
Abstract
Background:
The evidence supporting delivery of quality cardiopulmonary resuscitation is growing and significant attention has been focused on improving bystander cardiopulmonary resuscitation education for laypeople. The aim of this randomized trial was to assess the effectiveness of instructor’s real-time objective feedback during cardiopulmonary resuscitation training compared to conventional feedback in terms of trainee’s cardiopulmonary resuscitation quality.
Methods:
We performed a cluster-randomized trial of community cardiopulmonary resuscitation training classes at Nowon District Health Community Center in Seoul. Cardiopulmonary resuscitation training classes were randomized into either intervention (instructor’s objective real-time feedback based on the QCPR Classroom device) or control (conventional, instructor’s judgment-based feedback) group. The primary outcome was total cardiopulmonary resuscitation score, which is an overall measure of chest compression quality. Secondary outcomes were individual cardiopulmonary resuscitation performance parameters, including compression rate, depth, and release. Generalized linear mixed models were used to analyze the outcome data, accounting for both random and fixed effects.
Results:
A total of 149 training sessions (2613 trainees) were randomized into 70 intervention (1262 trainees) and 79 control (1351 trainees) groups. Trainees in the QCPR feedback group significantly increased overall cardiopulmonary resuscitation score performance compared with those in the conventional feedback group (model-based mean Δ increment from baseline to session 5: 11.2 (95% confidence interval 9.2–13.2) and 8.0 (6.0–9.9), respectively; p = 0.02). Individual parameters of compression depth and release also showed higher improvement among trainees in QCPR group with positive trends (p < 0.08 for both).
Conclusion:
This randomized trial suggests beneficial effect of instructor’s real-time objective feedback on the quality of layperson’s cardiopulmonary resuscitation performance.
Keywords
Introduction
Out-of-hospital cardiac arrest (OHCA) is a major global public health issue and a leading cause of death, accounting for more than 200,000 deaths per year in the United States alone. 1 Cardiopulmonary resuscitation (CPR) is one of few modifiable factors known to be associated with increased survival for OHCA. In particular, because the vast majority of victims of OHCA die before reaching hospital, prompt delivery of high-quality CPR has been shown to be an essential link in the chain of survival for OHCA.2–5 However, while incidence of bystander CPR has been emphasized, high-quality CPR has often been overlooked.6–8 Previous studies have demonstrated that cardiac arrest outcomes are directly related to the quality of CPR provided, which includes adequate chest compression depth, rate, and minimizing interruptions in the chest compressions.9,10 As there are growing evidence supporting the importance of high-quality CPR, significant attention has been also focused on raising awareness and improving bystander CPR education among laypeople. 11
Current resuscitation guidelines emphasize the importance of providing high-quality CPR. 12 However, it was reported most bystander CPR does not meet these high-quality CPR criteria, strongly implying an urgent need for new strategies to assist in the delivery of quality bystander CPR. 7 Moreover, it is also challenging for instructors to provide accurate and objective feedback on trainees’ CPR performance. To address this issue, the 2015 American Heart Association (AHA) guidelines recommended the use of CPR feedback devices that can help to learn the psychomotor skill of CPR and provide corrective feedback on CPR performance. 13 Many attempts have been made to improve the quality of layperson CPR during training by developing various CPR feedback devices.14,15 Recently, increasing evidence support the effect of visual feedback systems in terms of high-quality chest compressions and chest compression skill acquisition for layperson. 16
One key feature of effective learning method is the provision of instructor feedback to trainees by instructor. 17 However, it is challenging for instructors to provide accurate and objective feedback on trainee’s CPR performance.18,19 The QCPR® Classroom device is a quality monitoring system, which monitors CPR performances of multiple trainees simultaneously and in real time, therefore enables instructors to give real-time feedback and coaching to those who need. To our knowledge, no previous studies have examined the effect of instructor’s real-time feedback using QCPR Classroom device during adult layperson CPR training. The aim of this randomized trial was to assess the effectiveness of instructor’s real-time objective feedback compared to conventional subjective feedback on trainee’s CPR quality.
Methods
Research ethics board approval was obtained for this research (IRB number: 1704-179-851). We received a waiver for informed consent.
Study setting and design
We conducted a prospective, cluster-randomized trial at Nowon District Community CPR Training Center in the Seoul Metropolitan Area. Since its opening in 2012, the Nowon CPR Training Center offered over 12 CPR classes each week (up to three classes per day) to residents of Nowon. This randomized trial was conducted from 18 January to 18 April 2017. During the study period, there were three CPR instructors at the Center, and each CPR class was taught by one of the three instructors.
Study participants
Adult laypeople (over 19 years) who were residents of Nowon and registered to the CPR training classes at the Nowon CPR Training Center were included in the study. Participants who did not complete the 1-h CPR training session were excluded from the study.
