
Abstract
Background:
Conventional hands-on chest compression, in cardiopulmonary resuscitation, is often inadequate, especially when the rescuers are weak or have a small physique.
Objectives:
This study aimed to investigate the potential of leg-foot chest compression, with and without a footstool, during cardiopulmonary resuscitation.
Methods and Results:
We prospectively enrolled 21 medical workers competent in basic life support. They performed cardiopulmonary resuscitation on a manikin for 2 min using conventional hands-on compression (HO), leg-foot compression (LF), and leg-foot compression with a footstool (LF + FS). We analyzed the compression depths, changes in the rescuers’ vital signs, and the modified Borg scale scores after the trials. The compression depth did not differ between the cases using HO and LF. In the case of LF + FS, compression depths ⩾5 cm were more frequently observed (median, inter-quartile range: 93%, 81%–100%) than in HO (9%, 0%–57%, p < 0.01) and LF (28%, 11%–47%, p < 0.01). The increase in the heart rate or modified Borg scale scores, after the trials, did not differ between the HO and LF group; however, the values were the lowest in the case of LF + FS (49 ± 18 beats/min and 5 (4–7) in HO, 46 ± 18 and 6 (5–7) in LF, and 32 ± 11 and 2 (1–3) in LF + FS, respectively, p < 0.01). However, the increase in blood pressure, SpO2, and respiratory rate were not different among each group. The increases in the heart rate and modified Borg scale scores negatively were correlated with the rescuers’ body size, in the case of HO and LF, but not LF + FS.
Conclusion:
LF can be used as an alternative to HO, when adequate HO is difficult. LF + FS could be used when rescuers are weak or have a small physique and when the victims are bigger than the rescuers.
Introduction
In cardiopulmonary resuscitation (CPR), chest compression is often incomplete, especially when the rescuer is weak or has a small physique. A rescuer’s exhaustion, in the case of prolonged CPR, can lead to the deterioration of the quality of CPR. Leg-foot compression (LF) has been advocated as one of the CPR options,1–3 but is no longer included in the new international guideline of CPR 4 because of the lack of evidence on its efficacy. However, when rescuers are weak or have small physiques, are alone and tired after prolonged CPR, or when the risk of infection to rescuers is suspected, LF could be an alternate option. Furthermore, if a footstool is available, LF can improve CPR quality through both a higher performance efficacy and lower levels of fatigue, owing to the effective use of a rescuer’s weight.
Accordingly, this study aimed to compare conventional hands-on compression (HO), LF, and LF with a footstool (LF + FS) in terms of (1) the efficacy of chest compression, (2) changes in the rescuers’ vital signs and the degree of fatigue after the trials, and (3) their relationships with the rescuers’ body size.
Methods
We prospectively enrolled 21 healthy medical workers competent in basic life support. We recorded their height, weight, body surface area (BSA), and sole size and instructed them to perform HO, LF, and LF + FS. The order of the different trials was randomized by the envelope method. We used a CPR manikin (Little Anne®; Laerdal Medical AS, Stavanger, Norway) laid on the floor and a monitor/defibrillator (HeartStart MRx®; Philips Medical Systems, Andover, MA, USA) equipped with a depth indicator (Q-CPR®; Philips Medical Systems). The monitoring device was shielded from the rescuers during the trials. Before the trials, the rescuers reconfirmed how they would perform HO, in terms of hand positioning on the lower half of the sternum, maintaining a chest compression rate of 100–120 min−1 and chest compression depth of approximately 5–6 cm, and ensuring proper chest wall recoil. Furthermore, we instructed all the rescuers on the leg-foot methods. The rescuers removed their shoes, found the sternum of the victim with their sole, and covered the whole sternum with the heel located on the lower half of the sternum to uncover the xiphoid process (Figure 1). 5 In the case of LF, the rescuers were required to compress the sternum with one of their soles, while standing directly over the manikin with the length of the foot parallel to the sternum, and with the weight-bearing foot placed at the side of the manikin. They were allowed to switch the leg used for chest compression when they felt tired. In the case of LF + FS, the rescuers stood on a footstool made of hundreds of paper with plastic tapes, with a height equal to the antero-posterior chest thickness of the manikin. They were instructed to compress the chest in the same place as during LF. In this study, we ignored artificial ventilation for the manikin.
