
Abstract
Purpose:
We have always used the standard anatomical landmark vertebrae to measure the sagittal alignment. Instead, scoliosis has been evaluated by the end vertebrae in the coronal plane. There have been clinical studies to investigate sagittal alignment on the end vertebrae of inflection points (IPs). The purpose is to determine sagittal alignment based on IPs and to elucidate the changes while considering age groups.
Methods:
We identified the most titled vertebrae in the sagittal plane to define the end vertebrae of S1, thoracolumbar and cervicothoracic IPs and to measure the Cobb angles of sacral slope, functional lumbar, thoracic, cervical segment between them, and the McGregor’s line, and the IP distances from the C2 plumb line to the point bisecting the upper end plate of the IPs, in addition to S1.
Results:
The most common thoracolumbar and cervicothoracic IPs were L2 and T1, respectively. However, the next most common cervicothoracic IP changed from T2 in the youngest to C7 in the oldest age group. The sagittal angles decreased at the sacral slope and functional lumbar segment but not the functional thoracic segment and functional cervical segment. Similarly, the distance increased at the C2 sagittal vertical axis (SVA) distance to S1 and thoracolumbar IP distance but not at the cervicothoracic IP distance. There was no difference in the pelvic incidence among age groups.
Conclusion:
The sagittal Cobb angles based on the IPs decreased at the sacral slope and functional lumbar segment in the older adults. Consequently, the C2 SVA distance to S1 and thoracolumbar IP distance increased.
Introduction
The sagittal alignments of the spine are significantly different according to age, sex, weight, and ethnicity. 1 –5 A wide variation in thoracic kyphosis and lumbar lordosis was found in healthy adults. 6 For example, the variation in thoracic kyphosis from T3 to T12 is from 9° to 53° in normal populations, 6 and the variation in lumbar lordosis from L1 to L5 is from −14° to −69° in normal populations. 6 These cervical, thoracic, and lumbar spine measurements were based on an anatomic classification and not on functional aspects.
Anatomic sagittal alignments might lead to conflicting results about the influence of sagittal alignments on clinical outcomes after spinal surgeries. 7 –14 In addition, the unexpected cervical sagittal malalignments were developed, and cervical sagittal alignment did or did not improve after surgeries dealing with thoracolumbar deformities. 15,16 These might suggest that the anatomic sagittal alignment has a limitation.
Instead of using anatomic sagittal alignment, the sagittal Cobb angles based on the end vertebrae and inflection points (IPs) might be useful for functional evaluation and preoperative planning for spinal deformity, which are similar to the coronal Cobb angles based on the end vertebrae in patients with scoliosis. Berthonnaud et al. 17 and Roussouly et al. 18 performed pioneering studies to evaluate functional sagittal alignment based on the IP between lordosis and kyphosis. However, there has been no report to elucidate the sagittal alignment based on IPs in different age groups.
The purpose of this study was to compare sagittal alignments based on IPs and to elucidate the changes while considering age groups.
Materials and methods
This study was approved by the institutional review board at the institution of the corresponding author (IRB number: 2014-I118). In this retrospective study, we analyzed the collected clinical information and the digitalized image documents after receiving consent from the adult volunteers to use them for the clinical study. The subjects included 147 asymptomatic healthy adults who had not undergone surgeries but underwent whole spine standing radiographs from 2003 to 2012. They wanted to undergo the whole spine radiograph for the checkup about the alignment of the whole spine on their own account without any symptom related to the spine. The subjects’ clinical and demographic information was blinded to the examiner. The subjects included 73 male and 74 female adults; their average age was 44.0 years old (range 20–74). The subjects consisted of three groups as follows: 49 subjects in their 20s from 20 to 29 years old, 50 subjects in their 40s from 40 to 49 years old, and 48 subjects in their 60s from 60 to 69 years old. We did not include subjects who are in their 30s, 50, or 70s to make the results clear. The average body mass index (BMI) of the subjects was 22.5 ± 3.4 kg/m2 (range: 10.1–30.0 kg/m2). The average BMI was not significantly different among the three age groups (22.0 ± 2.8 kg/m2 in the 20s, 22.5 ± 2.5 kg/m2 in the 40s, and 22.8 ± 4.1 kg/m2 in the 60s, p > 0.05).
The radiological assessments were performed by the standardized procedures. The subjects were instructed to stand quietly in the upright position while looking straight ahead with the bilateral hips and knees fully extended. Subjects also had both feet shoulder width apart with their heads relaxed with his or her fingertips touching the clavicles. Lateral radiographs were performed using standard radiographic techniques, wherein the tube was centered on the level of the center of the xiphoid process. The radiographic film cassette was 182 cm (72 inches) from the tube, and radiographs were taken without magnification.
