CPR as well as fear of doing something wrong, fear of exacerbating the situation, and fear of being the cause of the person’s death.
The difference between mean observable BLS checklist scores of groups was statistically significant (one-way ANOVA, F(2, 73) = 28.050, p = 0.000, ηp2 = 0.435). Post hoc multiple comparisons using Tukey’s test revealed that Group C (32.32 ± 3.84) mean scores were higher than those of Group A (25.04 ± 3.59, p = 0.000) and Group B (26.04 ± 3.77 p = 0.000). The percentages of the observable BLS checklist items were also calculated to explore the skill steps in detail (See Figure 3).
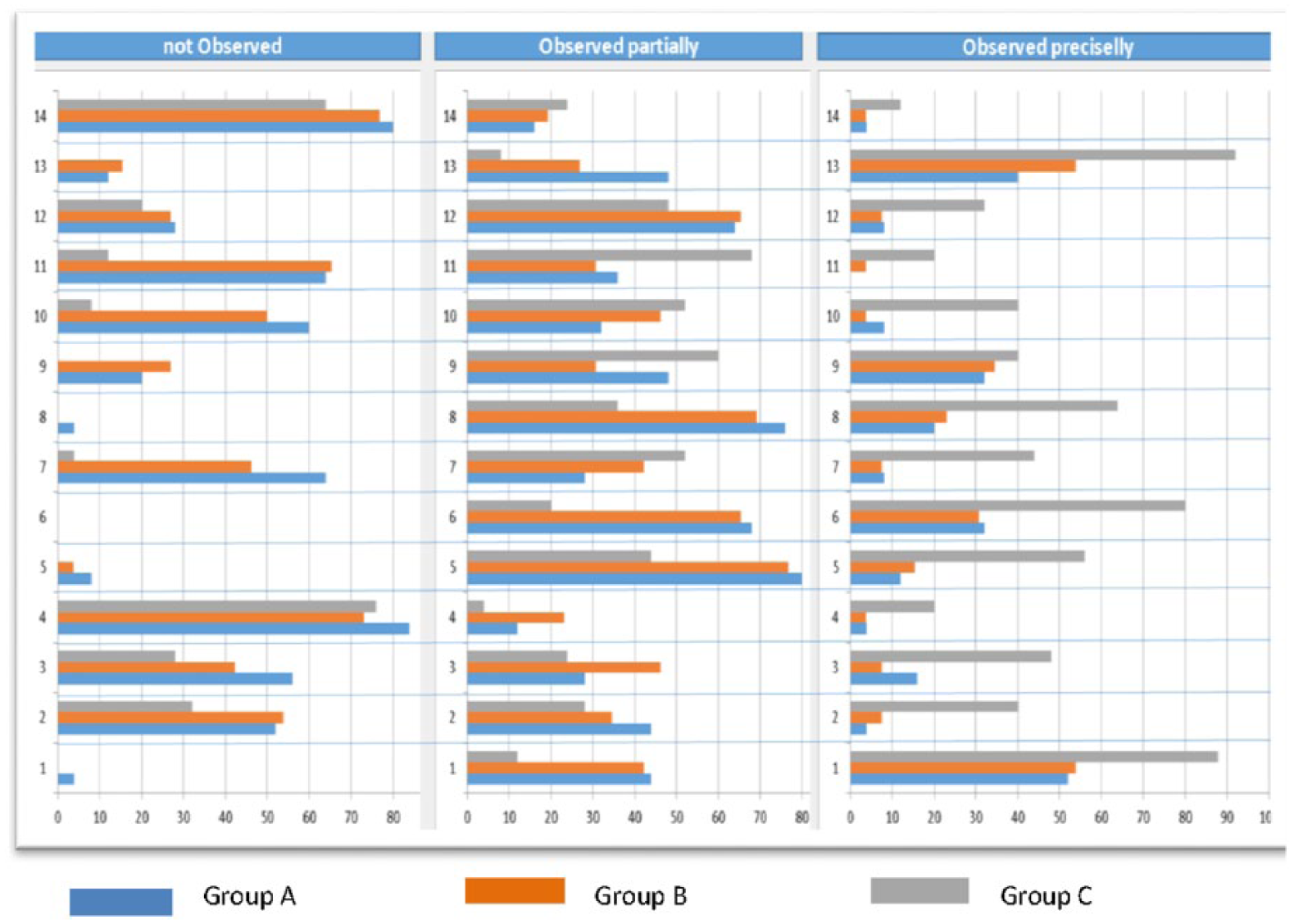
The percentage of observable BLS checklist items in the observation categories.
