
Abstract
Objective
To explore the diagnostic value of MR T2 mapping in monitoring and evaluating the rabbit vertebral model with Echinococcus multilocularis infection.
Materials and methods
24 New Zealand white rabbits were randomly divided into the experimental group (n = 16), saline control group (n = 4), and blank control group (n = 4). The experimental group underwent surgery to drill holes on the surface of the spinous process of the 12th thoracic vertebra, fill it with a gelatin sponge, and adsorb multilocular hydatid suspension. The saline control group received an operation with saline, and the blank control group did not receive any intervention. The model rabbits were dynamically evaluated by routine MRI and MR T2 mapping once a month after surgery, 6 times. Two rabbits with positive imaging results were randomly selected every 2 months for histopathological examination to evaluate the severity and pathological features of the rabbit model with Echinococcus multilocular infection.
Results
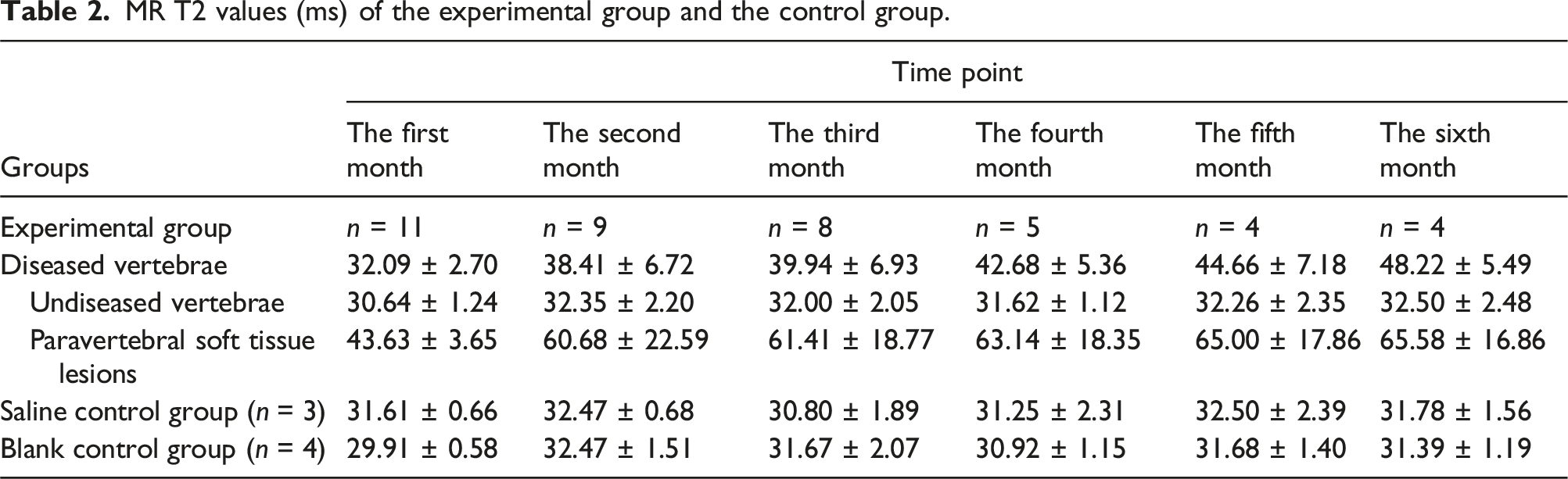
There was no significant difference in the T2 mapping values between the diseased vertebrae and the undiseased vertebrae in the experimental group at the 1st month after surgery (t = 1.7, p = .119), and the differences were statistically significant at the 2nd to 6th month after surgery (p < .05). In the 1st and 2nd months after an operation, there was no significant difference in T2 values between the vertebrae of the saline control group, the blank control group, and the experimental group. In the third, fourth, fifth, and sixth months after surgery, the vertebrae of the experimental group were compared with that of the saline control group and the blank control group, and the difference was statistically significant (p < .05). There was no significant difference in T2 mapping values every month after surgery between the saline control group and the blank control group (p > .05).