Two experienced spine surgeons measured each of the radiographs on two separate occasions separated by 1 month randomly. They measured the first, second, third, fourth, fifth, and sixth end vertebrae from the bottom in the whole spine lateral radiographs by identifying the most tilt vertebrae, similar to the end vertebra of the whole spine anteroposterior radiographs for patients with scoliosis. The McGregor’s line and lower horizontal margin of the lateral radiograph at the bottom were also measured. The third end vertebra of the thoracolumbar IP was identified, and the fifth end vertebra was the cervicothoracic IP. Next, the sacral slope was measured between the lower horizontal margin and the first end vertebra, the functional lumbar segment between the second and third end vertebrae, the functional thoracic segment between the fourth and fifth end vertebrae, and the functional cervical segment between the sixth end vertebra and the McGregor’s line (Figure 1). The IP distances were measured from the C2 plumb line to the point bisecting the upper end plate of the thoracolumbar and cervicothoracic IPs, in addition to C2 sagittal vertical axis (SVA) distance to S1 (Figure 2). We arbitrarily assigned a positive value when the sagittal angle was kyphotic or when the C2 plumb line was located anterior to the end vertebra.

Sagittal Cobb angles of the sacral slope between the lower horizontal margin and the first end vertebra (α), the functional lumbar segment between the second and third end vertebrae (β), the functional thoracic segment between the fourth and fifth end vertebrae (γ), and the functional cervical segment between the sixth end vertebra and McGregor’s line (δ).

The IP distances from the C2 plumb line to the point bisecting the upper end plate of the (a) first sacrum (C2 SVA distance to S1), (b) thoracolumbar, and (c) cervicothoracic IPs. IP: inflection point; SVA: sagittal vertical axis.
Statistical analyses were completed using IBM Statistics 24 (IBM SPSS, Armonk, New York, USA). The differences in continuous variables among the three groups were examined with analysis of variance (ANOVA). Differences in continuous variables between two out of the three groups were examined with post hoc ANOVA based on the Tukey’s method. Values were expressed as the mean values with standard deviation. Preliminary statistical power analyses were performed by G*Power version 3.1.5 (Universität Kiel, Germany). The power was 0.8 for ANOVA with an effect size of 0.25. The total sample size should be more than 128. The sample size in each group should be more than 43.
It was considered significant when p was less than 0.05. When two experienced spine surgeons had different IPs, they engaged in a discussion to reach a final conclusion about the appropriate IPs. The intraobserver and interobserver reliabilities were calculated using the reliability statistics by intraclass correlation (ICC) for the distance and the Cobb angle. 19,20 The ICC values were graded using previously described semiquantitative criteria: excellent for values in the 0.9–1.0 range, good for 0.7–0.89, fair/moderate for 0.50–0.69, low for 0.25–0.49, and poor for 0.0–0.24. 19,20
Results
Distribution of the IPs in the total study population
The thoracolumbar IP was L2 in 64 patients (43.5%), L1 in 35 patients (23.8%), and L3 in 25 patients (17.0%; Table 1). The cervicothoracic IP was T1 in 62 patients (42.2%), T2 in 30 patients (20.4%), and C7 in 22 patients (15.0%).
Distribution of IPs in the total study population.
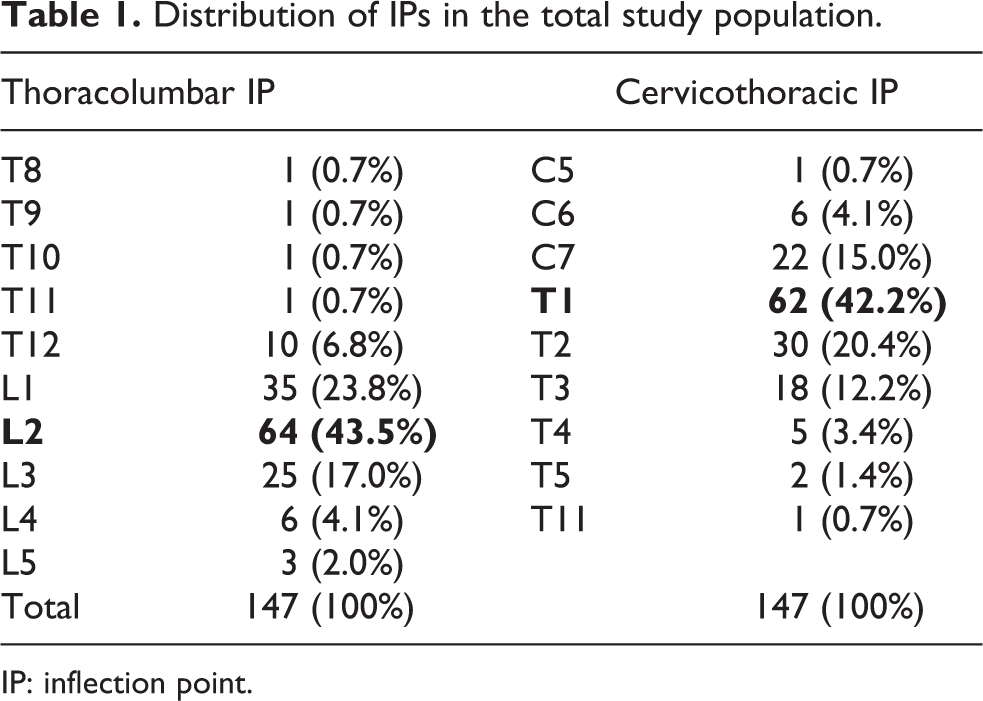
IP: inflection point.
