
Abstract
Purpose
To provide preliminary evidence of the effectiveness of a novel surgical technique using patient-specific 3D-printed titanium prosthesis/autograft composite (3D-PAC) in reconstruction of a large osteoarticular metacarpal defect.
Material and methods
Seven patients (4 women, 3 men; mean age, 30 years; mean follow-up duration, 37.4 months (range, 12-73 months)) with large osteoarticular metacarpal defect who were treated with 3D-PAC reconstruction between January 2018 and November 2024 were included in the study. The etiologies were bone tumors in 4 patients, and open fracture in 3 patients.
Results
At the final follow-up, mean metacarpophalangeal (MCP) extension was 2.1° (range, 0°-10°), and flexion was 52.9° (range, 30°-90°). Mean total active motion of the involved digit was 185.7 (range, 110°-270°) with 3 excellent cases, 3 good cases, and 1 fair case. Mean grip strength was 71.3 % (range, 40%–91%), and key pinch strength was 84.7% (range, 50%–128%) of the contralateral side. Mean visual analog scale score was 0.6 (range, 0-2), Michigan Hand Outcomes Questionnaire score was 70.3 (range, 52.4–83.1), and Disabilities of the Arm, Shoulder and Hand score was 12.9 (range, 4.2–21.7). One patient developed persistent periprosthetic joint infection which required prosthetic removal and converted to arthrodesis. No mechanical complications including aseptic loosening, and implant breakage was revealed. All were satisfied with the function and cosmesis of reconstructive hands.
Conclusion
Patient-specific 3D-printed titanium prosthesis/autograft composite reconstruction appears to be effective in treatment of large osteoarticular defect of metacarpal in a pilot study. Although suboptimal MCP flexion and decreased hand strength were revealed, such joint motion-sparing procedure was useful to achieve satisfactory hand function and cosmesis. Further studies with a larger sample size compared with the conventional treatments are required to validate the benefits of 3D-PAC reconstruction.
Keywords
Introduction
Three-dimensional printing technology is increasingly being used in orthopedics. 1 The 3D-printed prosthesis can be designed to maintain the functional alignment, and the articular section can be precisely contoured to provide the anatomical contact with the corresponding articular surface. 2 A review of current literature demonstrates that patient-specific 3D-printed prostheses achieved consistently good results in several areas of osteoarticular reconstruction. 3 However, the application in metacarpal was published only in a few case reports.4,5
The metacarpals are long bones of the hand which act as the bridge between the carpals and phalanges, forming the framework of the hand. 6 Metacarpal bone defect secondary to neoplasm and trauma always causes significant impairment of the hand function. A large osteoarticular defect of the metacarpal may result in joint instability, malalignment of the finger, and weakness of finger. Reconstruction of such defect is a great challenge for orthopedic surgeons.4,5,7
The arc of motion of the joints in the hand is fundamental for many of the activities of daily living. 8 For this reason, several authors preferred the joint motion-sparing procedures to arthrodesis in treatment of the large osteoarticular defect.5,9 The conventional options of joint motion-sparing reconstruction include osteoarticular metacarpal allograft, osteoarticular metatarsal autograft, vascularized or nonvasculaized bone graft with metacarpophalangeal (MCP) silicone implant arthroplasty, and osteoarticular metacarpal metal prosthesis. Based on the current evidence regarding the outcomes of such interventions, the optimal choice of reconstruction is still debatable. Each method also carries its own risks of complications. The osteoarticular allograft has the high rate of nonunion of the graft-host junction, allograft fracture, deep infection, and subchondral fragmentation with degeneration of articular cartilage whereas the osteoarticular autograft that offers better healing potential is associated the donor-site complications and morbidity.10–12 Mismatch of the joint surface of osteochondral graft and the opposing native joint structure also increases the risk of secondary osteoarthritis. 9 The bone graft with MCP silicone implant arthroplasty was described as a useful joint motion-sparing option.12,13 Whereas the clinical results are acceptable, the complications and longevity of the silicone implant arthroplasty are still a concern. Increased incidence of decreased range of motion, implant fracture, and articular deformity were reported in long-term follow-up of silicone implant replacement. 14 Silicone particulate-induced synovitis may occur if the implant is broken. 15 In addition, the growth plate of proximal phalanx must be removed in growing patient with open epiphyses. 16 The osteoarticular prosthesis has the benefit of avoiding the donor-site complications. However, its poor healing property with the soft tissue sleeve around may be associated with consequent instability or dislocation. 7
In the present study, the alternative reconstruction of a large osteoarticular metacarpal defect using a novel design of patient-specific 3D-printed titanium prosthesis/autograft composite was described. The rationale for using this technique is to combine the advantage of the 3D-printed prosthesis which can replicate the normal anatomy and form the customized framework with autograft which could enhance the bone and soft tissue healing with surrounding structure. The purpose of this study is to provide preliminary evidence of the effectiveness of this reconstruction method.
