
Abstract
Hydatidosis is a zoonotic parasitic disease caused by Echinococcus, which is highly prevalent in pastoral areas. In China, this disease is mainly caused by Echinococcus granulosus and Echinococcus multilocularis. Cystic echinococcosis, which is one of the most common types of echinococcosis, is described as swelling and growth of cystic lesions. Alveolar echinococcosis, which is less common, is invasive. Cases of mixed echinococcosis infection accompanied by extrahepatic organ metastasis are extremely rare. Treatment of these cases is complicated and the prognosis is extremely poor. We report a case of hepatic echinococcosis in a 40-year-old Tibetan man who was treated with the hepatic right tricuspidectomy + left hepatic duct jejunostomy (Roux-en-Y) surgical procedure. This procedure provides a reference for treatment of similar cases of echinococcosis. For patients with multiorgan metastasis, chemotherapy is the first choice. This should be followed by possible surgical treatment for life-threatening lesions of alveolar echinococcosis and subsequent chemotherapy. Individualized treatment accompanied by multidisciplinary treatment and damage control surgery could optimally benefit patients with advanced hepatic echinococcosis.
Keywords
Introduction
Hydatidosis, also known as hydatid disease, is a zoonotic parasitic disease that is caused in the intermediate host by Echinococcus granulosus infection. Hydatidosis is mainly prevalent in the northern hemisphere and is extremely harmful to human health. 1 After humans ingest food contaminated with echinococcosis eggs, the eggs enter the intestine and parasitize the liver through the portal system to form liver hydatid lesions. Hydatidosis occurs most frequently in the liver (70%), followed by the lungs (20%), and it occasionally occurs in other organs, such as the spleen, heart, kidney, and brain. Hepatic hydatidosis echinococcosis is commonly observed in China. E. granulosus infection of the liver, which is caused by infection with E. granulosus eggs, is also called cystic echinococcosis. Echinococcus multilocularis infection of the liver, which is caused by infection with E. multilocularis eggs, is also called alveolar echinococcosis. 2 Hepatic hydatid lesions can affect the entire liver, destroying its anatomy and impairing its function. Without effective measures, the mortality rate of echinococcosis can reach 90%. At present, treatment of echinococcosis is mainly based on surgery, combined with intervention and drug therapy, which serve as a supplementary comprehensive treatment. 3 Because hepatic alveolar echinococcosis has similar invasive growth characteristics as malignant tumors, the lesions involve important blood vessels and bile ducts in the hilum. This makes achieving radical resection difficult or impossible, especially in patients with both types of echinococcosis accompanied by distant organ metastasis, which is more difficult to treat. We report a case of hepatic two-type hydatid disease that was treated with hepatic right trifoliate resection + left hepatic duct jejunostomy (Roux-en-Y). After the operation, most of the lesions in the important bile duct and blood vessel area to be preserved were removed. The remaining lesions were finely stripped, with the aim of minimizing postoperative lesion load, preventing acute infection, reducing suffering of the patient, and improving quality of life.
Case presentation
The patient was a 40-year-old Tibetan man who had lived in a pastoral area for a long time. He was admitted to hospital for the first time with intermittent right upper quadrant pain for longer than 1 year and aggravation of 10 days. After admission, abdominal B-ultrasound showed masses in the S4 and S5 segments of the liver and a 124 × 93-mm mixed mass. The boundary of the mass was blurred, the shape was irregular, and there was a strong echo (uneven small calcification) inside the lesion. The rest of the liver had several similar scattered echoes with diameters of 30 to 40 mm. Upon exploration, 82 × 54-mm (segment S5) and 102 × 63-mm (across segments S6, S7) cystic masses were identified. The boundary of the masses was still clear, the wall thickness was 4 mm, and a number of small, liquid, dark areas were observed. In segment S4 of the liver, another 70 × 68-mm hyperechoic mass was found. The boundary was clear, and the lesion was irregular in shape. The hepatic portal system was deformed by compression, and the right hepatic vein and portal vein were invaded. Computed tomography (CT) and magnetic resonance imaging (MRI) of the abdomen showed the following. (1) Segment S4 of the liver contained large mass lesions in the right lobe and multiple round-shaped, low-density lesions. The maximum cross-sectional area was 16.7 × 9.8 cm. This was considered hepatic alveolar echinococcosis with multiple intrahepatic metastases. The portal vein and intrahepatic artery were greatly affected, and the hepatic hilum and right kidney were compressed. (2) Multiple cystic lesions in the right lobe of the liver were observed. Segments S2 and S3 of the liver were dominated by calcification, and the maximum diameter was 7.3 × 6.7 cm. This was considered multiple hepatic cystic hydatid disease (Figure 1). Chest CT showed multiple irregular nodules in both lungs, which were considered hydatid lung metastases (Figure 2). Laboratory tests showed that an echinococcosis serum test was positive. According to World Health Organization-Primary Lesions Neighboring Organs And Metastasis Staging, the lesions were staged as P4N1M1, and the opportunity for radical surgical resection had been lost. The patient’s liver function was normal. We continued treatment with oral administration of albendazole (15 mg/kg/day, twice a day).