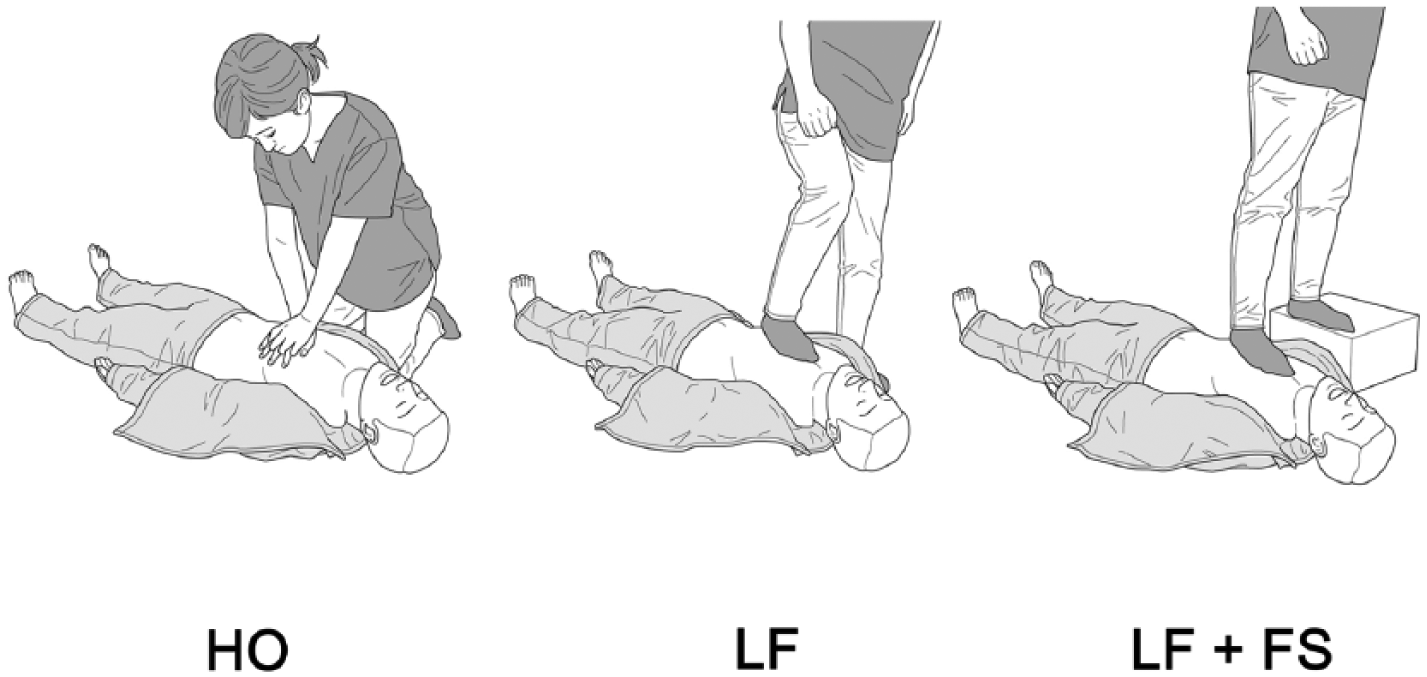
Types of chest compression.
After receiving the instructions, the rescuers’ blood pressure, heart rate, respiratory rate, and oxygen saturation of arterial blood (SpO2) were measured. During the trials, the rescuers kept track of how fast they compressed the sternum of the manikin by a metronome marking time at 100 ticks per minute. All the rescuers performed external heart compression using each method for 2 min, and this was followed by measurement of their vital signs, a resting period of 10 min, and then measurement of their vital signs again, before they switched to another method. In the three trials, we counted and recorded the number of compressions and the compression depths and categorized them into three groups: ⩽4 cm, 4–5 cm, and ⩾5 cm. We used the modified Borg scale scores for the estimation of rescuers’ fatigue after CPR. Data collection and analysis were performed after approval was obtained from the institutional review board (Hamamatsu University School of Medicine Local Ethics Committee 25-270), and written informed consent was obtained from the participants for their anonymized information to be published in this article.