Materials and methods
This study was approved by the Institutional Review Boards; reference numbers IRBRTA 1625/2567. Between January 2018 and November 2024, a total of 7 patients with large osteoarticular metacarpal defect underwent patient-specific 3D-printed titanium prosthesis/autograft composite reconstruction. The medical record was reviewed for demographic data as well as for preoperative, intraoperative, and postoperative information. All patients were also informed that data regarding their clinical and radiological examinations would be submitted for publication.
Patients
The study group consisted of 4 women and 3 men with a mean age of 30 years at the time of surgery (range, 11–53 years). All were right-hand dominant. The average duration of postoperative follow-up was 37.4 months (range, 12–73 months). The etiology included bone tumors in 4 patients, and open fracture in 3 patients. Four defects were on the right and 3 were on the left hands. Four patients had defects comprising whole metacarpal (total metacarpal defect). Three patients had defects involving the metacarpal head and diaphysis (partial metacarpal defect).
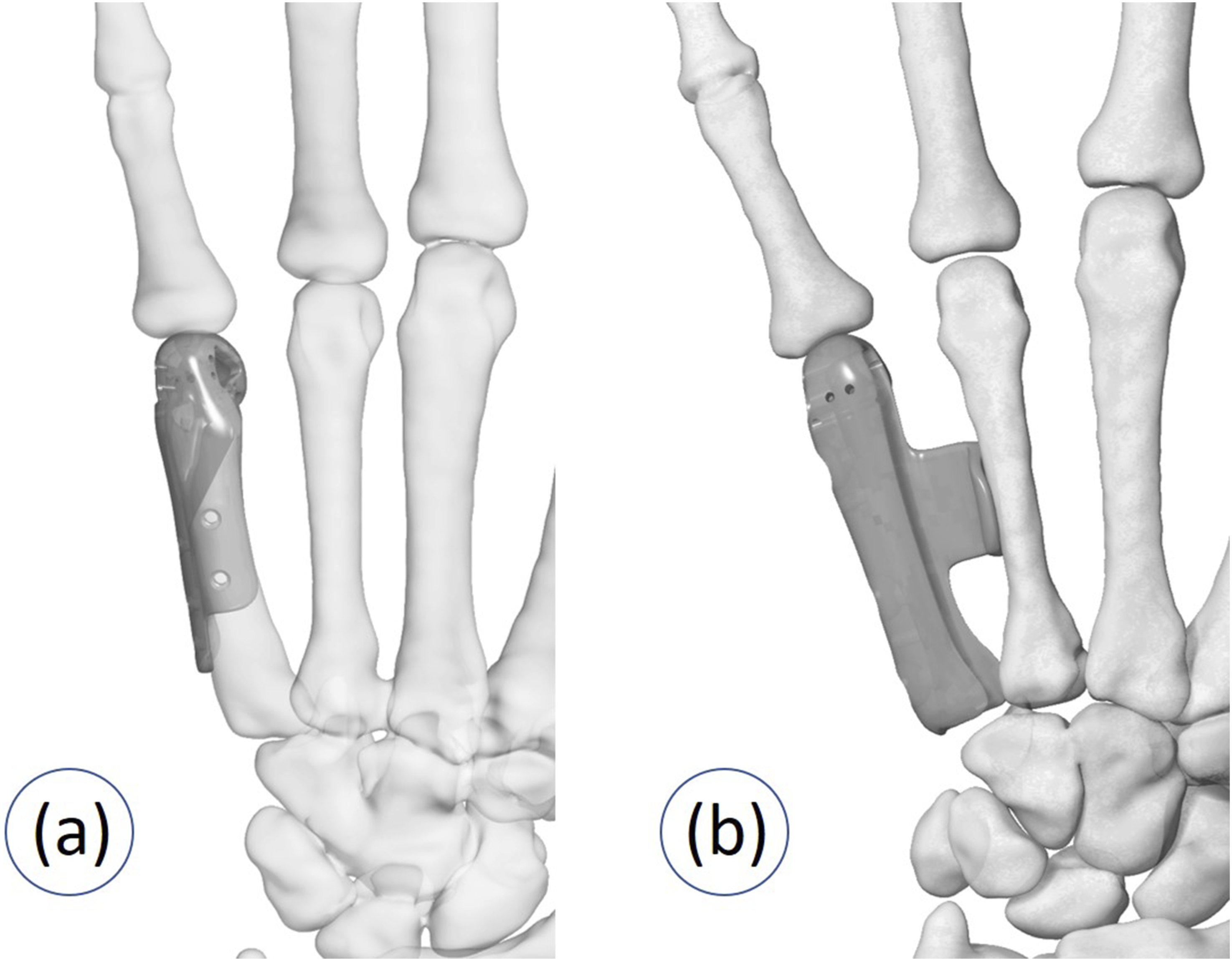
Metacarpal reconstruction was performed according to the extent of the osteoarticular defect. The reconstruction was classified in two patterns as follows (Figure 1). Pattern 1: Partial metacarpal replacement with MCP capsuloligamentous reconstruction Pattern 2: Total metacarpal replacement with MCP capsuloligamentous reconstruction and intermetacarpal arthrodesis Pattern of metacarpal reconstruction (a) Partial metacarpal replacement. (b) Total metacarpal replacement.