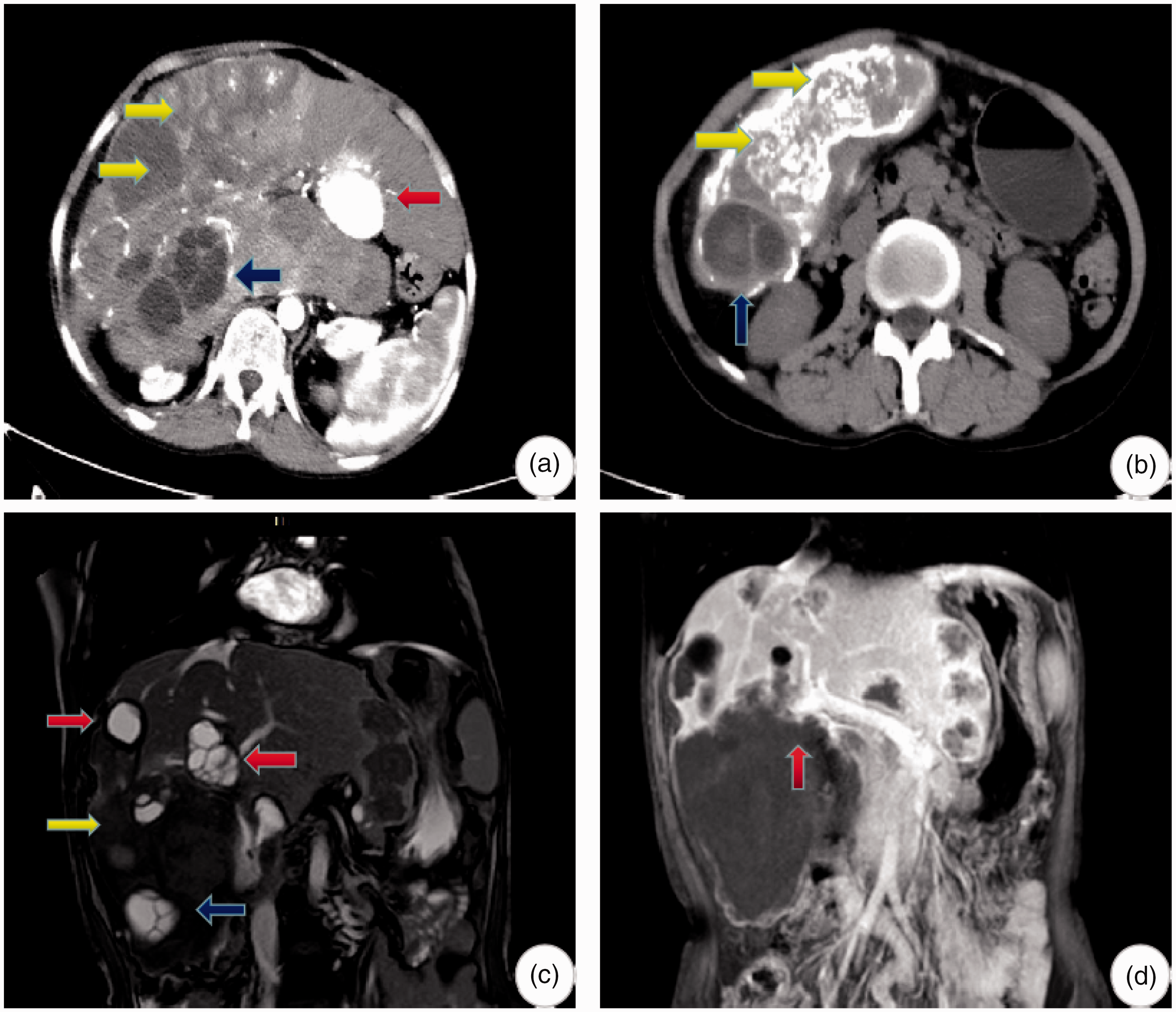
Preoperative imaging examination of the patient. (a) The enhanced phase of computed tomography shows CE5 cystic echinococcosis at segments S2 and S3 of the liver (calcification type, red arrow). CE2 cystic echinococcosis can be seen at segments S6 and S7 of the liver (multi-sub-capsule type, blue arrow). Giant vesicular echinococcosis can be seen across segment S4 in the hepatic right lobe (yellow arrow). (b) Cystic echinococcosis can be seen in the plain scanning stage of computed tomography (blue arrow), as well as vesicular echinococcosis (yellow arrow). Uneven calcification can be seen in the lesion. (c) Magnetic resonance imaging shows cystic hydatidosis with clear boundaries (red and blue arrows). Small cystic structures of different sizes in echinococcosis lesions, which are typical cystic changes, can be seen. The interval of a low signal is a “rose petal sign” and echinococcosis can be seen (yellow arrow). (d) The right branch of the portal vein is invaded (red arrow).