Conclusion
The MR T2 mapping technique can quantitatively evaluate the changes of vertebral alveolar echinococcosis, and it shows sensitivity to pathological changes in vertebrae prior to detectable damage using conventional MRI; this offers potential for early detection of vertebral alveolar echinococcosis.
Introduction
Echinococcosis is a common and severe zoonotic parasitic disease reported worldwide. 1 Echinococcosis refers principally to two severe zoonotic tapeworm diseases, cystic echinococcosis (CE) and alveolar echinococcosis (AE), caused by Echinococcus granulosus and Echinococcus multilocularis, respectively. 2 Both CE and AE are major public health issues worldwide. They heavily impair the patients, especially AE, with a mortality rate of about 90% within 10 to 15 years of diagnosis if the patients are untreated or treated inadequately. 3 The highly endemic areas of AE are in various climate zones of the northern hemisphere, including Europe, Asia, Africa and North America. The global burden of AE is estimated to be 18,200 cases per annum, which results in approximately 666,000 DALYs (37 DALYs per case). 4 In more than 95% of cases of AE, the major organ involved is the liver; extrahepatic involvement is rare.5,6 Bone lesion accounts for 0.5% to 4.0% of all echinococcosis lesions and since bone cystic echinococcosis (CE) caused by Echinococcus granulosus is the most common form of bone echinococcosis clinically and bone AE is much rarer. 7 Because of AE’s rare occurrence, lingering course, and diverse symptoms, vertebral AE is difficult to diagnose, and a relevant diagnostic delay often occurs. These are the reasons why vertebral AE is rare. As the number of immunocompromised individuals increases, the disease may become more common.8,9
X-ray findings of vertebral AE are nonspecific. 10 Computed tomography (CT) and its 3D reconstruction technology can accurately evaluate this disease’s bone destruction, calcification, and pathological fracture, and provide more information for the anatomic localization of the lesions. The CT findings of vertebral AE are similar to those of vertebral tuberculosis and metastatic tumors, and are easy to misdiagnose. 11 Magnetic resonance imaging (MRI) can play a crucial role in the differential diagnosis of the two. However, MRI has the most important diagnostic value for vertebral AE. 11 With the rapid development of MRI examination technology, quantitative techniques of MRI have been increasingly studied in the diagnosing diseases. As a non-invasive multi-echo sequence that can reflect the microscopic changes at the molecular level of biological tissue, the MR T2 mapping sequence can not only directly observe the signal changes of lesions, but also determine the T2 mapping value of the lesion area, and quantitatively analyze the lesion area by obtaining the water content of the vertebrae. 12 In addition, T2 mapping pseudo-color maps allow direct observation of morphological abnormalities in articular cartilage and signal abnormalities in bone marrow from structural morphology imaging through changes in color scale. Because T2 mapping values are more sensitive to tissue anisotropy (e.g., collagen matrix alignment), changes in collagen fiber density and water content, T2 mapping sequences are more often used to detect damage and degeneration of cartilage, 13 lumbar intervertebral disc degeneration,14,15 etc. Still, there are fewer studies for the diagnosis of vertebral AE. In this study, MR T2 mapping was used to evaluate and analyze the vertebrae of rabbits infected with AE.
Materials and methods
Fabrication and grouping of a rabbit vertebral model of AE
The experimental animal center of Xinjiang Medical University provided 24 New Zealand rabbits (experimental animal license number: SYXK (new) 2018-0003), aged 10 to 12 weeks, both male and female, with the body weight of (2.6 ± 0.2) kg, randomly divided into three groups. Anesthesia was administered with Sutai + Sumian at 1:1 intramuscular injection. Experimental group: a total of 16, drilled holes at the body surface marking of thoracic 12 spines, filled with gelatin sponge and adsorbed with 0.4 mL/each of Echinococcus multilocularis suspensions; Saline control group (sham-operated group): a total of 4, drilled holes at the body surface marking of thoracic 12 spines and injected with 0.4 mL/each of saline; A total of four rabbits were in the blank control group, and they did not receive any intervention.
MRI scanning
MRI sequences and parameters.

The New Zealand rabbits used in the experiment were examined by MRI once a month after surgery, 6 times.