Prosthesis design and fabrication
High-resolution CT scanning (Philips Brilliance 64 CT scanner, Cleveland, Ohio, USA; voxel size 0.3 × 0.3 × 0.3 mm, 120 kV, 150 mAs, pitch 0.5) of both hands was performed and reconstructed into 3D images. The 3D implant model was constructed using the image processing techniques and computer-aided design. The surface of rendered 3D model of the normal side was reversed and registered with the affected side to identify the correct profile of the articular surface and evaluate the defect for prosthesis design. In the patient who had a long-standing condition with significant metacarpal shortening, the prosthetic length was reduced to accommodate the defect, optimize the surrounding soft tissue tension, and facilitate adequate soft tissue coverage. The implant design was accomplished with a close collaboration between the surgical team and engineering team.
Prosthesis design in partial metacarpal defect
In this design, the partial metacarpal was replaced while preserving the original proximal bone and CMC joint. The prosthesis consisted of head portion and side plate. The head portion had a hollow body to contain the bone graft inside. The medial and lateral openings were created for attachment of the ulnar and radial collateral ligaments, respectively. Multiple suture holes surrounding the head and its openings were adopted to be used for capsuloligamentous repair with mesh graft augmentation. The undersurface of the side plate was shaped in conforming with the outer surface of remaining metacarpal. Multiple screw holes in the side plate were designed for screw insertion in coronal and sagittal planes (Figure 2). Design in partial metacarpal defect. Prosthesis consisted of head portion (red arrow), side plate (blue arrow), and opening for collateral ligament attachment (white arrow). (a) The lateral aspect. (b) The posterior aspect. (c) The medial aspect. (d) The anterior aspect.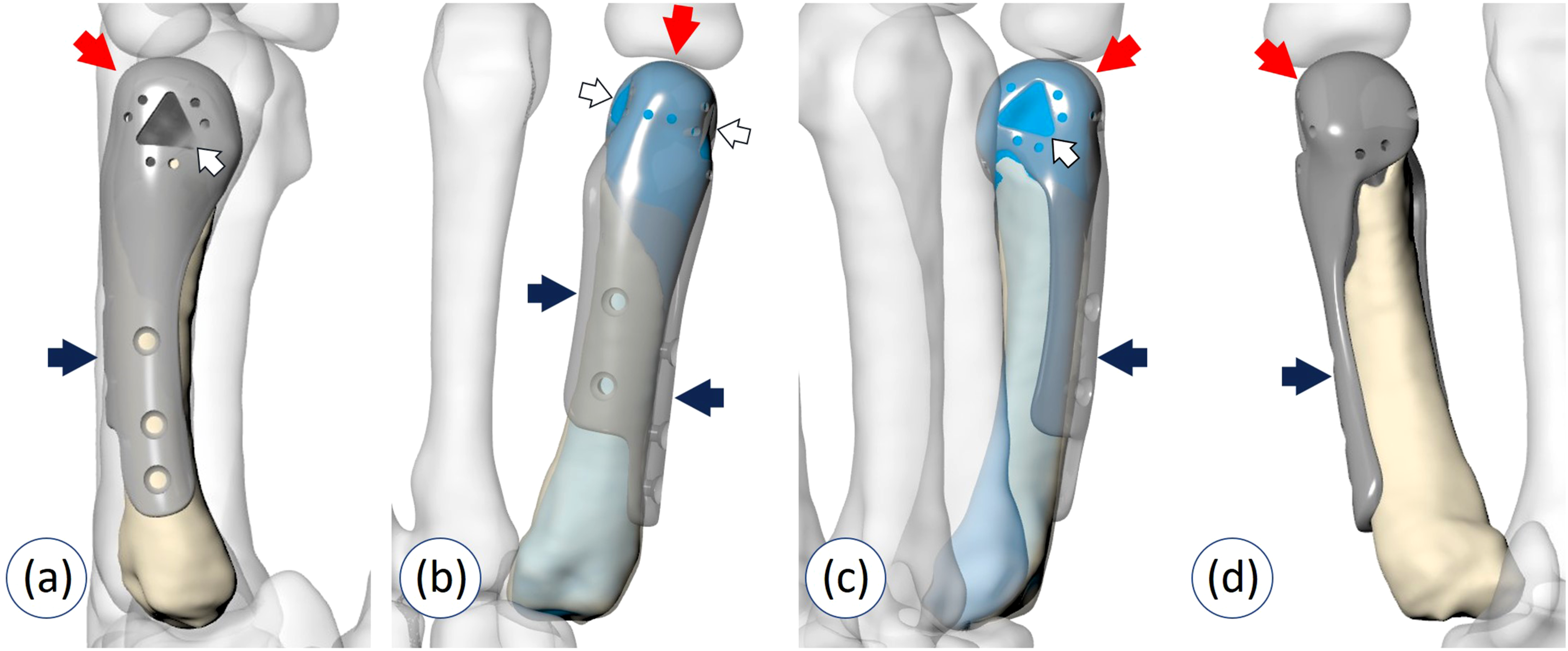
Prosthesis design in total metacarpal defect
In this design, the entire metacarpal was replaced in combination with fusion to the adjacent metacarpal. The first-second, second-third, and fourth-fifth intermetacarpal arthrodesis was planned for the defect of the first, second or third, and fourth or fifth metacarpal, respectively. The implant consisted of head portion, metacarpal body, and side wing. The head portion had the opening and surrounding suture holes to be used for capsuloligamentous repair with mesh graft augmentation. The metacarpal body was designed to have a side opening for containing a strut bone graft. The k-wire and screw holes in the metacarpal body were made for temporary and permanent fixation of the bone graft, respective. The side wing was projected from the ventral edge of side opening in the middle part of the metacarpal body. Its curved lateral end was buttressed on the adjacent metacarpal diaphysis to maintain normal intermetacarpal space (Figure 3). Design in total metacarpal defect. (a) Prosthesis consisted of head portion, metacarpal body with side opening (white arrow), and side wing (yellow arrow). (b) The k-wire holes (blue arrow) and screw holes (green arrow) in the metacarpal body were created for temporary and permanent fixation of the bone graft, respectively.