A Kruskal–Wallis H test showed that there were statistically significant differences between groups’ observable BLS checklist scores (See Table 1):
Item 1 value was χ2(2) = 8.999, p = 0.011. Group C performed significantly better on position at 47.50 compared to Group A (33.46) and Group B (34.69).
Item 2 value was χ2(2) = 7.499, p = 0.024. Pairwise comparisons were not significant for instruction groups. Response scores were as follows for Group C (47.62), Group A (33.94), and Group B (34.12).
Item 3 value was χ2(2) = 7.459, p = 0.024. Group C performed significantly better on checking for no breathing at 47.58 compared to the Group A (32.56). Pairwise comparison was not significant for Group B (35.48).
Item 5 value was χ2(2) = 15.404, p = 0.000. Group C performed significantly better on hand placement at 47.58 compared to Group A (31.68) and Group B (34.06).
Item 6 value was χ2(2) = 14.476, p = 0.001. Group C performed significantly better on shoulders and elbows at 50.40 compared to Group A (32.16) and Group B (33.15).
Item 7 value was χ2(2) = 23.897, p = 0.000. Group C performed significantly better on chest return at 54.62 compared to Group A (27.86) and Group B (33.23).
Item 8 value was χ2(2) = 11.465, p = 0.003. Group C performed significantly better on compressions rate at 48.50 compared to Group A (31.06). Pairwise comparison was not significant for Group B (36.04).
Item 10 value was χ2(2) = 20.815, p = 0.000. Croup C performed significantly better on giving breath better at 53.68 compared to Group A (29.94) and Group B (32.13).
Item 11 value was χ2(2) = 20.820, p = 0.000. Group C performed significantly better on breath results chest raise at 53.30 compared to Group A (31.10) and Group B (31.38).
Item 13 value was χ2(2) = 14.429, p = 0.001. Group C performed significantly better on CPR delivery at 49.74 compared to Group A (30.12) and Group B (35.75).
The difference between mean measurable BLS scores of groups was statistically significant (F(2, 73) = 13.527, p = 0.000, ηp2 = 0.270). Post hoc multiple comparisons using Tukey’s test revealed that Group C (23.76 ± 3.98) mean scores were higher than those of Group A (17.52 ± 4.89, p = 0.000) and Group B (19.50 ± 4.09, p = 0.002).
A Kruskal–Wallis H test showed that there was statistically significant difference between groups’ measurable BLS scores (See Table 2):
Items of Measurable BLS Skills Checklist.
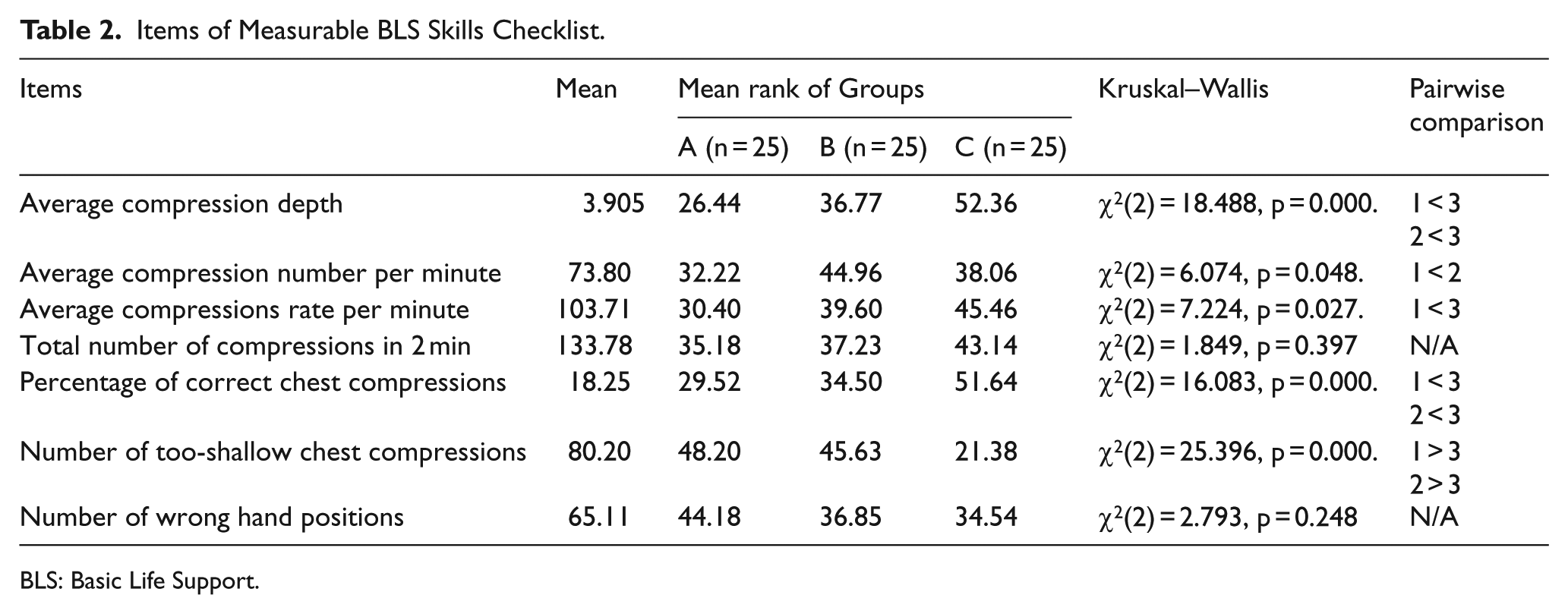
BLS: Basic Life Support.
Item 1 value was χ2(2) = 18.488, p = 0.000. Group A performed significantly better on compression depth at 52.36 compared to Group A (26.44) and Group B (36.77).
Item 2 value was χ2(2) = 6.074, p = 0.048. Group B performed significantly better on compression number at 52.36 compared to Group A (26.44). Pairwise comparison was not significant for Group C (52.36).
Item 3 value was χ2(2) = 7.224, p = 0.027. Group C performed significantly better on compressions rate at 45.46 compared to Group A (30.40). Pairwise comparison was not significant for Group B (39.60).
Item 5 value was χ2(2) = 16.083, p = 0.000. Group A performed significantly better on correct chest compressions at 43.14 compared to Group A (35.18) and Group B (37.23).
Item 6 value was χ2(2) = 25.396, p = 0.000. Group C performed significantly worse on swallow chest compression at 21.38 compared to Group A (48.20) and Group B (45.63).
Discussion
Our findings showed that all instruction methods led to increased BLS knowledge scores. This result was compatible with the literature; cognitive-only CPR training programs could achieve an acceptable standard level of proficiency. 5 A study from Denmark brief BLS training which combines theoretical introduction with hands-on practicing increased students’ BLS knowledge. 21