Continuous data are expressed as means ± standard deviation (SD) or medians with inter-quartile range, and categorical data are shown as numbers and percentages. To analyze the changes in the blood pressure, heart rate, respiratory rate, and SpO2, and the modified Borg scale scores, a two-sided paired t-test or Mann–Whitney U test was used to compare two continuous variables with or without normal distribution. One-way analysis of variance (ANOVA), followed by a Bonferroni test and Kruskal–Wallis test, and then a Dunn test, were used to compare the compression depths, changes in the vital signs, and the modified Borg scale scores between the trials, with or without normal distribution. To analyze the relationship between the rescuers’ characteristics (height, body weight, BSA, and sole size) and elements with significant changes in the vital signs and the modified Borg scale scores, we used Pearson’s correlation coefficient test. Values of p < 0.05 were considered statistically significant. All the graphs were constructed and statistical analyses were performed using Prism version 5.0 (GraphPad, San Diego, CA, USA) and SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
The mean age of the rescuers was 33.6 ± 9.3 years; 11 of them were male and 10 were female. Their height, body weight, BSA, and sole size were 165.6 ± 8.2 cm, 59.1 ± 11.0 kg, 1.65 ± 0.17 cm2, and 25.1 ± 1.6 cm, respectively. None of the rescuers had any complications after the trials.
The number of chest compressions did not differ between the trials. The prevalence of categories in compression depth did not differ between HO and LF. Compression depths ⩾5 cm were most frequently observed in the case of LF + FS, whereas in HO and LF the depth was predominantly in the 4–5 cm range (Table 1).
Number and depth of chest compressions.
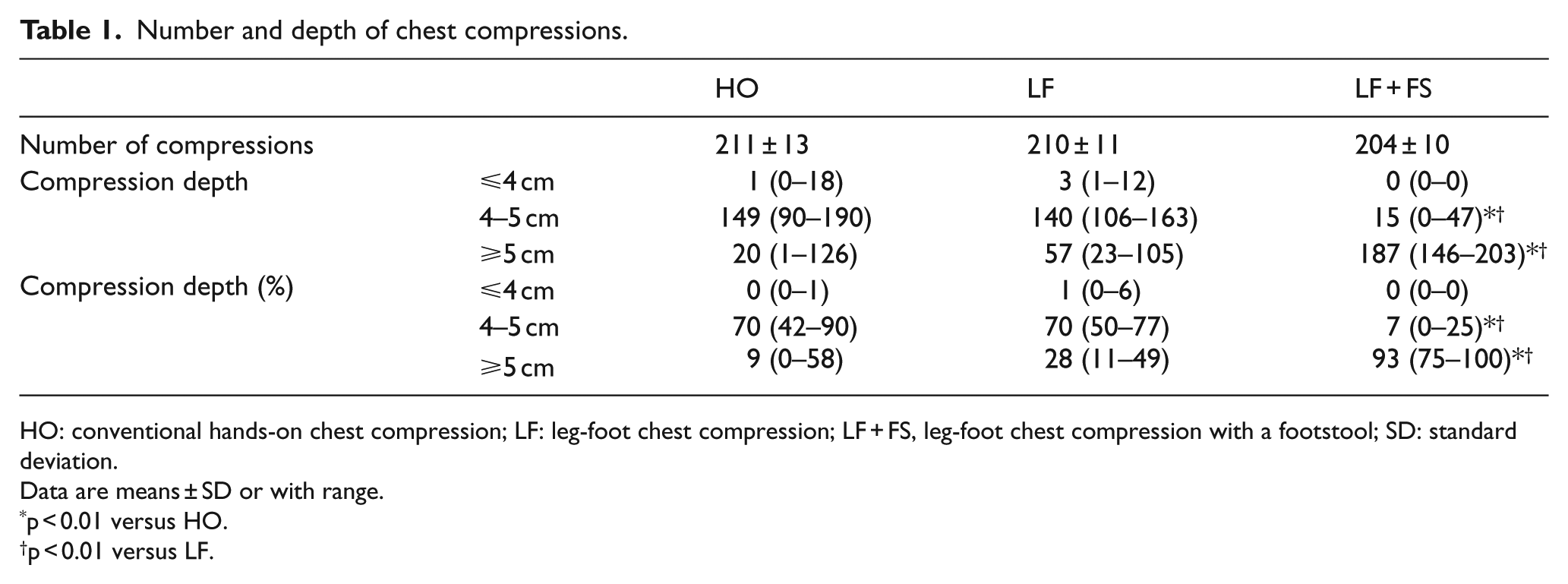
HO: conventional hands-on chest compression; LF: leg-foot chest compression; LF + FS, leg-foot chest compression with a footstool; SD: standard deviation.