After the computerized model was accomplished, the manufacturing process was conducted by the engineering organization (Meticuly Co. Ltd, Chulalongkorn University, Thailand) which is ISO 13,485 certified for the development and production of the orthopedic devices. The prosthesis was fabricated from medical grade titanium alloy (Ti-6Al-4V) powder using selective laser melting 3D-printed machine (Mlab cusing 200-R, GE, Germany). Surface of the prosthesis which was contacted with bone graft or patient’s bone was roughened by grit-blasting process using aluminum oxide particles to produce an irregularity at 4-7 microns depth. Cleaning and steam sterilization processes were subsequently performed.
To ensure structural strength of the titanium implant, finite element analysis with ANSYS mechanical software (Ansys Inc., Canonsburg, Pennsylvania, USA) was conducted. Testing and standard compliance including full biocompatibility test according to ISO10993 standards and 3D printing mechanical standards according to additive manufacturing ASTM F3001 were executed.
The surgical guides and anatomic models were fabricated to be used intraoperatively for accurate placement of the prosthesis. The guides and anatomic models were manufactured by layer plastic deposition (LPD) printer (Zortrax, Poland) using certified medical grade material (polyamide) filament. The guides and models were sterilized using low-temperature hydrogen peroxide gas plasma (Sterrad system, Advanced Sterilization Products, Div. of Johnson & Johnson Medical Inc., Irvine, California, USA) prior to surgery.
Surgical technique
Surgical technique in partial metacarpal defect
The metacarpal defect was exposed via the dorsal approach. An anatomic model of affected metacarpal had been used intraoperatively to verify the matching precision and optimal position of the prosthesis. Multiple strands of 2-0 Fiberwire (Arthrex, Naples, Florida, USA) were passed through the peripheral holes surrounding the prosthetic head for subsequent suturing with the capsuloligamentous structures and mesh graft. A 3D-printed surgical drill guide was closely fit on the bony edge of the remaining metacarpal which had been used as a reference. After all trajectories were predrilled into the bone, the guide was removed. The prosthesis was then placed and the 2.7-mm standard cortical screws (DePuy Synthes, West Chester, Pennsylvania, USA) were inserted into the predrilled holes to secure the prosthesis. The cavity between the undersurface of the implant and original fractured bone was completely filled with the cancellous iliac crest bone graft. Medial and lateral collateral ligaments, volar plate, and dorsal capsule were reattached to the prosthetic head using preloaded Fiberwire. A strip of polypropylene mesh (PROLENE™, Johnson & Johnson, Langhorne, Pennsylvania, USA) was placed on top of the reattached structures and wrapped around the head of prosthesis. The mesh was tightened by folded over and sutured to itself using 2-0 Fiberwire (Figure 4). Surgical technique in partial metacarpal defect. (a) The metacarpal defect was exposed via the dorsal approach. (b) An anatomic model of affected metacarpal had been used intraoperatively to verify the optimal position of the prosthesis. (c) A 3D-printed surgical drill guide was closely fitted on the bony edge of the remaining metacarpal to create the screw holes. (d) The prosthesis was placed and the cavity between the prosthetic undersurface and the original fractured bone was filled with the cancellous iliac crest bone graft. (e) The capsuloligamentous structures were sutured to the prosthetic head. (f) A strip of polypropylene mesh was placed on top of the reattached structures and wrapped around the head of prosthesis.