(a) Computed tomography shows distant organ lung metastasis. (b) The patient also has distant organ brain metastasis. (c) Computed tomographic results of a reexamination 27 days after surgery showing a small number of residual lesions. (d) Computed tomographic reexamination results 2 months after surgery. The red arrows show the drainage tube.
Two years later, the patient was admitted to the hospital again because of recurrent abdominal pain and bloating for more than 2 months. A physical examination showed tenderness in the right upper abdomen and a swollen liver under the right costal margin, approximately 8 cm below the costal margin. The lesions had increased compared with the previous admission.
We obtained the patient’s consent for publication. The study was approved by the Ethical Committee of the Affiliated Hospital of QingHai University (26-June-2018, Grant No: P-SL-2018011).
Therapy process
After discussion with the multidisciplinary team, and taking into account the patient’s medical history, clinical manifestations, imaging examination, and laboratory results, the diagnosis of liver-type echinococcosis accompanied by distant organ metastasis was established. Continuous oral albendazole treatment was not effective in treating liver lesions in the patient. The lesions did not shrink, but increased, and the patient showed persistent abdominal pain and distension. To improve the quality of life of the patient and prevent liver failure caused by acute infection, we decided to perform palliative surgery. Surgery can achieve the following two purposes: (1) resection of the right hepatic lobe, providing adequate drainage to control infection, and (2) confirmation of the diagnosis for follow-up treatment, although the lung lesions cannot be removed in one procedure. Preoperative evaluation indicated the following: liver function was rated as Child grade A, with an indocyanine green retention rate in 15 minutes of 12.2%, and increased left liver compensation. During the operation, after general anesthesia, the upper abdomen was opened with an inverted L-shaped incision. The right lobe of the liver was swollen. The lesion was tightly adhered to the diaphragm, the omentum, and the right kidney. Hepatic cystic echinococcosis was closely related to the middle and left hepatic veins, and cheese-like necrosis (CE5 type) was observed between these veins. The first hepatic hilum was dissected and the blockage band was reserved. The right branch of the portal vein and the proximal end of the bilateral hepatic duct were invaded by the lesion. The lesion on the right side was removed as far as possible along the edge of the lesion, and the CE5 type cystic necrosis was removed. The left hepatic duct was isolated in the left hepatic lobe and left hepatic duct jejunostomy (Roux-en-Y) was performed. The liver section and the hepatic and intestinal anastomosis were placed in the drainage tube. The operation took 300 minutes, intraoperative blood loss was approximately 3000 mL, and the blood transfusion volume was 2000 mL. The postoperative pathological diagnosis was hepatic alveolar echinococcosis and hepatic cystic echinococcosis (Figure 3).