Interventions
QCPR Classroom device
In this trial, we used QCPR Classroom prototypes (Laerdal Medical, Stavanger, Norway), which is a real-time quality monitoring system that allows instructors to visually monitor CPR performances of multiple trainees simultaneously (up to 25 trainees for the first version and up to 42 trainees for the second version). Instrumented and individually numbered Little Anne manikins, organized in columns and rows within the classroom, connect wirelessly and automatically to a QCPR Classroom tablet (iPad with QCPR Classroom App installed), which then presents each trainee’s performance within a matrix that represents the placement of the manikins in the room. Each trainee’s CPR performance is graphically indicated as (1) good CPR performance, (2) not deep enough compressions, (3) incomplete release, (4) too fast compressions, and/or (5) too slow compressions. Figure 1(a) depicts the graphics used. From this matrix, instructors could see who are the participants who need to improve their CPR performance and could give feedback by calling out their unique manikin number. For those with not deep enough compression, the instructor gave feedback to compress deeper; for incomplete release, the instructor gave feedback to release each compression completely; for too fast compressions, the instructor gave feedback to compress slower; and for too slow compressions, the instructor gave feedback to compress at faster rate. As the trainees’ CPR performance changes, the graphic is updated. At the end of the class, the instructors were given an overall summary of each individual trainee as well as the class performance as depicted in Figure 1(b).
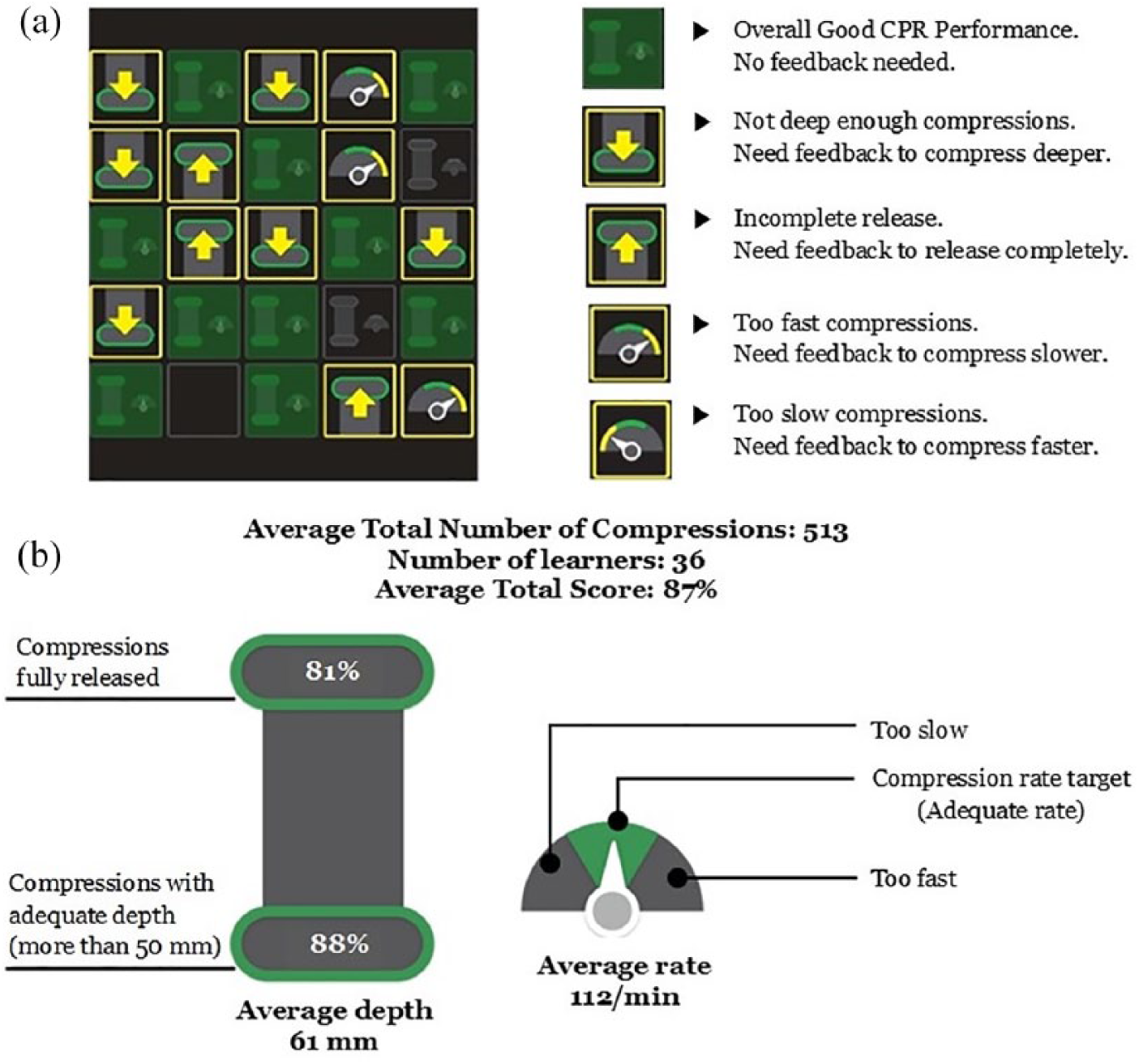
Display of QCPR Classroom real-time CPR feedback. (a) An example of instructor tablet screen with real-time trainees’ CPR performance matrices. Each of the square box on the left represents an individual trainee. Within the box, the trainee’s CPR performance matrices are indicated as (1) good CPR performance, (2) not deep enough compressions, (3) incomplete release, (4) too fast compressions, or (5) too slow compressions. Based on these matrices, instructors can identify those who need to improve their CPR performances and give feedback by calling out their unique manikin number. (b) An example of CPR feedback indicators.