The angle of segments and IP distances in the total study population
The sacral slope, pelvic incidence, functional lumbar, functional thoracic, and functional cervical segments were 34.39 ± 9.10°, 59.14 ± 8.70°, −37.04 ± 12.19°, 45.92 ± 15.82°, and −27.19 ± 14.82°, respectively. The C2 SVA distance to S1, thoracolumbar, and cervicothoracic IP distances were 2.28 ± 39.19 mm, 16.49 ± 34.38 mm, and 13.85 ± 17.80 mm, respectively. The reliability statistics by ICC for the Cobb angle was 0.777 for the intraobserver reliability and 0.672 for the interobserver reliability. The reliability statistics by ICC for the distance was 0.998 for the intraobserver reliability and 0.965 for the interobserver reliability.
Comparison of measured values by age groups
The most common thoracolumbar IP was L2 in all age groups (Table 2). However, the next most common cervicothoracic IP changed from T2 in the youngest age group to C7 in the oldest age group, even though the most common cervicothoracic IP was T1 (p = 0.009, Table 3).
The difference of the thoracolumbar IP according to age groups.

IP: inflection point.
The difference of the cervicothoracic IP according to age groups.
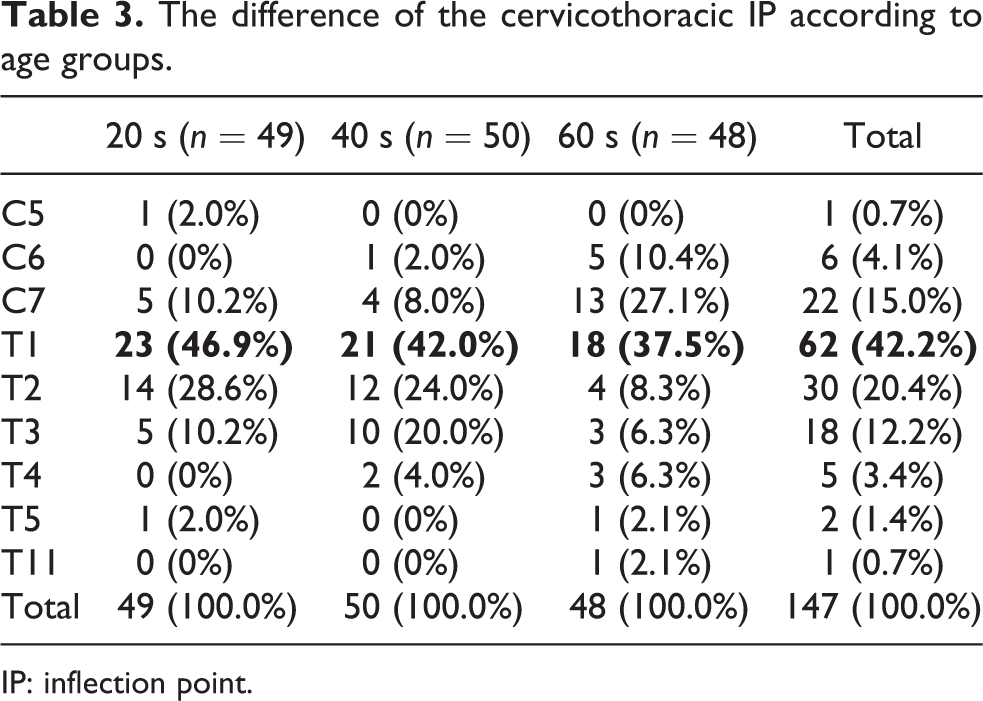
IP: inflection point.