Image processing
Using the Function Tool two software on the post-processing workstation, we automatically selected a region of interest (ROI) with an area of 60 mm2 on the T2 mapping and generated T2 values. The ROI was placed in the middle three layers, where the lesion showed the best. Then, the average value of T2 was obtained 3 times, and the diseased vertebrae, undiseased vertebrae, and paravertebral soft tissue lesions were repeatedly measured with the experimental group. The ROI of the three levels with the most uniform and continuous vertebral signal strength was selected in the saline control group and the blank control group.
Histopathological examination
Every 2 months, two rabbits were randomly selected for histopathological examination based on the rabbits with positive findings on imaging. Firstly, the rabbits were euthanized, routinely shaved, the skin was exposed, and the tissue specimens in the lesion vertebrae, adjacent upper and lower vertebrae, and surrounding soft tissues were taken out, fixed in 10% formaldehyde, routinely embedded in paraffin wax, cut in 5 mm sections, stained with HE, and sectioned. The Echinococcus multilocularis infections of the specimens and their specific pathological changes were observed in the light microscope.
Statistical analysis
Data were statistically analyzed using GraphPad Prism 10.0 and SPSS 26.0 software. When the p value is less than or equal to 0.05, we consider the distinction statistically significant. T2 values of each group were tested for normality using the Shapiro-Wilk test. We performed a normality test for the difference of T2 values between diseased and undiseased vertebrae in the experimental group, using the Paired Samples t test and Wilcoxon paired signed rank test to compare the differences, respectively. We performed a Normality and Homogeneity of variance test on the T2 values of the vertebrae in the saline control group and the blank control group with diseased vertebrae in the experimental group. One-way analysis of variance (ANOVA) and the Kruskal-Wallis H test were used to compare the differences among the three groups. If the difference between the three groups was statistically significant (p < .05), followed by the Dunn procedure with Bonferroni correction to account for differences between the groups.
Results
Routine MRI
The imaging changes of rabbits’ vertebrae infected with AE in the experimental group from 1st to 6th month after surgery are shown in Figure 1. In the experimental group, there was no bone positive manifestation in the first month after the operation. Still, the paravertebral soft tissues showed low or equal signal on T1WI, and the fat inhibition images on T2WI showed high signal vesicles with aggregation “grape-like” (Figure 1(a)). In the 2nd month, enlarged vesicles still show long T2 signals, and the vertebral body is patchy, with slightly longer T1 prolonged T2 signals of bone marrow edema (Figure 1(b)). In the third month, the lesion enlarged, a soft tissue mass formed, a hyperintense T2 signal was observed, and small vesicles was scattered around it (Figure 1(c)). In the 4th month, the bone was destroyed, and the signal intensity of the destroyed area was mixed; calcifications and dead bone could be seen. On T2WI fat-suppression imaging, the vertebrae showed nodules and patchy, slightly high signals (Figure 1(d)). In the fifth and sixth months, the extent of bone destruction and soft tissue mass increased, the spinal canal narrowed, the spinal cord was compressed to varying degrees, and the central canal of the spinal cord was dilated above the lesion level (Figure 1(e)). In the saline control group, there was no abnormal change in the vertebrae of the rabbits, and a slight high-density surgical scar was observed in the surrounding soft tissue. The results of the blank control group were negative. Changes in MR sagittal T2-trim images of rabbits’ vertebrae infected with AE in the experimental group from 1st to 6th months after surgery. (a) “grape-like” high-signal vesicles in the paravertebral soft tissue; (b) The small vesicles became larger and increased, and the vertebra showed small patches with slightly higher signal; (c) Soft tissue mass formation; (d) Bone destruction and patchy high signal were observed in the vertebrae; (e) Visible bone destruction and increased soft tissue mass.
MR T2 values
MR T2 values (ms) of the experimental group and the control group.

Comparison of T2 values of the experimental and control groups from 1st to 6th months after surgery. Note: * represents p < .05; ** represents p < .01; ns represents p > .05; the difference is not statistically significant.

The trends of T2 values of diseased vertebrae, undiseased vertebrae, and paravertebral soft tissue lesions in the experimental group from 1st to 6th months after surgery.