Study procedures
Randomization
Each CPR training class was randomized into either real-time objective feedback group or conventional feedback group. Randomization occurred at the level of the class (cluster). During the study period, there were three CPR training classes each weekday at Nowon CPR Training Center. Using SAS programming, a randomization schedule was generated for each training day, either “QCPR Classroom-based feedback” or “Conventional feedback” days. All three CPR training classes on the day of “QCPR Classroom-based feedback” were given real-time feedback during the course of the training and all three CPR training classes on the day of “Conventional Feedback” were given conventional feedback based on the instructors’ subjective judgment. QCPR Classroom collected and stored data from all classes during the study period to the QCPR Classroom cloud server.
CPR training
Each CPR training class, which was based on the adult chest compression only protocol, was taught by one certified CPR instructor. Training was approximately 1-h course consisting of a 30 min video-based dispatcher telephone-CPR (T-CPR) training with chest compression only, a short role-play, and debriefing. This video-based T-CPR training program was implemented in four districts of Seoul Metropolitan in 2015 with Nowon district as one of them (Home Education and Resuscitation Outcomes Study, HEROS). The video included the concepts of T-CPR, bystander CPR simulation with a dispatcher using trainee’s own phone, and practice sessions following demonstration of simulated layperson. During the role-play, one trainee played as a dispatcher and the other played as a layperson for 15 min, followed by a 15-min debriefing session. HEROS program focuses on cooperation with dispatcher, from recognition to performing DA-CPR and hands-on practice so that participants can provide bystander CPR promptly in real situations.
Prior to the training, each trainee was assigned to a numbered manikin on the floor and asked to remember their manikin number. During the training, trainees were instructed to perform CPR for five separate sessions. Approximate durations of each CPR sessions were 1.5 min for sessions 1 and 2, 1-min for session 3, 3 min for session 4, and 2.5 min for session 5. During the first CPR session, no feedback was given to the trainees; therefore, session 1 was considered as baseline measure of trainees’ CPR performance quality. For the rest of sessions, the instructor provided either QCPR-based or conventional feedback to those who did not perform high-quality CPR by calling out their manikin numbers. At the end of the class, trainees were asked to complete one-page survey on their knowledge and overall experience of the course.
Outcome measures
Primary outcome measure was changes of the quality of CPR performance, measured as total score, from baseline (session 1) to session 5. The total score is an individual’s overall measure of CPR performance scored from 0% to 100%. The algorithm to calculate total score has been developed by Laerdal Medical in close collaboration with the AHA (http://cdn.laerdal.com/downloads-test/f3784/Att_2_to_00021778.pdf). For the overall score calculation of an individual trainee, compression components including depth, rate, and complete release are compared to a selected guidelines recommendation (resuscitation guidelines selected from AHA, European Resuscitation Council, Newborn Life Support, or trainer’s custom set guidelines). For those who perform CPR exactly according to the Resuscitation Guidelines selected (e.g. compression rate of 100–120/min, depth of at least 5 cm), overall score of 100% will be given. If the CPR performance deviates from the selected guidelines, the scores are reduced along S-curves outside of the thresholds (in a sinusoidal manner), meaning that the larger the deviation from the guideline recommendation, the more the score is reduced. Secondary outcome measures were changes of the following individual CPR quality parameters from baseline to session 5: average compression rate per minute, average compression depth (measured in mm), percentage of correct depth, and percentage of complete release.
Sample size
We calculated cluster sample size with a method that takes into account the intra-cluster correlation coefficient (ICC), the expected effect, and the power of the study. Based on the previous QCPR data, we calculated an ICC (ρ) of 0.03, and with a power of 80% at 5% significance level to detect a difference of 18% in total CPR scores, the required sample size would be 864 per each randomization group. Assuming each class has on average of 25 trainees, each group needed 35 clusters (classes). Under an assumption that about 10% will have missing data, we aimed to recruit 1900 participants (76 classes) in total (950 participants per study arm).
Statistical analysis
Differences in baseline characteristics by intervention group were analyzed with Wilcoxon signed rank test for continuous variables and χ2 tests for categorical variables. The primary analysis of study outcome was based on linear mixed models (PROC MIXED) for total CPR score outcome, accounting for both cluster-level (class and instructor) and individual-level (age, gender, and employment status) covariates, and an unstructured covariance matrix was assumed. The mixed models for total score outcomes from first session to fifth session and accounted for within-cluster correlation and for the repeated measures. Changes over time in the quality of CPR performances (differences between session 5 scores and baseline scores) between intervention and control groups were also assessed (difference-in-difference (D-I-D) method), accounting for cluster- and individual-level covariates.