Data are means ± SD or with range.
p < 0.01 versus HO.
p < 0.01 versus LF.
The changes in the rescuers’ conditions are summarized in Table 2. No significant differences in systolic/diastolic blood pressure, heart rate, SpO2, or respiratory rate were observed before each trial. The systolic blood pressure, heart rate, and respiratory rate increased significantly after each trial, whereas the diastolic blood pressure and SpO2 remained unchanged. The increase in the heart rate was not different between HO and LF, but was significantly smaller in the case of LF + FS (p < 0.01). The modified Borg scale score after the trial was lower in the case of LF + FS (median, inter-quartile range: 2, 1–3) than HO (5, 4–7; p < 0.01) and LF (6, 5–7; p < 0.01; Figure 2). In terms of HO and LF, the increases in the heart rate were negatively correlated with the rescuers’ height, body weight, BSA, and sole size (Table 3). The modified Borg scale score was also negatively associated with body weight in HO and sole size in LF. In LF + FS, no correlations were observed between the increase in the heart rate or modified Borg scale scores and any elements of body size (Table 3). In addition, there were no significant differences of changes of vital signs among the first, second, and third rounds in HO, LF, and LF + FS.
Changes in the rescuers’ vital signs after the trials.
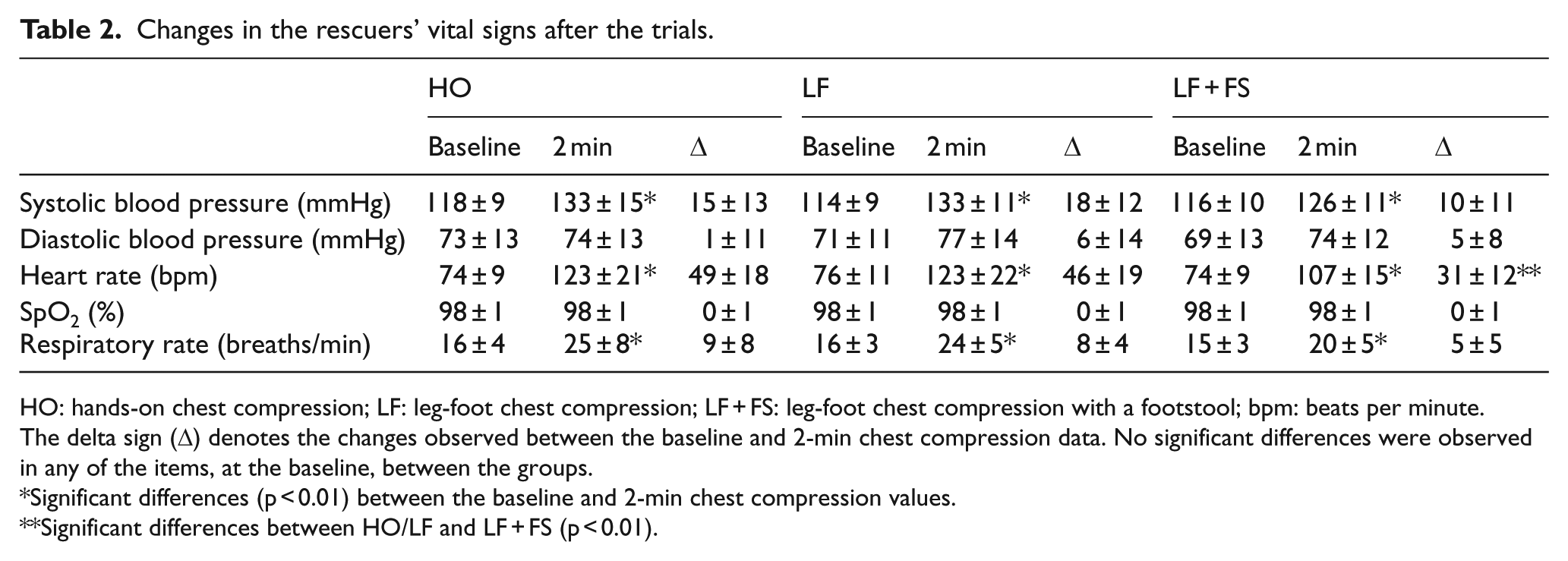
HO: hands-on chest compression; LF: leg-foot chest compression; LF + FS: leg-foot chest compression with a footstool; bpm: beats per minute.
The delta sign (Δ) denotes the changes observed between the baseline and 2-min chest compression data. No significant differences were observed in any of the items, at the baseline, between the groups.
Significant differences (p < 0.01) between the baseline and 2-min chest compression values.
Significant differences between HO/LF and LF + FS (p < 0.01).
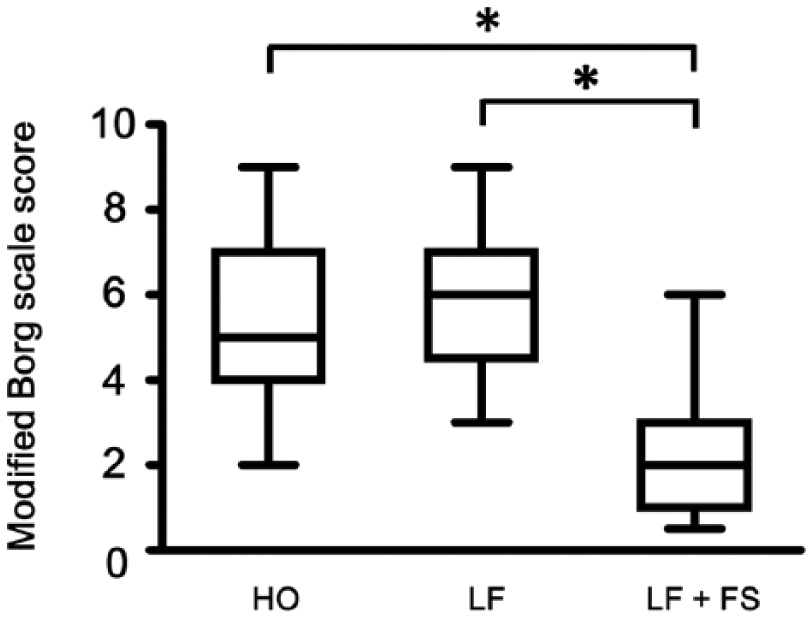
Modified Borg scale score after 2 min of chest compression.
Relationships between changes in the heart rate and modified Borg score after the trials and the rescuers’ age and parameters of body size.