Surgical technique in total metacarpal defect
The prosthesis/autograft composite was prepared for implantation. Multiple strands of 2-0 Fiberwire were passed through the peripheral holes surrounding the prosthetic head for subsequent suturing with the capsuloligamentous structures and mesh graft. The autogenous iliac crest strut graft was harvested, contoured, and placed into the side opening. In the proximal portion, the bone graft was projecting laterally to later contact with the adjacent metacarpal for intermetacarpal arthrodesis. A 1.6 mm K-wire was drilled into the bone graft through each k-wire hole of metacarpal prosthetic body to create the holes. After exposure through dorsal approach, a 3D-printed surgical guide was meticulously fit on the lateral aspect of the metacarpal. Two of 1.6 mm K-wires were passed from the guide holes through the bone. The guide was removed while the K-wires were left in place. Decortication of the recipient graft bed at the proximal portion of the adjacent metacarpal was performed. Each K-wire end was passed through the corresponding pre-drilled hole of the bone graft. The prosthesis/autograft composite was sliding toward the metacarpal. Before the side wing fully contacted with the diaphysis, the proximal portion of bone graft was shaped to properly fit with the recipient bed. After the intraoperative fluoroscopy verification and clinical examination to make sure that the prosthesis alignment was accurate, three 2.4 mm cortex screws (DePuy Synthes, West Chester, Pennsylvania, USA) were inserted from the screw holes of the prosthesis through the bone graft and the metacarpal. The MCP capsuloligamentous reconstruction was performed (Figure 5). Surgical technique in total metacarpal defect. (a) Multiple strands of Fiberwire were passed through the peripheral holes surrounding the prosthetic head for subsequent suturing with the capsuloligamentous structures. (b) The autogenous iliac crest strut graft was harvested, contoured, and placed into the side opening. (c) A 3D-printed surgical guide was fitted on the lateral aspect of the metacarpal and 2 K-wires were passed from the guide holes through the bone. (d) The guide was removed while the K-wires were left in place. (e) The prosthesis/autograft composite was placed by passing each K-wire end through the corresponding pre-drilled hole of bone graft. (f) A strip of polypropylene mesh was placed on top of the reattached structures and wrapped around the prosthesis.
Postoperative management
Postoperatively, the hand was immobilized in a plaster splint. Two weeks after the surgery, the splint was removed, and the patient was transitioned into a removable orthosis and active range-of-motion exercises were initiated. Weight bearing was allowed at 12 weeks postoperatively.
Evaluation
Postoperative clinical assessment, radiographic findings, and complications were reviewed. The clinical assessment included MCP range of motion and total active motion (TAM) of the involved finger, MCP stability test in a fully extended position and 30 flexion compared with the contralateral side, grip strength, key pinch strength, visual analog scale (VAS) score, Michigan Hand Outcomes Questionnaire (MHQ) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, and patient subjective satisfaction. The metacarpal alignment, joint congruity, and incorporation of bone graft were evaluated postoperatively with plain X-rays. Incorporation of bone graft with remaining metacarpal in partial metacarpal replacement was additionally assessed with CT scan at 12 weeks postoperatively because it was blocked from view by metal component of prosthesis on plain radiography. The Osteoarthritis Research Society International (OARSI) atlas was used as a reference for grading radiographic changes of the surrounding joints (MCP and CMC joints). 17 The joint space narrowing (JSN), and osteophytes were scored on 0-3 scales. Subchondral sclerosis, subchondral erosion, and cysts were scored as absent/present. This grading method has been validated and commonly used for progressive assessment in hand osteoarthritis. 18 All parameters were measured by 2 orthopedic surgeons separately. Good inter-rater agreement was demonstrated with Cohen’s kappa values of 0.67–1.0. Discussion for consensus was performed in cases of different opinions. The complications including infection, joint instability, contracture, dislocation, and device-related complications such as periprosthetic fracture, implant loosening or osteolysis were reviewed.
Results
Details of the study group and results at the final follow-up.

F: female; M: male; R: right; L: left; ROM: range of motion; MCP: metacarpophalangeal; TAM: total active motion; VAS: visual analogue scale; DASH: the patient-based Disabilities of the Arm, Shoulder and Hand; MHQ: Michigan Hand Outcomes Questionnaire.
aTAM was calculated the by subtracting the total active flexion of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints from the total extension deficit of the same joints (hyperextension of these joints was disregarded).
bTAM result according to categorical rating scale described by Duncan et al.: (Finger) 220°-260°, excellent; 180°–219°, good; 130°–179°, fair; <130°, poor (Thumb) 119°-140°, excellent; 98°–118°, good; 70°–97°, fair; <70°, poor.
cGrip strength compared with the contralateral side.
dPinch strength compared with the contralateral side.
In partial replacement, mean MCP extension was 3.3° (range, 0°–10°), and flexion was 55° (range, 30°-90°). Mean TAM was 170° (range, 110°–270°). Mean grip strength was 68.7 % (range, 40%–91%), and pinch strength was 90% (range, 67%–128%) of the contralateral side. Mean visual analog scale score was 1 (range, 0–2), Michigan Hand Outcomes Questionnaire score was 67.2 (range, 52.4–76.9), and Disabilities of the Arm, Shoulder and Hand score was 14.2 (range, 10–17.5). In total replacement, mean MCP extension was 1.3° (range, 0°–5°), and flexion was 51° (range, 45°-70°). Mean TAM was 197.5° (range, 115°–260°). Mean grip strength was 73.3 % (range, 55%–90%), and pinch strength was 80.8% (range, 50%–100%) of the contralateral side. Mean visual analog scale score was 0.3 (range, 0–1), Michigan Hand Outcomes Questionnaire score was 72.6 (range, 60.7–83.1), and Disabilities of the Arm, Shoulder and Hand score was 11.9 (range, 4.2–21.7).
Postoperative radiographic evaluation.