Pathological manifestations
In the 1st to 2nd months after surgery, vertebrae infection Echinococcus multilocularis experimental rabbit microscopy showed that the bone matrix was still present, with peripheral calcium salt deposits, and many multinucleated giant cells were seen. Necrotic worm eggs were seen in the soft tissue, and many inflammatory cells such as eosinophils were seen around. In the 3rd to 4th month after surgery, bone destruction was seen microscopically; AE internal capsule with calcification was seen in the bone tissue, surrounded by granuloma formation and fibrous tissue hyperplasia, and partially visible formation of calcium salt crystals. In the 5th to 6th month after surgery, multiple vesicle-like structures were observed in the bone tissue, and the walls of the vesicles were cuticular structures with uniform pink staining. Dust-like calcification and large necrosis were observed in the necrotic area around the vesicles. A large number of inflammatory cells infiltrated the periphery, and the new and old lesions coexisted.
Discussion
Bone echinococcosis is rare, with the vertebrae and pelvis being the most common sites of bone involvement.7,16 The severe clinical symptoms and high recurrence rate of the spinal AE cause great distress to patients. The need for more specificity of early clinical symptoms and the low awareness of clinicians of the disease often lead to initial misdiagnosis. The New Zealand White Rabbit has a skeletal system and vertebral structure similar to the human body. 17 There were several studies of spinal diseases using the rabbit model.18,19
The vertebral AE is the hematogenous transfer of Echinococcus multilocularis to germinate and multiply in the cancellous bone of the vertebrae and attachments, and grow along the trabecular space with little resistance, destroying the trabeculae and the bone cortex, as well as invading the paravertebral and peripheral soft tissues. 20 The image of vertebral AE shows osteolytic bone destruction, peri-lesional bone hyperplasia, sclerosis, and common irregular calcification in the lesion area. Fibrosis, calcium salt deposition, and pathological fracture occur after the progression of the lesion.7,21,22 The paravertebral area often forms an irregular and invasive soft-tissue mass poorly demarcated from the surrounding structures. 23 CT has a significant advantage in detecting minor bone destruction, the site and degree of vertebral involvement, and the presence or absence of dead bone. In the early stage of lesions or when the bone destruction is not significant, MRI is superior to CT in detecting lesions.24,25 With the development of MRI technology, quantitative technology has become more and more mature, and its superiority lies in the fact that it is less affected by the diagnostician’s subjectivity, and it can tap into the information of histopathological changes so that it has higher accuracy for the diagnosis of diseases.26,27 There are few reports on the use of T2 values in vertebral AE. In the current experiment, we used a spinal model of a New Zealand rabbit infected with Echinococcus multilocularis to explore the changes in T2 values of rabbits’ vertebral AE over time, and obtained the early evolutionary pattern of vertebral AE, which proved that the T2 mapping technique could quantitatively assess the changes in tissue composition within the vertebral AE, and has certain guiding significance for its diagnosis and differential diagnosis.
In clinical practice, T2 mapping is currently limited by time costs. Firstly, the scanning sequence takes a relatively long time. Secondly, after scanning, MRI technicians need to manually segment the region of interest (ROI). To reduce time costs and further minimize errors (i.e., human errors), making it practical and reproducible in actual operations and normal clinical workflows, it is necessary to achieve automated segmentation and analysis processes. This includes developing algorithms that can accurately identify and segment regions, as well as tools that can automatically calculate T2 values. Additionally, a standardized post-processing procedure needs to be established to ensure consistency and comparability of results among different research centers. With continuous technological advancements and in-depth research, we have the potential to overcome these limitations and make T2 mapping a powerful tool in clinical practice.