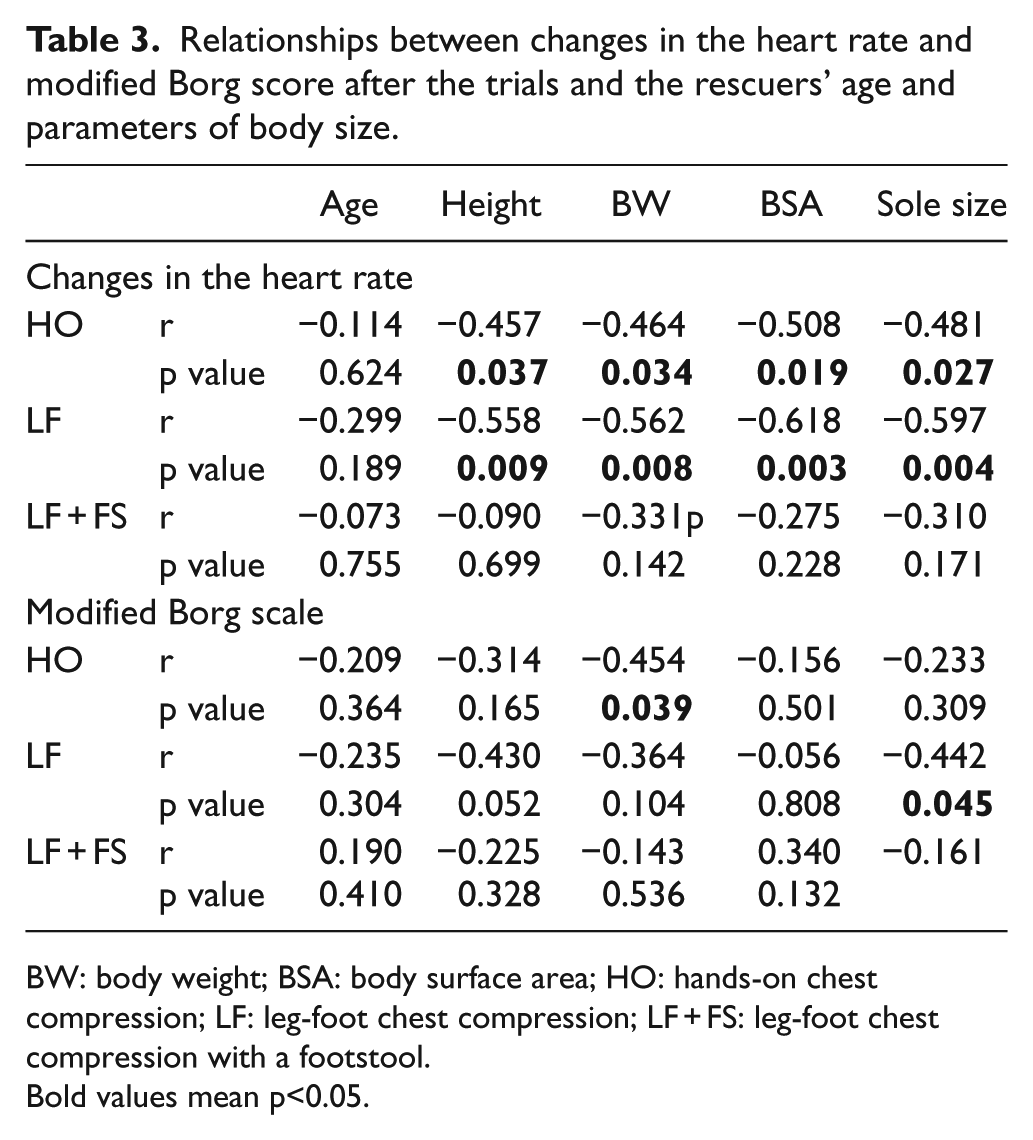
BW: body weight; BSA: body surface area; HO: hands-on chest compression; LF: leg-foot chest compression; LF + FS: leg-foot chest compression with a footstool.
Bold values mean p<0.05.
Discussion
In this study, we demonstrated that (1) the compression depths were predominantly in the 4–5 cm range in HO and LF and ⩾5 cm in LF + FS; (2) the increases in heart rate and the modified Borg scale score, after the trials, did not differ between HO and LF but were smaller in LF + FS; and (3) the increases in heart rate and the modified Borg scale score were negatively correlated with the rescuers’ body size in HO and LF, but not LF + FS.
