
Abstract
There has been a wide interest in using platelet-rich plasma (PRP) as a therapeutic agent to enhance spinal fusion. There are two review articles based only on clinical studies regarding the effect of PRP on spinal fusion. However, with regard to both animal model studies and clinical studies, there is no review studies regarding its effect on spinal fusion and no review studies focusing on the platelet count and the concentration of the growth factor in the PRP. The purpose is to review the literatures about the effect of PRP on spinal fusion according to the animal model studies and clinical studies, focusing on the effect of the platelet count and the concentration of the growth factor in the PRP. A PubMed search was performed for English-language articles. We identified 20 articles regarding the effect of PRP on fusion in animal model studies and clinical studies, of which 16 articles met the study criteria of case–control studies or prospective randomized studies for the spinal fusion. The articles were categorized into small-sized animal model, middle-sized animal model, and clinical studies. Studies have shown both beneficial and inhibitory effects. The conclusion that PRP has the stimulating effect on spinal fusion was not reached. However, PRP might promote the human spinal fusion if the platelet count or the concentration of growth factors in the PRP increases.
Introduction
Spinal fusion is a frequent procedure for treating spinal degenerative disease, spinal fracture, and spinal deformities. Pseudoarthrosis after spinal fusion surgery is one of the serious complications. 1 Various attempts including pedicle screw instrumentation, plate insertion, interbody fusion (IF), autogenous bone graft (ABG), and recombinant human bone morphogenic protein-2 (rhBMP-2) have been made to overcome this complication 2 –5 ; however, these methods have not eliminated pseudoarthrosis and were accompanied by undesirable side effects. 6,7
According to in vitro studies, platelet-rich plasma (PRP) is an autogenous source of growth factors with osteoinductive properties. 8,9 PRP has several growth factors, such as platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF-β). 10,11 As a new trial, there has been a wide interest in using PRP as a therapeutic agent to enhance spinal fusion. The are two review articles on the effect of PRP on spinal fusion, which are based only on clinical studies. 12,13 However, based on both animal model studies and clinical studies, there are no review studies regarding its effect on spinal fusion and no review studies focusing on the effect of the platelet count and the concentration of the growth factor in the PRP on spinal fusion.
We reviewed the literature focusing on the effect of the platelet count and the concentration of the growth factor in the PRP on spinal fusion based on the animal model and clinical studies.
Review
Using the PubMed search engine, a detailed computerized literature search for using medical subject headings of “platelet rich plasma” and “fusion” and “lumbar vertebrae” or “cervical vertebrae” was conducted. This database consisted of literature published from 1980 through 2016. We included only English-language articles. During screening, the articles meeting any of the following criteria were excluded from the review: (1) case-series studies and review studies, (2) studies that were not conducted in in vivo system, either animal or human, (3) studies that did not evaluate spinal fusion, (4) studies did not use control subjects, (5) studies that did not evaluate the subjects receiving PRP, (6) studies did not include at least one of the following: a measurement of fusion rate with histologic or radiologic assessment, (7) studies that did not perform statistical analysis, and (8) case reports. The search strategy yielded 20 articles based on animal and clinical studies regarding the effect of PRP on spinal fusion. Two articles were excluded because they did not use control subjects, 14,15 and another two articles were excluded because they did not evaluate spinal fusion. 16,17 Of the 20 articles, 16 met the study criteria (Figure 1). 18 –33 These 16 studies were categorized into small-sized animal model, middle-sized animal model, and clinical studies.

Flowchart showing results of literature search.
All articles were retrospective case–control studies or prospective randomized studies. Three studies were based on the small-sized animal model of rats (Table 1) and three studies were based on the middle-sized animal models (Table 2). The remaining 10 studies were about the effect of PRP, which were based on the human spinal fusion models (Table 3).
Literature review about the effect of PRP on the spinal fusion based on rat model.

DT: duration of treatment (months); PLF: posterolateral fusion; IF: interbody fusion; ABG: autogenous bone graft; ABM: autogenous bone marrow; ACS: absorbable collagen sponge; PRP: platelet-rich plasma; PPP: platelet-poor plasma (supernatant); HA: hydroxyapatite; CT: computed tomography; NSD: no significant difference.