Results of the PROC MIXED models are reported as adjusted means (calculated from least-square means) and the 95% confidence intervals (CIs). All statistical analyses were performed using SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA).
Results
Study population
The flow of participants through the study is described in Figure 2. During the study period, we had a total of 150 training classes (3183 trainees). After excluding one class with only student trainees (with less than 19 years of age), we randomized a total of 149 classes into QCPR-based feedback group (70 classes; 1322 trainees) or conventional feedback group (79 classes; 1438 trainees). After excluding those without CPR quality data due to technical manikin error (n = 18) and those who did not complete all five sessions of the CPR performances (n = 129), a total of 2613 participants were included for the final analysis with 1262 trainees in the QCPR-based feedback group and 1351 in the conventional feedback group.
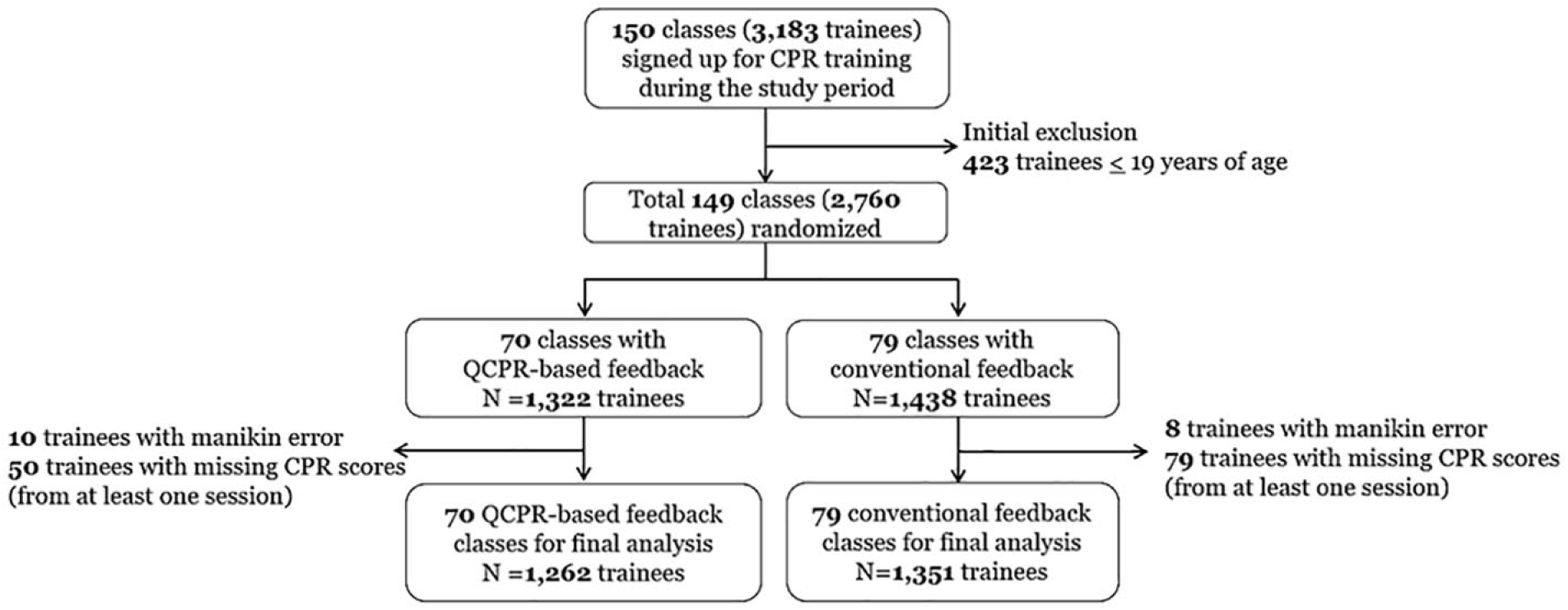
Flow of participants through the trial.
Table 1 summarizes the baseline demographics of the participants and characteristics of the study arms. There were no significant differences in the baseline characteristics of the participants between the study arms in terms of sex and age. However, trainees in QCPR-based feedback group showed higher employment status compared with those in conventional feedback group (86.8% vs 80.8%; p < 0.01). Classes in both study arms had same median number of trainees per class, which was 10 trainees per class. During the study period, there were a total of three instructors employed and there were significant differences in the distribution of the instructors between the study arms. Significantly more numbers of the instructor’s feedbacks per class were given to the intervention group (median 8 feedbacks, interquartile range (IQR) 5–12) than control group (median 6 feedbacks, IQR 5–8; p < 0.01).
Baseline demographics of the participants and characteristics of the CPR training classes.