Comparing the instructions, the mobile-assisted program significantly increased the knowledge scores of the students with regard to time and group variables, as shown in the repeated measure mixed ANOVA. This result requires explanation, because all groups had same official course time, and Group A spent all course time for knowledge acquisition while the other groups (Group B and C) used structured video, which covered only cognitive components to enhance psychomotor BLS skills. The highest knowledge score of Group C may be because group members had supported their learning with self-instruction and had opportunity for repetitive practice guidance and feedback, which should be effective on their knowledge score. 5
Considering availability of hands-on practicing, it can be expected7,18 that Groups B and C had to obtain a greater quality CPR parameter than Group A. However, comparisons of BLS manikin skill reports with one-way ANOVA show that only compression-related BLS skill rates were more positive in Group C than the other instruction groups. Video-mediated hands-on practicing by Group B did not result in mastery of psychomotor BLS skills. It can be concluded that, considering course time and total number of group members, instructor guidance per student and practicing time were ineffective. 23 Directive CPR feedback devices are useful for improving compression rate, depth, release, and hand position. 8 The smartphone app not only prompted BLS steps but also measured quality data, which were processed and resulted in feedback such as visual information or voice messages like “good rate,” “start CPR,” or “push hard.” 24
When examined in detail, Group C’s high-quality CPR parameters were a more positive exemption for hand position. We consider that three reasons could lead to this situation. First, in the regular BLS course, students learned where chest compressions were performed and practiced hand placement on the manikin sternum. If hand position was wrong, students received corrective feedback from the instructor; this requirement was not met by the smartphone app because it was unable to estimate the hand position. Second, Group C members practiced on pillows or soft objects, which were dissimilar from human chest anatomy. Finally, instructions considering practice time and guidance by an instructor seemed to be insufficient to correct hand positions on the chest. Short experience time without guided reflection was insufficient to promote practice change.18,25
In this study, observers rated hand position scores of Group C more positively, but skill reporter results showed that differences were not significant. If observer rates and skill reporter results did not support each other, we accepted the skill reporter results as more reliable. 26
All instruction groups were far from meeting the targeted learning objectives related to environment safety, activating emergency response system, and ventilation performance. Only one of four students activated the emergency response system and checked for life signs after delivering 2 min of CPR. All students’ ventilation-related skills were poor (Items 10, 11, 12). Even if 20% of students in Group C performed chest rise, the skill reporter found this attempt to be ineffective. Instruction groups were ineffective at opening the airway and neglected the ventilation steps. 27 One of the possibilities for the low ventilation rate of students may be insufficient hands-on practice time and tutor support per student. The instructor’s role for motivation, enthusiasm, and feedback in CPR training is critical. Although Group C had the opportunity for repetitive practice via a mobile device, the smartphone app was designed for hands-only CPR, and self-instruction did not include ventilation skills. 28 Learners and rescuers should consider personal and environmental risks before starting CPR.