Literature review about the effect of PRP on the spinal fusion based on the middle-sized animal model.
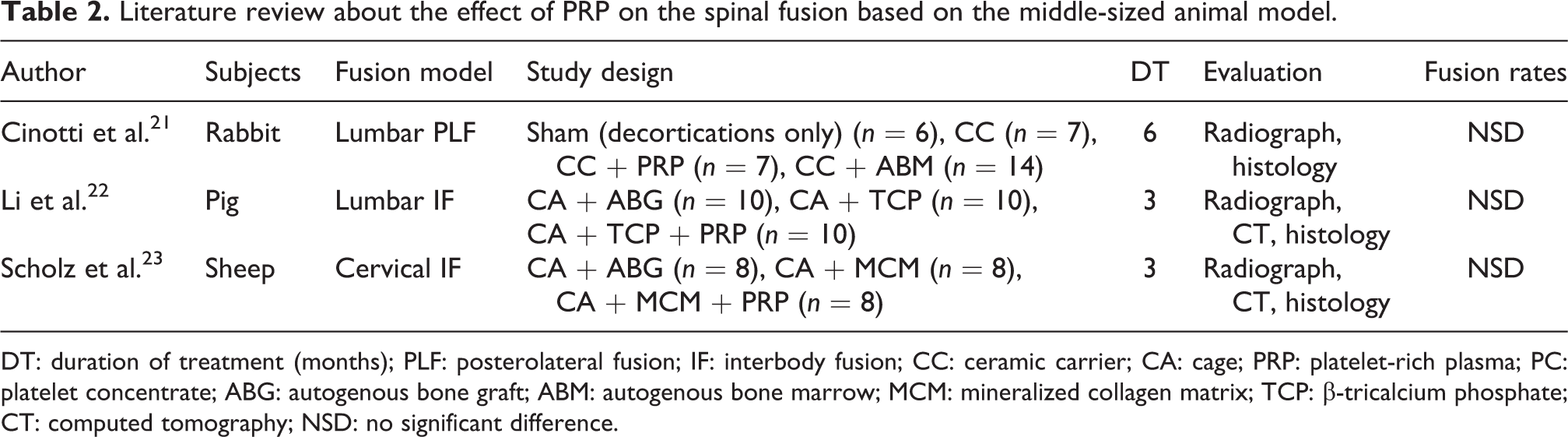
DT: duration of treatment (months); PLF: posterolateral fusion; IF: interbody fusion; CC: ceramic carrier; CA: cage; PRP: platelet-rich plasma; PC: platelet concentrate; ABG: autogenous bone graft; ABM: autogenous bone marrow; MCM: mineralized collagen matrix; TCP: β-tricalcium phosphate; CT: computed tomography; NSD: no significant difference.
Literature review about the effect of PRP based on the human spinal fusion studies.

FU: follow-up period (months); PLF: posterolateral fusion; IF: interbody fusion; ABG: autogenous bone graft; CA: cage; PRP: platelet-rich plasma; CT: computed tomography; NSD: no significant difference; SD: significant difference.
Studies based on the small-sized animal model
Kamoda et al. 18 investigated using rat models the effect of PRP on spinal fusion. Fifty rats underwent lumbar posterolateral fusion (PLF), which were divided into three groups including the sham group with only surgical dissection (n = 10), PRP group with autogenous coccygeal bone graft and the use of PRP (n = 20), or normal arthrodesis group with autogenous coccygeal bone graft (n = 20). Bony fusion was evaluated by microcomputed tomography examination and histological analysis at the final follow-up of 2 months after operation. At 8 weeks, 7 of 10 rats in the normal arthrodesis group and 9 of 10 rats in the PRP group were considered to have achieved fusion (p = 0.27).