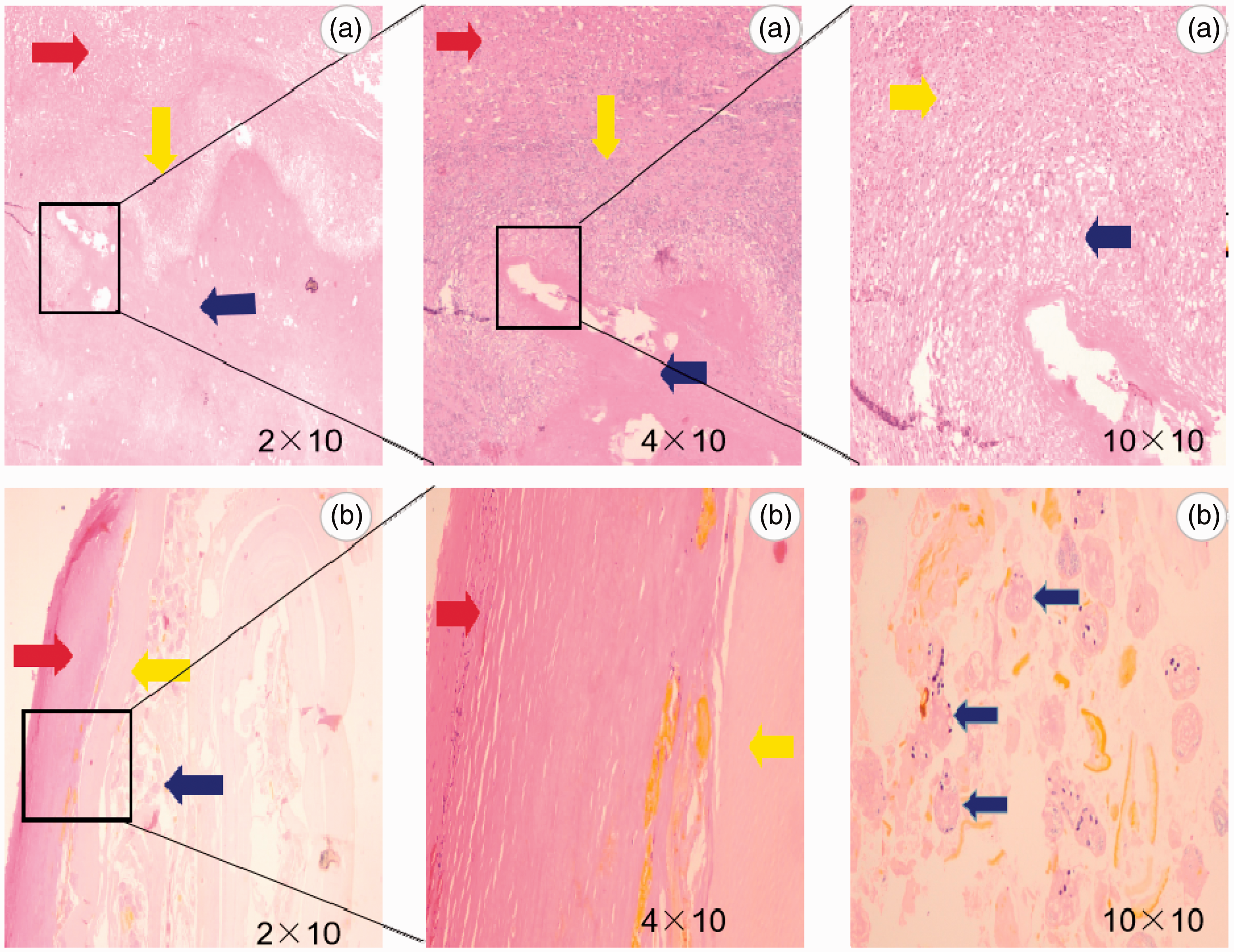
(a) Different magnifications of the corresponding areas in the marginal zone of vesicular echinococcosis as shown by hematoxylin and eosin staining. The red helix shows a clear hepatic cord structure, and hepatocytes are evenly arranged and bridge-like, which indicate normal liver tissue. Most inflammatory cells of different sizes, such as eosinophils, lymphocytes, and macrophages, are seen within areas of the inflammatory infiltrative zone (yellow arrow). There is no obvious hepatic cord and cell structure in the lesion area (blue arrow). There are small vesicles of different sizes and there are interstitial substances with different contents around the vesicles, which are shown as red areas. (b) Different magnifications of the corresponding areas of cystic hydatid cystic pathology as shown by hematoxylin and eosin staining. The inner capsule is divided into two layers. The outer layer is the stratum corneum, which is indicated by the red arrow, and is divided into multiple layers. Elasticity, separation of the layers, and structural fractures were observed. The inner layer is a germinal layer (yellow arrow) in which pedicled germ cell head segments and hair follicles can be grown (blue arrows).