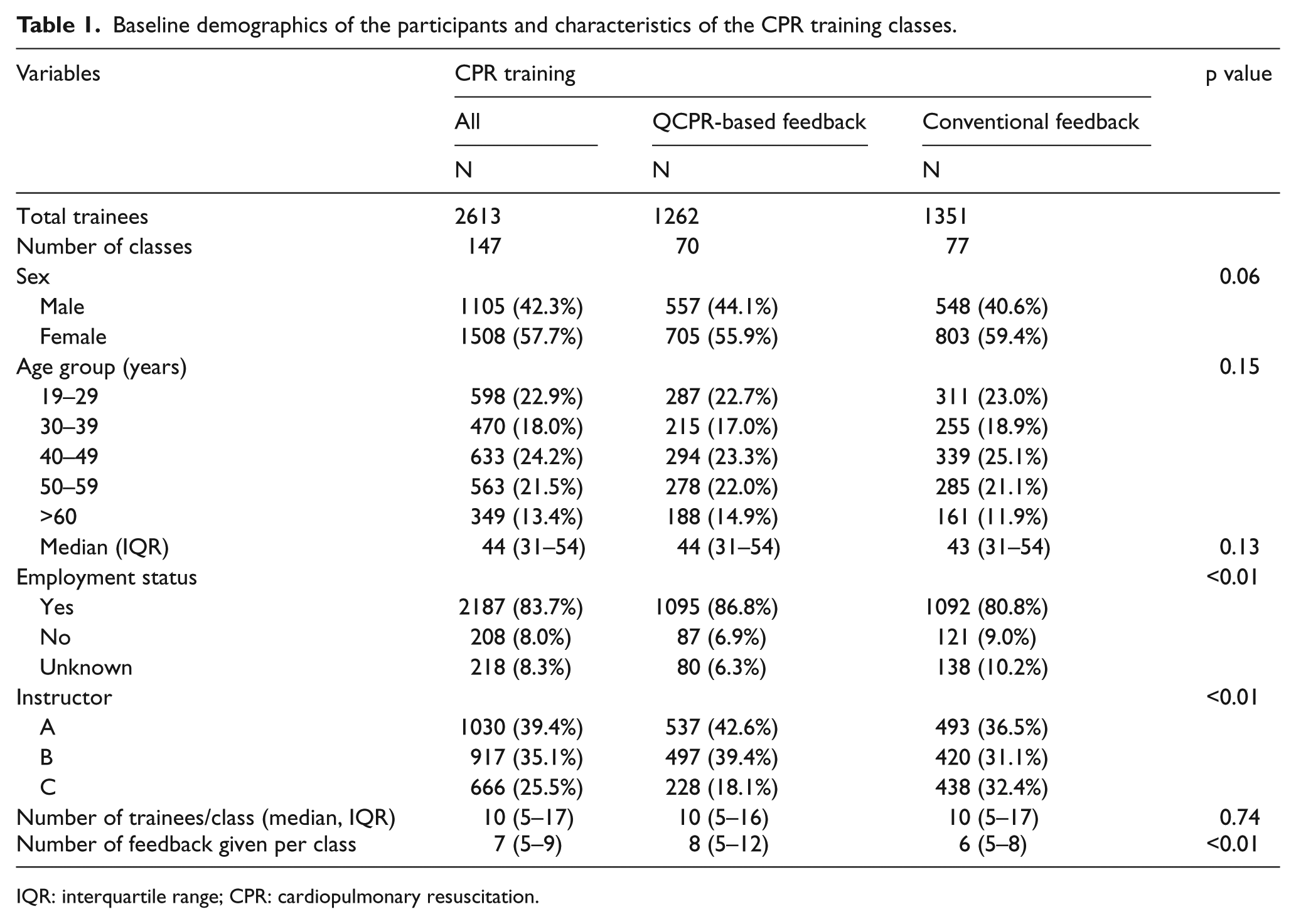
IQR: interquartile range; CPR: cardiopulmonary resuscitation.
Quality of overall CPR performance
Overall, a significantly higher total CPR performance score was observed in trainees in QCPR-based feedback group compared to conventional feedback group throughout course of the CPR trainings. Table 2 shows both crude and model-based means of CPR performance quality measures in the baseline session and session 5 and changes from baseline to the last session (session 5). In terms of changes from baseline, trainees in both feedback groups demonstrated improvements of their overall CPR performances (measured by total CPR score) by the end of the session (total score change: QCPR feedback group = 11.2; conventional feedback group = 8.0). However, those in the QCPR feedback group showed significantly greater improvements than trainees in the conventional group (D-I-D = 3.2; 95% CI 0.4–6.0; p = 0.02).
Quality of CPR performance outcomes by intervention group.