MCP: metacarpophalangeal; JSN: joint space narrowing.
aRadiographic assessment using the osteoarthritis research society international (OARSI) atlas as a reference.
Apart from PJI, other complications were not revealed in the present study. In a patient who had PJI, arthrodesis of MCP joint was performed after the infection had successfully been eradicated. No additional bone graft was required for such procedure as the patient had adequate bone stock from the previous reconstruction. Solid fusion was achieved at 8 weeks after the procedure. Analysis of the retrieved implant demonstrated osseointegration of the undersurface prosthesis with the bone graft. The metacarpal replacement in an 11-year-old girl did not show the evidence of premature closure of proximal phalangeal physis of the reconstructive finger.
Representative cases
Partial metacarpal replacement
Open fracture of the right fifth metacarpal (Patient 5)
A 24-year-old male sustained the open fracture of the right fifth metacarpal from a motorcycle accident. The patient received a surgical debridement and referred to our department. Plain X-rays and CT demonstrated a large osteoarticular bone loss of fifth metacarpal with metacarpal head and diaphysis involvement. A reconstructive procedure with partial metacarpal prosthesis was performed at 3 weeks after the injury. At this point, the soft tissue was optimized to allow definite treatment and the surgical area was free of infection and drainage. Early postoperative radiograph showed well contour of the prosthesis with the remnant of metacarpal, and the prosthetic head was well congruent with the articular surface of the proximal phalanx. There was no bone length discrepancy compared with the contralateral normal side, and normal metacarpal oblique line was observed. He was able to return to military duty with heavy hand use. The final postoperative radiographs at 34 months postoperatively showed that the alignment of prosthesis/autograft composite was maintained. Increased JSN was found but the patient exhibited good function of the affected hand (Figure 6). Partial metacarpal replacement in a patient with large osteoarticular bone loss from open fracture of fifth metacarpal (Patient 5). (a) X-rays preoperatively. (b) Incorporation of bone graft with remaining metacarpal was observed from postoperative CT evaluation at 12 weeks. (c) X-rays at 34 months postoperatively. (d) Postoperative images demonstrated appearance and range of motion at the final follow-up.
Total metacarpal replacement with intermetacarpal arthrodesis
Giant cell tumor of the left first metacarpal (Patient 6)
A 53-year-old female with giant cell tumor of the left first metacarpal. Radiographic evaluation showed expansile lytic lesion with soap bubble appearance over the entire fist metacarpal. Bony deformity combined with significant shortening was observed. The patient underwent the en bloc resection and immediate reconstruction with first metacarpal prosthesis combined with first-second intermetacarpal arthrodesis. In this case, the prosthesis was designed to be 9 mm shorter than the normal contralateral side to fit in with the extent of tumor resection. Immediate postoperative X-rays showed prosthesis and screw fixation were in alignment and position as planned preoperatively. The artificial metacarpal head was well articulated with the base of proximal phalanx. At 3 months postoperatively, there was radiographic evidence of bone fusion between the strut graft inside the prosthesis and the second metacarpal. The X-rays at 32 months postoperatively demonstrated maintaining alignment of prosthesis and MCP joint. At the final follow-up, satisfactory surgical outcome and cosmesis was revealed (Figure 7). Total metacarpal replacement in a patient with giant cell tumor of the first metacarpal (Patient 6). (a) X-rays preoperatively. (b) X-rays at 32 months postoperatively. (c) Postoperative images demonstrated appearance and range of motion at the final follow-up.
Chondrosarcoma of the left fifth metacarpal (Patient 4)
A 22-year-old female with chondrosarcoma of the left fifth metacarpal. Radiographs and MRI revealed an expansile osteolytic lesion involving the entire length of the metacarpal. Following the en bloc resection, immediate total fifth metacarpal replacement with fourth-fifth intermetacarpal arthrodesis was performed. The follow-up radiography at 3 months after surgery showed that the prosthesis was in a good alignment. The anatomy of the fifth metacarpal was well-restored with well congruity of MCP joint. Incorporation of bone graft at the recipient site was revealed. The follow-up X-ray at 36 months postoperatively demonstrated the prosthetic alignment was maintained. At the final follow-up, although the range of motion and strength was diminished compared with the normal side, the patient was still satisfied with the cosmetic and functional outcomes. Motion at the fifth CMC joint was noted with the hand movement (Figure 8). Total metacarpal replacement in a patient with chondrosarcoma of fifth metacarpal (Patient 4). (a) X-rays preoperatively. (b) X-rays at 36 months postoperatively. (c) Postoperative images demonstrated appearance and range of motion at the final follow-up.
Discussion
This study reported the outcome of composite biological reconstruction using a novel design of patient-specific 3D printed titanium prosthesis and autograft in treatment of a large osteoarticular metacarpal defect. Satisfactory results were obtained in all excepts one who need the prosthetic removal due to PJI.