There was a difference in the sacral slope and functional lumbar segment among age groups (p = 0.002, p = 0.005, respectively), but there was no difference in the pelvic incidence, functional thoracic segment, or functional cervical segment among age groups (Table 4). The C2 SVA distance to S1 and thoracolumbar IP distance differed among age groups (Table 4). However, the cervicothoracic IP distance did not differ (Table 4). The angles of the sacral slope and functional lumbar segment decreased in the 60s age group compared with the 20s or 40s age groups (Table 5). Similarly, the C2 SVA distance to S1 and thoracolumbar IP distance increased for the 60s age group compared with the 20s or 40s age groups.
The difference of sacropelvic morphology, sagittal Cobb angles of segments, and the IP distance according to age groups.

IP: inflection point; SVA: sagittal vertical axis.
The difference of sagittal Cobb angles of segments and the IP distance between two age groups.
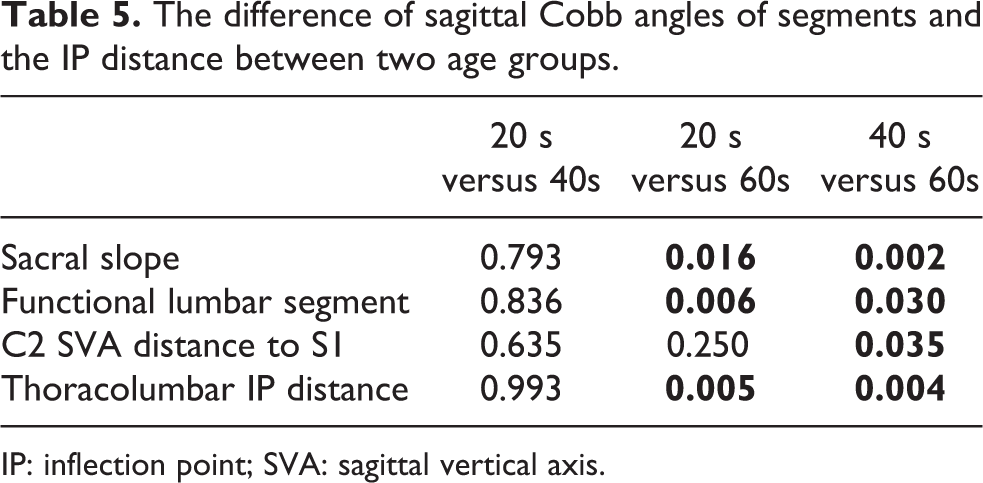
IP: inflection point; SVA: sagittal vertical axis.
Discussion
The purpose of this study was to investigate sagittal alignment using IPs and their variations while considering age. In the current study, the most common thoracolumbar and cervicothoracic IPs in the total population were L2 and T1, respectively. However, the next most common cervicothoracic IP changed from T2 in the youngest age group to C7 in the oldest age group, even though the most common cervicothoracic IP was T1. The sagittal Cobb angles decreased at the sacral slope and functional lumbar segment due to possible age-related degeneration. Similarly, the IP distances increased at the C2 SVA distance to S1 and thoracolumbar IP distances due to possible degeneration.
Stagnara et al. 21 investigated 100 healthy French volunteers who were between 20 years and 29 years old. They evaluated the global angle of lordosis and kyphosis, united by an intermediate thoracolumbar vertebra tilted most from the horizontal in the standing lateral radiograph of the whole spine. 21 The intermediate thoracolumbar vertebrae were T12 (22%), L1 (33%), and L2 (21%). 21 The global angle of kyphosis was 50° ± 30°, and the global angle of lordosis was 37°. 21 In addition, Vaz et al. 22 investigated 112 healthy volunteers between the ages of 20 and 45 years old. They evaluated the global angle of lordosis and kyphosis, united by a straight thoracolumbar segment in the standing lateral radiograph of the whole spine. 22 The global angle of kyphosis was 47.92 ± 3.5°, the global angle of lordosis was 46.5 ± 11.1°, and the sacral slope was 39.4 ± 9.3°. 22 Berthonnaud et al. 17 evaluated 160 asymptomatic volunteers between the ages of 20 and 70 years old. They evaluated the IPs between lordosis and kyphosis and the segments bound by the IPs in the standing lateral radiograph of the whole spine. 17 They found that the pelvic tilt has a linear correlation with the functional lumbar segment (r = 0.62, p < 0.001). 17 Although these studies reported variations in the lateral radiograph of the whole spine, sagittal alignments based on IPs of the end vertebrae were not carefully considered among age groups. The degenerative changes in older adults decreased the IP in sagittal Cobb angles and increased the IP distance in lumbar and sacral spines. This sagittal alignment was a compensation strategy within the spine, especially the cervical and lumbar spines as well as the sacrum, which may potentially be responsible for degenerative changes. Clinicians need to consider functional aspects of age-related degeneration in the sagittal plane and compensatory changes in the cervical and lumbar spines.