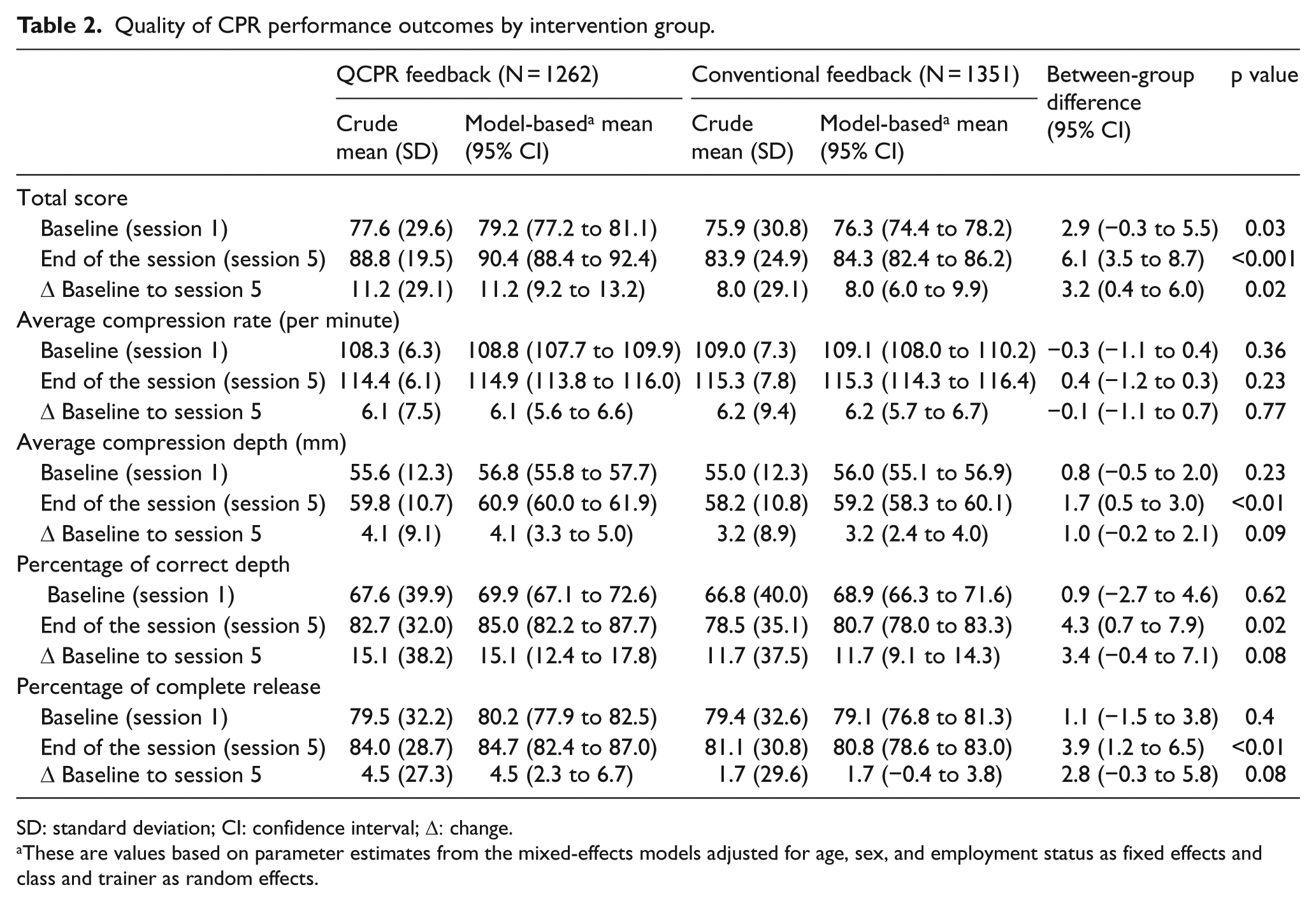
SD: standard deviation; CI: confidence interval; Δ: change.
These are values based on parameter estimates from the mixed-effects models adjusted for age, sex, and employment status as fixed effects and class and trainer as random effects.
Quality of average compression rate, depth, and release
We did not observe a statistically significant difference between the two groups for the average compression rate. Model-based average compression rate per minute changed from baseline to session 5 was 6.1 (95% CI 5.6–6.6) in QCPR feedback group and 6.2 (95% CI 5.7–6.7) in conventional feedback group with statistically non-significant differences (D-I-D of −0.1; 95% CI −1.1 to 0.7; p = 0.77). QCPR feedback group showed an average of 4.1 mm (95% CI 3.3–5.0) improvement in the compression depth compared to 3.2 mm (95% CI 2.4–4.0) in conventional feedback group. Changes in percentage of correct depth and complete release from baseline to session 5 were also higher in QCPR feedback group (model-based mean 15.1 and 11.7 for percent, respectively) than conventional feedback group (model-based mean 4.5 and 1.7, respectively). Between-group differences (D-I-D) for the individual parameters of average compression depth, percentage of correct depth, and complete release showed positive trends (p = 0.09, 0.08, and 0.08, respectively).
Survey results
On the post-training survey, students in both groups showed similar CPR knowledge skills (Table 3). There were also no differences in Likert-type scale questionnaires investing willingness to perform CPR in real-life situation as well as training course satisfaction (p > 0.05 for all).