Management of a large osteoarticular metacarpal defect remains challenging as reconstruction of both bony structure and MCP joint are essential to restore the function and cosmesis of the involved finger.5,9 Amongst the conventional reconstruction methods, bone graft with MCP silicone implant arthroplasty was the most popularly reported. However, the information regarding the outcomes of such option is limited and only published in the case reports.13,20–22 Based on our literature review, inconsistent operative outcomes were revealed. The functional assessment, grip strength and pinch strength of this type of reconstruction were not available. Athanasian et al. demonstrated that the postoperative MCP range of motion was half that of a normal joint in two patients who had giant cell tumor of metacarpal bone. 20 Jones et al. reported the 15°- 85° of MCP motion; however, radial displacement of the proximal phalanx and subsidence of the silicone implant into the fibula was observed on the follow-up radiograph. 13 Generally, silicone implant is not recommended for patients with high mechanical demands on their hand as it would not have withstood intense stresses from forceful pinching and grasping. 23 Biomechanical analysis indicated that increasing joint flexion range will be rising the stress levels and the pistoning motion on the implant, ultimately contributing to the less longevity of silicone arthroplasty. 24 Recently, the replacement with patient-specific 3D printed titanium prosthesis was proposed as an alternative reconstructive option.4,5,7
Based on the symmetry of the human skeleton, the 3D images of the normal side can be reversed to manufacture the prosthesis which has the accurate shape and dimension for the contralateral side. 25 In addition to anatomic restoration of the metacarpal head portion, reconstruction of the capsuloligamentous structure is necessary to enhance joint stability and function.4,5,26 In this work, the 3D-printed prosthesis was designed to provide the anatomical reattachment of the MCP ligaments and capsule with the peripheral holes surrounding the prosthetic head. In addition, the medial and lateral openings allowed the collateral ligaments to contact with the underlying bone graft. To our knowledge, there are no data available regarding the physiological process of ligament healing to 3D-printed prosthesis and the consistency of the repair. Therefore, further investigation is needed. Augmentation with the synthetic mesh has been proposed to reinforce the capsuloligamentous repair.27–29 A biomechanical study verified that use of polypropylene mesh augmentation increased the ultimate failure load of the repair. 28 A clinical study of proximal humeral prosthetic replacement found that the patients who had reconstruction with synthetic mesh had more stable joints and better function than those without mesh. 29 In the present study, stable MCP joint was obtained following a similar reconstructive technique in 6 of 7 patients.
In partial reconstruction of the tubular bones of the hand, the 3D-printed prosthesis with an intramedullary stem is a commonly used design pattern.4,7 Although the favorable outcome was reported, the potentially problematic mechanical complications in this type of prosthesis is concerning. 7 The small stem may be susceptible to the stem fracture whereas the large stem which requires additional removal of the inner cortical bone of the medullary canal may increase the risk of periprosthetic fracture.30,31 A prosthesis for a large osteoarticular defect which results in reduction of the stem length may lead to high strains around the stem that increase the risk for aseptic loosening. 32 In the present study, the cementless prosthesis has been utilized in the reconstruction. The extramedullary fixation system has been designed instead of the intramedullary stem to avoid the aforementioned problems, increase bone stock, and act as a framework for permanent fixation through osseointegration. The prosthesis had a hollow body to be filled in with the autograft, and a side plate which was secured to the remaining bone of metacarpal. The undersurface of the prosthesis was grit-blasted to induce the osseointegration. Structural strength of the implant and sufficient primary stability for successful integration was computerized assessed preoperatively with the finite element method. Satisfactory clinical and radiographic outcomes of the 3D-printed titanium implant with similar design was demonstrated in the distal humerus. 33 In the present study, incorporation of bone graft with remaining metacarpal, and osseointegration of the undersurface of retrieved implant with bone graft was evidenced. No mechanical complications including aseptic loosening, and implant breakage was revealed.
In reconstruction of the entire metacarpal defect, the use of a 3D-printed total metacarpal prosthesis was previously reported in treatment of a giant cell tumor of bone of the first metacarpal. 5 Such prosthesis was solid with multiple holes in the proximal and distal portions for the ligament reconstruction and temporary fixation. Satisfactory functional outcome at 24-months follow-up was observed; however, the proximal migration of the prosthesis which may be related to the CMC instability was found.
Reconstruction of the proximal portion of metacarpal which is a component of CMC joint is challenging. A wide range of surgical options was described. 34 In the present study, intermetacarpal arthrodesis was performed. Intermetacarpal arthrodesis was described as an effective and reliable technique in treatment of irreparable articular surfaces with considerable adjacent extra-articular bone loss from traumatic and oncologic causes of the thumb and other fingers.35–37 Meraghni et al. reported good functional outcomes of the fourth-fifth metacarpal fusion. 36 This procedure preserves some CMC motion with the range of motion in flexion-extension varied from 10° to 20°, thus providing partial adaptability of the palm when gripping. In the radial CMC joints, which are less mobile than the ulnar side joints, Wu et al. observed the acceptable results of the second-third metacarpal fusion in treatment of bony loss from gunshot injury. 35 In the thumb CMC joint, Taleghani et al. revealed the satisfactory outcomes of the first-second metacarpal fusion. 37 It maintains the thumb in a position of maximal function which is able to participate in power grip and pinch. High union rate of first-second metacarpal fusion was found, in contrast to the trapeziometacarpal fusion which has the nonunion rates ranging from 5% to 30%.37,38 In this study, bone union of intermetacarpal arthrodesis was achieved in all patients who had the total metacarpal reconstruction.