In CPR, chest compressions ⩾5 cm can improve the success rate of defibrillation and the return to spontaneous circulation.6–9 However, the measured compression depth during adult human CPR often remains <4 cm.10–12 A chest compression depth of 5–6 cm is recommended in the international guideline, 4 and this also applies to CPR performed by non-professional rescuers, in the case of out-of-hospital arrests. All the participants in this study were professional rescuers, and the prevalence of compression depths ⩽4 cm was very low in all the trials. Thus, the rescuers in this study were able to perform almost proper manual CPR.
In the case of an emergency, a rescuer needs to apply chest compression to a patient for at least a few minutes until emergency medical dispatchers arrive. If nobody else is around, the rescuer has to perform the chest compression alone. Subsequently, the chest compression will become weaker, over time, as the rescuer becomes more tired, resulting in poor-quality CPR and lower recovery rates without neurological complications. Previously conducted studies on the efficacy of CPR predominantly focused on patients’ statuses; however, few studies have focused on rescuers’ fatigue in the different methods. This study showed that both the increases in the heart rate and modified Borg scale score were negatively correlated with the body size of the rescuers in HO. This means that rescuers with a larger body size can perform proper chest compression for a longer time, whereas those with a smaller body size may get tired and be unable to maintain adequate HO for prolonged periods.
In this study, almost the same efficacy, with regard to chest compression depth and rescuers’ fatigue, was observed in the case of HO and LF. Interestingly, unlike in the case of HO, LF with shoes on can prevent rescuers from contracting infections through blood or vomit. If a rescuer needs to use the phone while performing CPR, and is willing to call an emergency service or parties concerned, LF allows him or her to make a call without the discontinuation of CPR. More importantly, while HO is unavailable to rescuers with disabilities of the arms or hands, LF allows for their performance of CPR. It is of concern that artificial ventilation using a pocket mask becomes more difficult when only one rescuer performs LF, compared to the case of HO. However, it has been described that continuous chest compressions only led to an improvement in the survival to hospital discharge, relative to standard CPR with chest compression and ventilation.13–16
This study demonstrated that LF + FS produced deeper compression and fewer increases in the heart rate and modified Borg scale score of rescuers, after the trials, compared to HO and LF. Furthermore, none of these elements were correlated with the rescuers’ body size. These findings imply that LF + FS could improve the efficacy of chest compression and extend the duration of proper chest compression, especially for rescuers with smaller body sizes. However, a previously conducted study reported that the prevalence of injuries in victims elevated from 28% and 27% to 49% when compression depths were compared between <5 cm and 5–6 cm and >6 cm. 17 It is recommended that the chest compression depth not exceed 6 cm, in spite of the low quality of the evidence in the guideline. 4 Thus, larger sized rescuers should avoid performing LF + FS. Conversely, smaller sized rescuers, such as children or thin women, might use LF + FS instead of HO. Although LF + FS cannot be performed if there is no footstool nearby, alternatives to footstools can be easily found, such as an encyclopedia at home, a suitcase in an airport, or a stone in a camp field. Consequently, while LF + FS may become one of the resuscitation options for use in everyday life, it should be carefully applied to restricted cases for weak and small rescuers.
Limitations
This study examined the efficacies of different chest compression methods in professional rescuers from a single center. Therefore, our data may not be applicable to diverse groups of rescuers. Moreover, we used a manikin instead of real human beings. The manikin has a spring inside the chest to imitate a real human body, therefore the chest recoil of the manikin is stable; whereas, real human bodies are vulnerable to rib fractures. In addition, to validate the usefulness of LF and LF + FS, we need to investigate these methods, enrolling various non-professional rescuers, especially elderly adults and children. Finally, the use of LF + FS should be considered in the worst situation that no other options are available.
Conclusion
When rescuers, especially those who are weak or have smaller physiques, are fatigued due to the prolonged duration of CPR and cannot maintain adequate HO, or when the risk of infection is suspected, LF can be used as an alternate option. Although this study demonstrated the superiority of LF + FS, its efficacy and safety must be evaluated carefully in real-world settings.
Footnotes
Acknowledgements
We thank Shigeru Kuriyama and Yusuke Ohta for their outstanding team work. Y.T. and T.S. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.