CPR knowledge and class satisfaction survey results.
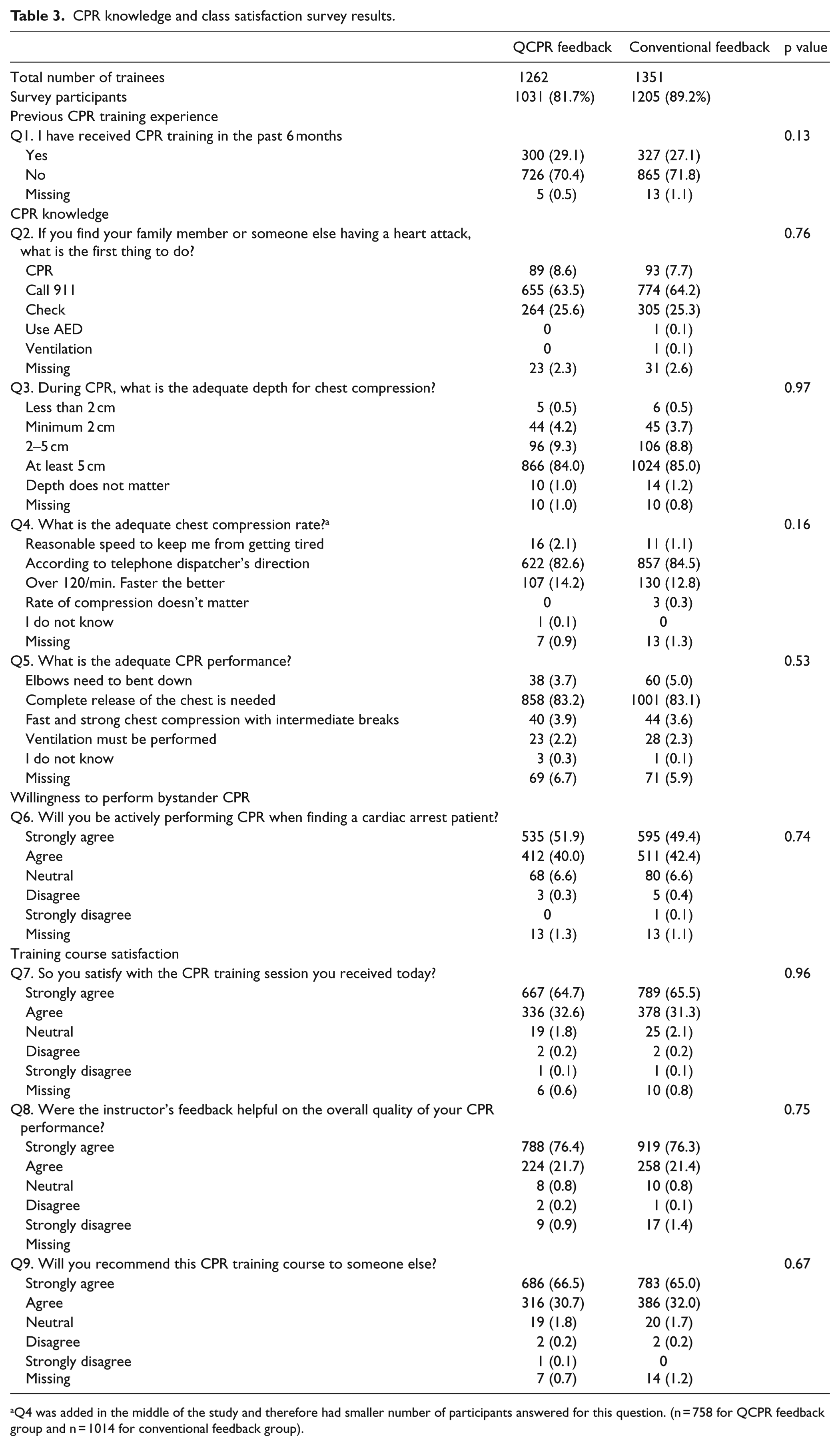
Q4 was added in the middle of the study and therefore had smaller number of participants answered for this question. (n = 758 for QCPR feedback group and n = 1014 for conventional feedback group).
Discussion
This prospective, cluster-randomized trial investigated the effect of QCPR Classroom–based instructor’s real-time objective feedback on the quality of trainees’ CPR performances. Our results showed that the instructor’s real-time objective feedback on trainees’ CPR skills during training showed a positive trend in improving the overall CPR performance quality of trainees. When considering chest compression parameters separately, trainees in QCPR group showed better compression depth and chest release, suggesting that the observed difference in total CPR performance scores may be attributed mainly in the difference in compression depth and chest release.