His group investigated its effect on the lumbar IF. Twenty-eight rats underwent lumbar IF with hydroxyapatite (HA) granules 19 and were divided into four groups including sham group with only surgical dissection (n = 7), group treated with HA granules and PRP (n = 7), group treated with HA granules and platelet-poor plasma (PPP, supernatant; n = 7), and group treated with HA granules only (n = 7). Bony fusion was evaluated by radiographic and histological analyses at the final follow-up of 3 months after operation. At 3 months after operation, all seven rats in the group treated with HA granules and PRP achieved bone union. In contrast, in the group treated with HA granules and PPP, only 1 (17%) of the 7 rats achieved bone union, and in the group treated with HA granules no rats achieved bone union. The group treated with HA granules and PRP showed bone formation compared with the group treated with HA granules only (p < 0.05) and the group treated with HA granules and PPP (p < 0.05). 19
However, Rao et al. 20 found no stimulating effect of PRP based on the rat model of lumbar PLF, which were divided into four groups including the sham group with only surgical dissection (n = 10), the group treated with rhBMP-2 and PRP (n = 10), the group treated with rhBMP-2 and autogenous bone marrow (ABM; n = 10), and the group treated with rhBMP-2 (n = 10). Bony fusion was evaluated using radiographic analysis, microcomputed tomography examination, and histological analysis at the final follow-up of 1 month after operation. The sham group with only surgical dissection showed no evidence of spinal fusion. The rate of fusion was radiographically and histologically similar in all three experimental groups. The area, volume, and density of the fusion mass for the group treated with rhBMP-2 and ABM were greater (p < 0.05) compared with the group treated with rhBMP-2. The group treated with rhBMP-2 and PRP had intermediate fusion area. In contrast to Kamoda’s result, 18,19 the group treated with rhBMP-2 and PRP did not show bone formation compared with the group treated with rhBMP-2.
Studies based on the middle-sized animal model
All three studies used a combination of radiographic and histologic assessments to obtain the fusion rate. All 3 studies found that PRP did not promote spinal fusion rate (Table 2).
In the model of lumbar PLF, rabbits were divided into four groups including sham group with only surgical dissection (n = 6), group treated with ceramic carrier (CC) (n = 7), group treated with CC and PRP (n = 7), and group treated with CC and ABM (n = 14). 21 At the final follow-up of 6 months after operation, the radiographic analysis showed a fusion rate of 86% in the group treated with CC and PRP and group treated with CC and ABM and a fusion rate of 71% in the group treated with CC. In the PRP group, there was no evidence of increased vascular density in the grafted material. Therefore, PRP did not promote spinal fusion rate.
The other studies used IF model using either lumbar or cervical spine. 22,23 Li et al. 22 investigated its effect based on pig model of lumbar IF with carbon fiber cage. They were divided into three groups including the group treated with ABG (n = 10), the group treated with β-tricalcium phosphate (β-TCP; n = 10), and the group treated with β-TCP and PRP (n = 10). At the final follow-up of 3 months after operation, the radiographic analysis showed 70% (7/10) fusion rate in the group treated with ABG. At all the levels, the group treated with β-TCP and PRP showed partial fusion, while the group treated with β-TCP had six partial fusions and four nonfusions (p = 0.08). The study showed that the addition of PRP did not increase bone formation compared with the results of group treated with β-TCP.
Scholz et al. 23 investigated its effect based on sheep model of cervical IF with cylinder-design titanium cage. They were divided into three groups including the group treated with ABG (n = 8), the group treated with mineralized collagen matrix (MCM; n = 8), and the group treated with MCM and PRP (n = 8). At the final follow-up of 3 months after operation, the study showed that the results of the group treated with MCM or the group treated with MCM and PRP were inferior to that of group treated with ABG.