Although more invasive procedure which compromised CMC motion was performed in treatment of total metacarpal defect, the MCP range of motion and functional outcomes between partial and total reconstructive groups appeared to be comparable. Potential biomechanical consequence from motion loss following intermetacarpal fusion in total replacement is the overloading of adjacent CMC joints which could lead to pain, inflammation, stiffness, and subsequent osteoarthritis. 35 In this research, radiographs confirmed the absence of carpometacarpal arthropathy at the final review. This result is consistent with previous published data of long-term outcome in intermetacarpal arthrodesis. 39
In order to achieve the ideal position of the prosthesis, a 3D-printed implant guided system was developed. The 3D-printed guide has been used to accurize the insertion of k-wires and screws through the prosthesis for levelling and aligning as planned. 40 It was designed to apply on the distinct bony landmarks of the remaining metacarpal in partial reconstruction and the adjacent metacarpal in total reconstruction. The prosthesis was fabricated to have the side wing in total reconstruction and side plate in partial reconstruction in full contact with the underlying cortical surface. These structures not only allow improved stability and osseointegration by adding more contact area between prosthesis and bone but also enhance precisely position of the prosthesis from their conforming surface. 33 In the patient who preexisting shortening, the prosthetic length was reduced to facilitate prosthesis insertion and soft tissue coverage. The replacement was successful and a favorable clinical outcome was obtained.
Metacarpophalangeal joint acts as the most important joint for hand function. It is the starting point for the complex movements involved in gripping objects and contributes 77% of the total arc of finger flexion. 41 Based on a previous study, the MCP joint’s functional range of motion (fROM) of the thumb and four ulnar fingers was 10–32° and 33–73 degrees of flexion, respectively. 42 Although many patients in the present study did not gain fROM of MCP joints, all but one had good to excellent outcomes according to TAM rating scale. In the present study all cases are right-handed. Previous investigations have demonstrated that right-handed persons were 0%–15.8% stronger in grip strength on the dominant side. 43 Despite decreased hand strength beyond the reported range, all patients were satisfied with the hand function. This is possibly because if the strength required was not more than the threshold, the patients would still be able to perform their tasks. Several studies revealed that the hand function in daily activities often rely on not only the grip strength but also the ability to manipulate objects, the range of motion, and the ability to overcome resistive force.44,45 In this study, 4 patients with bone tumors who had the normal MCP joint space on the X-rays preoperatively demonstrated Grade 1 JSN at the initial follow-up. We hypothesize that the alteration in a short period occurred because the radiographically invisible cartilaginous surface of the original metacarpal head which its thickness typically ranges from 0.36 to 1.10 mm was replaced with the titanium surface of prosthesis. 46 Grade 1 JSN of MCP joint was also presented on the initial postoperative X-rays in 3 patients with open fracture; however, the preoperative joint space could not be assessed due to the osteoarticular bone loss. No progression of JSN was detected on the postoperative follow-up radiographs in all bone tumor cases. In contrast, worsen JSN in 2 patients who had the open fracture was observed. This possibly initiated by the cartilage damage from the injury. Grade 1 osteophyte and subchondral erosion was revealed on the final radiographs in 2 and 3 cases, respectively. Presence of these radiographic features were not correlated with decreased range of motion and functional deterioration in the follow-up period. However, longer monitoring of the development of arthritic condition is required. In case of progression to the end-stage arthritis which requires revision, conversion to the total MCP arthroplasty is planned. Resurfacing of the proximal phalanx using prosthesis with high-density polyethylene component or MCP silicone implant arthroplasty combined with strut bone graft in replacement of the 3D printed titanium prosthesis could be the management options to preserve motion of MCP joint. 47
Complications associated with the use of 3D-printed titanium prostheses in the hand such as infection, dislocation, contracture of joint, spontaneous fusion, and implant failure were described. 7 In the present study, PJI occurred in one patient who sustained the blast injury. The precipitating wound contamination with extensive soft tissue and bony injury could lead to postoperative infection. Solid fusion of MCP joint was obtained after staged revision, first eliminating the infection and subsequent treating with arthrodesis.
This study has several limitations. A small sample size with heterogeneity in etiology and defect extent limit the generalizability of the findings. The lack of direct comparison with the conventional operative options such as bone graft with MCP silicone implant arthroplasty or osteoarticular allograft prevents assessment of whether the proposed technique is superior or inferior. The absence of long-term follow-up and complication data restricts conclusions about the prosthesis’s long-term durability. To validate the benefits of such novel reconstruction technique, further studies in each specific condition with a larger sample size compared with the conventional treatments are required.
Conclusion
Patient-specific 3D-printed titanium prosthesis/autograft composite reconstruction appears to be effective in treatment of large osteoarticular defect of metacarpal in a pilot study. Although suboptimal MCP flexion and decreased hand strength were revealed, such joint motion-sparing procedure was useful to achieve satisfactory hand function and cosmesis.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.