With consistent growing of importance of bystander CPR training, as well as high-quality CPR, several different training methods and feedback technology have been developed. A computer-based real-time audiovisual feedback system, which gives corrective instructions when errors of technique are detected during CPR training, is one of the most widely used methods that has been shown to be effective.20,21 There is good evidence supporting the use of CPR feedback devices during CPR training to improve both CPR acquisition skills and retention.22,23 In a randomized controlled manikin study, Baldi et al. 24 demonstrated significant improvement in CPR performance parameters, including correct depth, percentage of compressions with a complete chest recoil, compressions with the correct hand position, and total CPR score, in the groups receiving real-time visual feedback during Basic Life Support and Automated External Defibrillation training courses compared to the group without real-time visual feedback. However, some studies also show negative effects of these devices.25,26 Zapletal et al. 26 investigated the effects of three CPR feedback devices (including audiovisual devices) on CPR quality in 240 trained medical students and found that none of the devices improved chest compression efficiency. The study further reported delay in CPR start when using the feedback devices, suggesting that inability to improve quality of CPR performance may arise from complexity of the real-time audiovisual feedback that an individual may encounter while performing CPR.
In community layperson CPR training settings, while audiovisual feedback devices can be used to provide real-time objective feedback on trainee’s CPR performance, at the same time, the trainees may encounter difficulty in concentrating and acquiring CPR skills, because these individual feedback devices require audiovisual attention of the trainees as they perform CPR. Instead of using individual feedback devices in training settings, trainees may receive feedback from their instructors. In this case, trainees may better concentrate on their CPR performances as they get feedback from their instructors since it only requires audio attention of the trainees. Until now, only individual-level CPR feedback devices were available. While instructors may use individual feedback when having an individual trainee, most CPR classes have several trainees receiving CPR training simultaneously, and therefore instructors only provide subjective feedback to their trainees. In this regard, QCPR Classroom device enables an instructor to monitor real-time CPR quality of multiple trainees simultaneously so the instructor can provide real-time objective feedback to those who need. To our knowledge, this study is the first randomized trial investigating the effect of QCPR feedback device on the quality of CPR performances in adult layperson training setting.
Recently, Cortegiani et al. 14 conducted a randomized trial among secondary school students to evaluate the effectiveness of Laerdal Resusci Anne QCPR feedback compared to a standard instructor-based feedback for chest compressions acquisition in training. After a 30-min interactive frontal lesson about basic life support-defibrillation and high-quality chest compressions by a trained instructor, a total of 125 students performed 2-min CPR and received either instructor-based or QCPR-based feedback according to their randomization, 7 days post training. Students in QCPR group showed a significantly higher total compression score (median 90%, IQR 81.9–96.0) compared to standard feedback group (median 67%, IQR 27.7–87.5; p = 0.0003). Regarding individual parameters, they observed a statistically significant difference between the two groups for the rate of chest compressions and percentage of chest compressions with complete release. In our adult layperson population, we also observed significantly higher total compression score, but by lesser magnitude than observed in Cortegiani’s study. The baseline total score for our conventional group was higher than that of Cortegiani’s study (76 vs 67), which suggests that the students in Cortegiani’s study had more room for improvement, therefore could demonstrate a higher difference. Moreover, younger population may have faster learning capability and have better adaptability to instructors’ feedback than older population.
Our study has limitations. First, trainers in this study were not blinded to the study arms. While instructor blinding was not feasible due to the design of the study, we developed study protocol prior to the trial and trained the instructors to abide strictly by the study protocol to minimize the bias. Second, we had three different trainers participating in the trial. There still might have been variability in how they conduct the training and give feedback to the trainees; thus, we adjusted trainer into our model as a random effect in the analysis. Third, there was a difference in the number of trainees trained in each class, which might have influenced the quality of instructor’s feedback. However, there was no significant differences in the median and IQR of number of trainees between QCPR-based (median 10 trainees; IQR 5–16) and conventional feedback (median 10 trainees; IQR 5–17) groups. Finally, our training course was about 1-h long with a total of five CPR sessions with durations of 1.5, 1, 3, 4, and 2.5 min for each of the five CPR sessions, respectively. Throughout the training, trainees felt fatigue, especially during the fourth CPR session where trainees had to perform CPR for entire 4 min. As a result of this, during the last session, trainees may not have performed CPR in their full extent, which could have minimized the effect of instructor’s objective real-time feedback. However, since both groups had same training and CPR durations, any potential minimized effect of instructor’s feedback should be effected non-differentially between two groups.
Conclusion
In an adult laypeople population, a CPR training with real-time objective instructor feedback using a classroom feedback device is more effective than conventional instructor feedback in terms of overall chest compression only CPR skill acquisition. Based on the present findings, further studies are warranted not only to find optimal feedback method for the CPR acquiring skill but also to evaluate the long-term retention of CPR skill after training with real-time objective instructor feedback.
Footnotes
Acknowledgements
The authors thank instructors at the Nowon District CPR Training Center, Hyun Soo Lee, Mi Ryung Lee, and Sarang Song, for their unconditional support on this trial.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. The training equipment used in this study (QCPR Classroom) was supported by the Laerdal Medical, but had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data.
Availability of data and materials
The data of this study are available and can be reanalyzed by authors.
Ethical approval
Research ethics board approval was obtained for this research (IRB number: 1704-179-851).