The results of our study were supported by a recent study, which was reported by Roussouly et al. 18 Their study evaluated 160 asymptomatic volunteers who were between 18 years and 48 years old. They evaluated the IPs and the functional lumbar segment bound by the upper end plate of the first sacrum and the IP from lordosis to kyphosis in the standing lateral radiograph of the whole spine. 18 They utilized a four-part classification scheme of sagittal morphology to classify each patient and concluded the patterns of variation in sagittal alignment to discover the association between spinal balance and the development of degenerative changes. 18 However, their study represented the range of sagittal alignment in young healthy participants without considering the age.
Other studies indicated an anatomic classification for the changes of sagittal alignments due to aging. 1,23 In a study that compared 85 patients with a lumbar degenerative disease with a normal control group, the patients had a greater decrease of sacral slope, more loss of lumbar lordosis (similar to the functional lumbar segment in the current study), and more anterior translation of the C7 plumb line (similar to the C2 SVA distance to S1 in the current study). 23 As the results of lateral spinal radiographs of 172 participants, Boyle et al. 1 found that the inflection of the cervicothoracic junction (the cervicothoracic IP in the current study) is T3 in the young age group, which moves to T1 with increasing age.
It is possible that the difference in the IPs might be due to the magnitude of the pelvic incidence. 17 We evaluated whether the changes of the IPs among age groups are related to the changes in the magnitude of the sacropelvic morphology of pelvic incidence, sacral slope, and the functional lumbar segment (similar to lumbar lordosis). There was no difference in the pelvic incidence among age groups, but the sacral slope and functional lumbar segment were different among age groups. The changes of the IPs according to age groups are due to aging instead of the magnitude of the sacropelvic morphology.
As with any study, the present investigation has some limitations. First, we did not compare the functional classification based on IPs with the anatomic classification to evaluate the sagittal alignments. Second, the study of alignment should ideally be performed using the biplanar slot scanner (EOS imaging technology), which gives true to axis images. In the current study, standard radiographs were used and might make measurements inaccurate and unreliable. Fortunately, the reliability statistics by ICC for the Cobb angle and the distance in the current study were excellent to moderate. Third, the number of the study population is too small to reflect those of the Korean population because the recruitment was made by their own intentions. Fourth, we neither provided the longitudinal data nor performed multivariate analysis to support that the degeneration is the cause of change of sagittal alignment parameters because it is a cross-sectional study, the number of the study population is small to perform the multivariate analysis, and we did not have the information about the magnetic resonance image of the whole spine of the study population. Therefore, it is possible that the subjects are inherently different and may not be related to aging. However, the aging factor resulted in an inverse relationship with disc height in the magnetic resonance image study for the lumbar spine. 24 The decreased disc height of the degenerative lumbar spine in the older adults might be related to the decreased sagittal Cobb angles of the lumbar spine based on the IP. Consequently, the C2 SVA distance to S1 and the thoracolumbar IP distance increased following the decreased sagittal Cobb angles of the functional lumbar segment. Further studies are required to evaluate the changes of the IPs according to disc degeneration based on magnetic resonance images studies in the larger study population in the future. Fifth, the study population included the volunteers. Even though they wanted to undergo the whole spine radiograph without any symptom related to the spine, they might have the possibility of their concerns about the spinal problems, which is the selection bias. Finally, the use of the C2 plumb line for sagittal balance has a risk of grouping together the normal and compensated subjects with balanced alignment. The angular measurements of spinosacral angle may overcome the risk. 25 However, to the best of our knowledge, this represents the first set of normative data on asymptomatic subjects in both young and old groups regarding sagittal alignment using IPs. Clinicians may consider sagittal alignments based on the IPs to clarify compensatory changes of the sagittal plane according to different age groups. Therefore, these functional alignments could be valuable to patients with degenerative spinal deformities, which are common in the aged as commonly utilized Cobb angles in the coronal plane.
Conclusion
In conclusion, the degenerative changes in elderly people might make the sagittal Cobb angles based on the IP decrease and the IP distance increase at the lumbar and sacral spines. The new method using the IP might be useful to evaluate the sagittal alignment of the spine in functional aspects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.