Studies based on the human models
Six clinical studies investigated the effect of PRP on the lumbar PLF (Table 3). 24 –29
In three of the six clinical studies, the group treated with autogenous iliac bone graft represented the control group. 24,25,29 In the other three clinical studies, the group treated with autogenous laminar or heterologous cancellous bone graft represented the control group. 26 –28 All of the six studies evaluated bony fusion with the radiograph or computed tomography (CT) at the follow-up period between 12 and 24 months after operation. Five of the six studies found that PRP did not promote spinal fusion rates. However, one recent study found PRP did promote spinal fusion rates. 27 In the prospective controlled trial, the study population was composed of two groups including the group treated with autogenous laminar bone and PRP (n = 25) and the group treated with autogenous laminar bone alone (n = 25). 27 Bony fusion was evaluated with radiograph and CT at the final follow-up of 24 months after operation. 27 They found that PRP enhanced bony fusion in the human spinal fusion model. 27
Four clinical studies investigated its effect on the IF of lumbar spine, 30 –32 thoracic spine, 32 or cervical spine (Table 3). 33 In two of the four clinical studies, additional PLF was performed. 31,32 In two of the four clinical studies, the group treated by the cage filled with autogenous iliac bone graft represented the control group. 30,31 In another clinical study, the group treated by the cage filled with ABG drawn from the fractured vertebrae represented the control group. 32 All of the three studies evaluated bony fusion with radiograph or CT at the follow-up period between 8 and 24 months after operation. All of them found that PRP did not promote spinal fusion rates.
In the other clinical study, the group treated by cortical allograft bone only represented the control group. 33 Study population was divided into two groups including the group treated with allograft bone and PRP (n = 42) and the group treated with an allograft bone alone (n = 39). Bony fusion was evaluated with radiograph at the final follow-up of minimum 24 months after operation. They found that PRP did not promote spinal fusion.
Platelet count and concentration of growth factor in the studies on PRP
Five animal and two clinical studies showed the platelet count and the concentration of growth factor in the peripheral blood and PRP (Tables 4 and 5). 18,19,21 –24,27 In the rat model, PRP had stimulating effect if the platelet count of PRP is five times that of peripheral blood. 18,19 However, in the middle-sized animal model, PRP had no stimulating effect even if the platelet count of PRP is five times that of peripheral blood. 21 –23 In the human clinical studies, PRP had no stimulating effect if the platelet count of PRP is five times that of peripheral blood. 24 It had stimulating effect if the platelet count of PRP is 10 times that of peripheral blood or the concentration of growth factor of PRP is 100 times that of peripheral blood. 27
Literature review about the platelet count and concentration of growth factor in the peripheral blood and PRP based on the animal model.
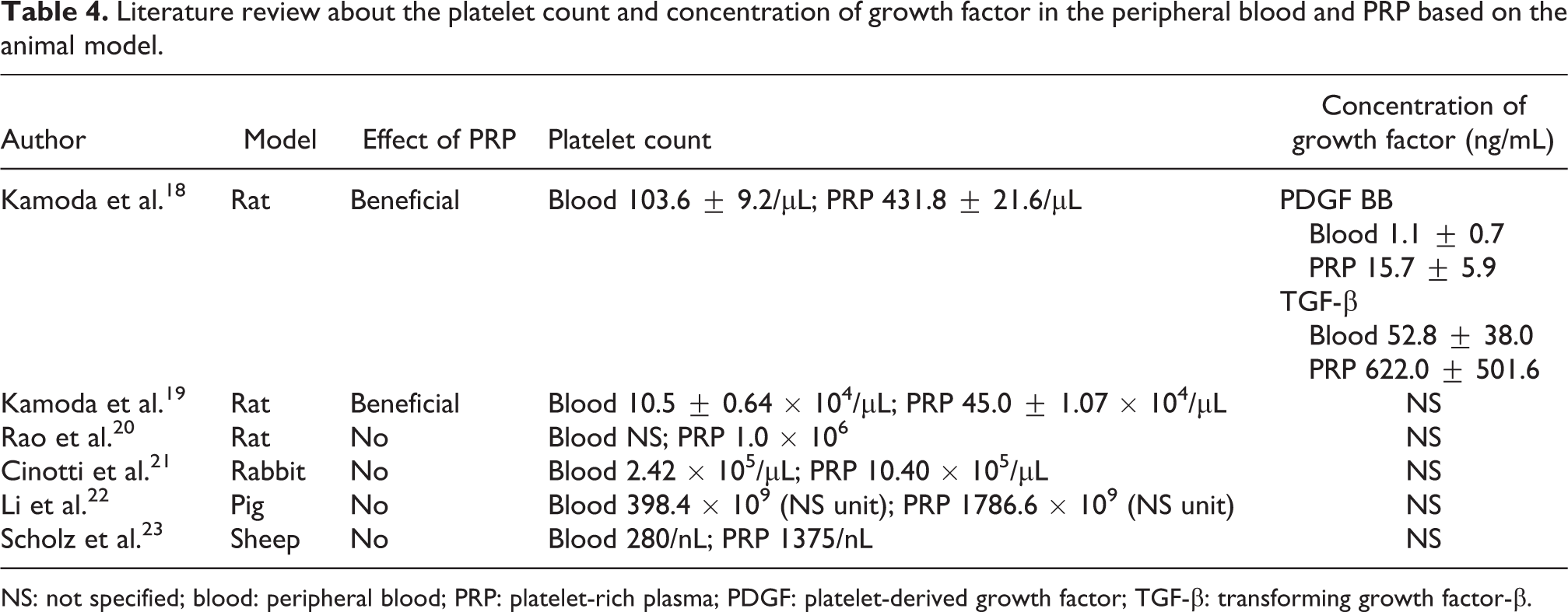
NS: not specified; blood: peripheral blood; PRP: platelet-rich plasma; PDGF: platelet-derived growth factor; TGF-β: transforming growth factor-β.