The result of this study confirmed that BLS training increases laypersons’ confidence. 22 Results showed that Group C students expressed higher confidence in their ability to act in an emergency when they witnessed a victim collapsing. Montgomery et al. 29 also reported that repetitive practice increased confidence in laypeople.
Students had multiple reasons for not performing CPR (e.g. panic, fear of failure (poor knowledge and/or imperfect performance), and that the potential harm that could be caused by the rescuer). 25 Similarly, in the study, a minority of the students stated that they would prefer to do nothing because of fear of doing something wrong. No one response expressed fears of infection and litigation. This report is compatible with Swor et al. 2 It was indicated that fear decreased with repeated training. 30 As the study did not include repetitive training, we could not test this.
Conclusion
Simplified BLS training led to increased BLS knowledge score, but the development of psychomotor and affective skills varied between groups. Comparing the instructions, the mobile-assisted program significantly increased the knowledge scores of the students. Theoretical BLS training did not result in mastery of basic psychomotor skills without hands-on practice. 5 Self-instruction, guidance, and feedback by the smartphone app improved students’ compression quality and confidence scores. The app also provided extra training time when the learners needed it.
Dissemination of BLS education using standard lower-fidelity manikins and the use of smartphones as prompt devices are appropriate for BLS courses. Although simplifying BLS training with hands-on practice and self-learning methods are considered to be useful, researchers should be aware of the importance of instructor feedback, motivating attitude, and expertise for answering student questions related to the emergency conditions.
This study suggests for future research that assessing educational outcomes requires multiple measurement methods and comparison and verifying techniques. Future training should evaluate the impact of repeated courses, retention of BLS skill, and training as a mandatory component of the high school curriculum. Further research is needed on use of smart devices to estimate the compression location and match it with the real hand placement for deficiency of guided feedback.
Limitations
The participating school was a vocational high school, and female students were in minority. Group members consisted of mainly male students. The students in Groups B and C used half-body, low-fidelity manikins during the instruction, and all instruction groups were tested with full-body, high-fidelity manikins. It was assumed that allocated time was sufficient considering the limited time for instruction. We were unable to determine the usage time of smartphones for hands-on training outside of school. Although the participants represented a variety of usage time, these results may not be generalizable to the entire population. Our findings show only participants’ post-intervention confidence scores and interpretations; these self-report expressions alone cannot be interpreted as meaning change in confidence originating from the difference in instruction.
Footnotes
Acknowledgements
The authors certify that they have participated sufficiently in the work to take public responsibility for manuscript. Furthermore, authors certify that this manuscript will not be submitted to or published in any other publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The authors can share any data and materials that reported in the study.
Informed consent
The authors obtained informed consent from the students and their family.
Ethical approval
The study was approved by the ethics committee at Hacettepe University and by the Ankara Provincial Directorate of National Education.
Human rights
This research does not harm human rights regarding Helsinki Ethical Principles for Medical Research Involving Human Subjects. This is an educational research and there is no involvement of patients in the study. The study was approved by the ethics committee at Hacettepe University and by the Ankara Provincial Directorate of National Education. These boards had requested an informed consent from the students’ family, and we obtained the approval as we met the conditions. The authors assure that there is no mention of specific gender or age is present in the paper.