The pathologic changes determine the basic pattern of bone destruction characterized by clusters or diffuse “honeycomb-like,” “grapelike,” and cystic bone destruction. Detecting high signal vesicles in the damaged vertebral body and paravertebral soft tissue on T2WI fat suppression imaging is helpful for qualitative diagnosis.24,28 Routine MRI can detect changes in vertebra signal and morphology, which are usually qualitative. However, MRI T2 mapping techniques can help to visualize and quantitatively obtain the water content of the vertebra. 12 The essence of AE is a delayed hypersensitivity reaction of the host secondary to the parasite, with the formation of granulomas of varying sizes around the vesicles, whose pathology is characterized by massive fibrous connective tissue hyperplasia and inflammatory cell infiltration. These pathological changes can lead to disruption of cell membranes and cause changes in tissue water content. The study showed a statistically significant difference in T2 values between the diseased vertebrae and the undiseased vertebrae in the experimental group in the 2nd to 6th months after surgery. The change in T2 value can be detected on the T2 mapping sequence when the bone marrow cells only undergo functional changes. There are no positive signs on the routine MRI. It helps detect bone changes early for diagnosis and treatment. In this study, the bone marrow T2 values of the lesion vertebrae in the 3rd to 6th months were higher than that of the corresponding vertebrae in the saline control group and the blank control group, respectively. The reason may be that when Echinococcus multilocularis spreads to the vertebra by blood circulation, it dissolves the replacement bone tissue, and erosion of the vertebral blood vessels can lead to vertebral ischemic necrosis. The leakage of cystic fluid from the small vesicles of the encapsulated worms leads to the metamorphic reaction of the bone tissues, 29 and all of these changes can cause a prolongation of the T2 relaxation time, and an increase in the T2 values. In addition, because the blood supply of soft tissues is richer than that of the vertebra, the bone tissue structure is dense and hard, with narrow trabecular spaces. It is easier for Echinococcus multilocularis to grow in the soft tissues and the course of the disease progresses more rapidly. Degeneration and necrotic liquefaction of the tissue around the vesicles often occurred, resulting in a significant increase in the tissue’s protein and water molecule content, so the highest T2 values were measured at the paravertebral soft tissue lesions in this study.
The T2 values of paravertebral soft tissue lesions increased significantly from (43.63 ± 3.65) ms to (60.68 ± 22.59) ms in the 2nd month after surgery. The reason may be that the degree of soft tissue infection in the experimental group was less severe in the first month after surgery, and the routine MRI results showed that only a tiny number of high-signal “small vesicles” appeared in the soft tissues. The extent of erosion of the soft tissues by Echinococcus multilocularis was smaller. The paravertebral soft tissue infection rate was 54.55% (6/11). In the 2nd month, the number of vesicles increased with time. The paravertebral soft tissue infection rate increased to 81.81% (9/11), and the T2 values increased to (60.68 ± 22.59) ms. The slow and slight increase in T2 values in the 3rd to 6th months after surgery suggests that as the lesion progresses, necrotic liquefaction may occur in the central region of the lesion leading to an increase in T2 values. There was little trend in the T2 values of undiseased vertebrae.
The limitations of this study mainly contain the following points: I. The number of experimental samples was small, and future studies with large samples and clinical explorations are needed. II. The T2 mapping technique is a powerful tool for quantitative analysis, but it still suffers from inter-observer bias because there is no international standard for handling data obtained from sequences. 30
In conclusion, T2 mapping technology can quantitatively evaluate the changes in vertebral AE, which has a certain guiding significance for the diagnosis and monitoring of this disease.
Footnotes
Author Contributions
Hui Guo conceived the idea. Jinhuan Han wrote the main manuscript text. Yushan Chang collected the data. Jinhuan Han and Yushan Chang performed the literature search. All authors reviewed the manuscript. All authors approved the final version for submission.
Euthanasia methods
The euthanasia of rabbits in this experiment was performed by overdose injection anesthesia. By means of experimental rabbit ear margin vein injection of 3% sodium pentobarbital, the dose of 90 mg/kg, death within about 15 minutes. Non-inhalation anesthesia refers to the rapid injection of an excessive amount of anesthetic to rapidly suppress the respiratory center and heart beat, so that the animal dies quietly. Barbiturates (mainly pentobarbital sodium) are the preferred method of rabbit euthanasia recommended in the American Veterinary Medical Association guidelines.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors gratefully acknowledge the financial support provided by the State Key Laboratory of Pathogenesis, Prevention, and Treatment of High Incidence Diseases in Central Asia Fund (Grant No. SKL-HIDCA-2024-BC6).