Postoperation, the patient developed a fever, increased white blood cells, and abnormal coagulation indicators (prothrombin time: 19.8 seconds, prothrombin time activity: 56%). He was administered anti-infection, plasma supplement, and liver protection drugs, with other treatment and infection control. Liver function indicators returned to normal on the 12th day after surgery. His temperature and white blood cell counts returned to normal on the 14th day. On the 7th day after surgery, the patient presented with bilateral massive pleural effusion and underwent bilateral pleural effusion drainage, which further improved the hypoalbuminemia. The pleural effusion was eliminated on the 12th day after surgery. No drainage was found in the abdominal cavity on the 20th day and the drainage tube was removed. On the 27th day after surgery, fever and the leukocyte count rose again. Reexamination of abdominal CT (Figure 2) showed perihepatic effusion and a low-density shadow of the residual cavity. These findings in addition to the clinical symptoms and laboratory examinations suggested postoperative residual effusion. Puncture drainage was performed under the guidance of B-ultrasound because of the possibility of concomitant postoperative infection after echinococcosis. The left cystic mass produced yellow-white purulent liquid and right perihepatic puncture released the bile-containing liquid. After 10 days of active administration of component drainage and anti-inflammatory, liver protection, and nutritional support treatment, the body temperature and white blood cell counts returned to normal. The cystic mass had no drainage in the residual cavity and extubation was then performed. A small amount of bile fluid was continuously drained from the liver, and a small amount of bile leakage was considered. The patient was eventually discharged from the hospital with a tube on the 43rd day after surgery, and bile leakage ceased after 2 months.
Discussion
Hydatidosis is a serious zoonotic disease that is caused by aphids that are parasitic to humans and certain animals. Hydatidosis has a worldwide distribution. According to the results of a national survey on the status of important human parasitic diseases in 2004, the average prevalence rate of hydatidosis in the population in endemic areas of echinococcosis was 1.08%, among which hepatic cystic echinococcosis accounted for 95%. 4 There are also differences in the prevalence of hydatidosis in different regions of the same country. The six provinces (regions) of Sichuan, Qinghai, Xinjiang, Gansu, Inner Mongolia, and Ningxia, account for 97% of the total number of reported cases of hydatidosis in the national network. These areas of a high incidence of echinococcosis in China account for more than 40% of the country’s land area, and the threatened population is approximately 66 million. According to the World Health Organization, the incidence rate of hydatidosis is 2% in high incidence areas. The incidence rate of echinococcosis in western China is 3.1% to 31.5% and the prevalence rate is 0.5% to 5.0%. The prevalence of hydatidosis in the population in some areas of the Qinghai–Tibet Plateau is 5.0% to 10.0%. However, the prevalence of mixed hydatids has not been reported in China or other countries. Alveolar echinococcosis is prevalent in high latitudes of Europe, Asia, and North America. 5 Hepatic alveolar echinococcosis in China is mainly found in the Sanjiangyuan area in Qinghai Province. 6
Obtaining the correct diagnosis of echinococcosis is crucial. The main diagnostic points of echinococcosis include the following. (1) Personal history is extremely important. Whether there is a pastoral life history and whether there is a history of contact with canines are important to know. Hydatidosis occurs in western pastoral areas. There are scattered cases of hydatidosis in agricultural areas, but most individuals have lived, worked, or have short-term travel history in pastoral areas. Adult worms of aphids live in the small intestine of canines. The eggs are excreted with the feces and are eaten by people after contaminating food and water. Worms can develop hooks in the human small intestine. After entering the blood, the worms enter the portal vein and usually colonize the liver. Hydatidosis is caused by echinococcosis initially in the liver, followed by the lungs and brain. Hydatidosis can also occur in any tissues and organs, such as the abdominal cavity, spleen, kidney, bone, and even the eye. (2) A serum immunological examination can be used as a reference for diagnosis, but this is not a basis for diagnosis. At present, an enzyme-linked immunosorbent assay is a commonly used method for diagnosing hepatic hydatidosis. If crude cystic fluid is used as an antigen, its sensitivity and specificity are not high, and this approach is often used when determining the epidemiology of hydatidosis. Initial serological screening in a survey, when detecting specific immunoglobulin G antibodies to diagnose echinococcosis, can increase the specificity and sensitivity to 89.7% and 96.5%, respectively, and increase the diagnostic accuracy to 92.3%. 7 (3) Imaging examinations mainly include B-ultrasound, CT, and MRI. An ultrasound examination shows strong echogenic lesions, and there may be uneven echoes inside. A CT scan shows an uneven mass and solid mass, and enhanced lesions show no obvious enhancement. Vesicles, calcification, and liquefaction necrosis are observed in the lesions. An MRI examination shows no regular solid masses, mainly a low signal, increased normal tissue enhancement, and no enhancement of lesions, resulting in clear boundaries. (4) Intraoperative lesions need to be differentiated from cancer and tuberculosis. Vesicular echinococcosis specimens are characterized by milky white or milky yellow surfaces. The texture of specimens is harder and denser than cancer. If there is calcification, it is extremely hard. In our patient, most of the borders of the masses were clear, but small pockets were visible on the edges. After a specimen was cut, it was solid, and the section was cheese-like. The larger lesion had liquefaction necrosis in the center and the liquid was purulent. The particularity and rarity of this condition lead to extremely complicated treatment. Echinococcosis is an endemic parasitic disease, which is relatively rare, especially when combined with vesicular and cystic components accompanied by extrahepatic distant organ metastasis. There have been no case reports of patients with two types of echinococcosis, and there is a lack of corresponding diagnostic consensus and standardized treatment.