Literature review about the platelet count and concentration of growth factor in the peripheral blood and PRP based on the human spinal fusion studies.

NS: not specified; Blood: peripheral blood; PRP: platelet-rich plasma; PDGF: Platelet-derived growth factor; TGF-β: transforming growth factor-β.
Discussion
There have been two review papers regarding the effect of PRP on spinal fusion based only on clinical studies. However, based on both animal model studies and clinical studies, there are no review studies regarding its effect on spinal fusion and no review studies focusing on the platelet count and the concentration of the growth factor in the PRP. There are literature reviews about the effect of PRP on spinal fusion based on the animal model studies and clinical studies, focusing on the effect of the platelet count and the concentration of the growth factor in the PRP.
In the current review, the results of spinal fusion applications are controversial in the small-sized animal model studies of rats. Both beneficial and inhibitory effects were found in the studies based on the animal model and clinical studies. PRP had stimulating effect if the platelet count or the concentration of growth factor in the PRP is much higher than those in the peripheral blood.
This might be explained by the fact that PRP might not have the stimulating effects continuing for longer follow-up period in the middle-sized animal model studies and the clinical studies compared to the short follow-up period of the small-sized animal model study. In addition, the concentration of PRP might have to be increased in the middle-sized animal model studies and the clinical studies because the weight of middle-sized animals and human beings is much heavier than that of the small-sized animal.
There have been controversies over the optimal concentration of growth factor to promote bone fusion. Kamoda et al. 18 suggested that to elicit its stimulating effect the PRP needed to be of four- to fivefold concentrate compared to its concentration of whole blood in a rat model. Carreon et al. 25 suggested that the concentration of PDGF or TGF should be more than 10 times the concentration of whole blood to get the bony fusion in the human spinal fusion model. Kubota et al. 27 found that the concentration of PDGF should be more than 100 times the concentration of whole blood to get the bony fusion.
Based on clinical studies only, Miyazaki et al. 12 updated the bone substitutes for spinal fusion. Similarly with the current study, they reached to the conclusion that the clinical use of PRP for the spinal fusion did not promote spinal fusion. Sheth et al. 13 performed meta-analysis about the efficacy of PRP. Similar to Miyazaki’s conclusion, 12 there is uncertainty about the evidence to support the clinical use of PRP for the spinal fusion. The PRP and control groups were similar with regard to solid fusion. 13 However, both of them had evaluated only clinical studies and did not compare the animal studies to clinical studies.
As with any study, the present investigation has several limitations. Our analysis was limited by variability among the studies with respect to the study designs in spite of selecting only retrospective case–control or prospective randomized studies. However, it is the first review article evaluating the effect of PRP on spinal fusion based on both animal and clinical studies.
Conclusion
The stimulating effect of PRP on spinal fusion is still not concluded. However, PRP might promote human spinal fusion if the platelet count or the concentration of growth factors in the PRP increases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.