Choosing the right treatment is crucial for improving the efficacy of echinococcosis. For lesions of hepatic alveolar echinococcosis that cannot be radically resected, physicians need to determine whether the patient has symptoms. If there are no symptoms, the patient can be considered for observation, and no surgery is required. After symptoms appear, surgical indications are evaluated. Radical surgical resection is still the preferred method for treating echinococcosis. The rate of radical resection of hepatic alveolar echinococcosis in European countries and Japan is greater than 50%. The radical resection rate of hepatic alveolar echinococcosis in China is 31.5%, which may be related to advanced cases that have been identified in China. 8 For patients with two types of echinococcosis, we adopt individualized treatment. We first performed vesicular hydatidectomy in our patient because of the large range of the right hepatic vesicular type of echinococcosis. After recovery of residual liver function, elective cystic hydatid puncture drainage was performed to prevent liver failure due to insufficient residual liver volume. The safe distance of the liver resection range is preferably 2 cm from the echinococcal lesion, which ensures that the lesion is cleared. If clinical practice does not meet this requirement, the lesion should be removed as completely possible. However, removing lesions of the inferior vena cava is difficult because of potential hydatid invasion of the inferior vena cava wall. A residual lesion that is in contact with a small amount of the inferior vena cava wall is also considered to have a radical effect after being inactivated with 10% hypertonic saline. In this case, albendazole can also enhance long-term survival after surgery, but the growth cycle of the echinococcosis is still relatively long. If there is a combination of cerebral echinococcosis with echinococcosis in other body sites, the prognosis is poor in most cases. In principle, neurosurgery should be performed first, followed by surgery targeting other echinococcosis-affected organs, such as the liver, lungs, and spleen.
Our patient’s hepatic hydatidectomy achieved the expected surgical purpose. After 2 months, an imaging review was performed (Figure 2). The patient recovered well postoperatively. We believe that, for patients with two types of echinococcosis and with remote organ metastasis, radical surgery or conditional liver transplantation should be performed after the disease is stable or the lesion is reduced. The lesions should be treated first and then chemotherapy is appropriate, but this approach is subject to further medical evidence. With regard to the nutritional status, patients with a poor diet may consider extending the time to remove the T tube after surgery. With advances in technology and improvement in surgical safety, we are confident that, in the future, surgical treatment of hepatic echinococcosis will play a vital role in curing this condition. This will reduce the suffering of patients, improve survival, and alleviate the social and family economic burden.
Conclusion
According to PNM classification and early-medium-late staging of hepatic alveolar echinococcosis, individualized treatment can improve the cure rate and quality of life of patients with echinococcosis. For patients with multiorgan metastasis, chemotherapy is the first choice, and this should be followed by possible surgical treatment for life-threatening lesions of alveolar echinococcosis. This approach should be subsequently followed with more chemotherapy. We believe that, although patients with advanced hepatic alveolar echinococcosis are difficult to treat, design of individualized treatment plans combined with guidance of multidisciplinary diagnosis and the surgical concept of injury control can provide the maximum therapeutic benefit to these patients.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Funding was provided by the Key Projects of Precision Medicine Research in National Key R&D Programmes (2017YFC0909900), the Special Project of the Clinical Medicine Research Center of the Qinghai Department of Science and Technology (2017-SF-L2), and the Qinghai Provincial Health Planning Commission guiding project (2016-wjtg-04).