
Abstract
Background
This study aims to investigate the impact of varying coronal alignments of femoral prostheses on stress and strain distributions within the lateral compartment following unicompartmental knee arthroplasty (UKA) in patients with normal bone density and osteoporosis using finite element analysis. Additionally, it examines the relationship between osteoporosis and the progression of osteoarthritis in the lateral compartment postoperatively.
Methods
UKA models were developed for both normal bone and osteoporotic conditions using a validated finite element model of the knee. Seven alignment conditions for the femoral prosthesis were simulated: 0° (neutral alignment), varus angles of 3°, 6°, and 9°, and valgus angles of 3°, 6°, and 9°, resulting in a total of 14 scenarios. Stress and strain distributions in the meniscus, tibial cartilage, and femoral cartilage of the lateral compartment were evaluated.
Results
The results indicated that stress and strain in the meniscus, tibial cartilage, and femoral cartilage of the lateral compartment increased with greater varus alignment and decreased with greater valgus alignment in both normal and osteoporotic models. At equivalent alignment angles, stress and strain were consistently higher in the osteoporotic model (M2) compared to the normal bone model (M1), although the peak equivalent stress in the tibial cartilage was lower in the M2 model than in the M1 model.
Conclusions
In patients with osteoporosis undergoing fixed-bearing medial UKA, varus malalignment of the femoral prosthesis can lead to increased stress and strain in the lateral compartment’s meniscus, tibial cartilage, and femoral cartilage. These findings suggest that osteoporosis may contribute to abnormal stress and strain distributions in the lateral compartment following UKA, potentially accelerating the progression of osteoarthritis in this region postoperatively.
Background
Unicompartmental knee arthroplasty (UKA) is widely used as a knee-preserving procedure for the treatment of isolated medial compartment knee osteoarthritis (KOA), with favorable early outcomes. 1 Its potential advantages include a more natural gait, improved range of motion, preservation of more bone mass, and faster recovery. 2 Despite these advantages over total knee replacement (TKA), UKA has a higher revision rate, primarily due to postoperative complications such as progression of osteoarthritis in the lateral compartment, postoperative pain, and periprosthetic fracture and loosening.3,4 Osteoarthritis of the lateral compartment is particularly common in the mid- and late postoperative periods, with a prevalence of approximately 38% in the mid-period and 40% in the late period. This condition is considered an irreversible complication after UKA and a significant cause of revision. 4
Additionally, UKA is a technically demanding procedure requiring precise osteotomy and prosthesis positioning. Misalignment of the prosthesis is strongly associated with postoperative complications.5–7 Previous studies have shown that prosthesis misalignment can lead to changes in contact patterns and increased stress. Such complications, including the progression of osteoarthritis in the lateral compartment, may result from altered stress patterns in the bone and cartilage. 8 However, prior biomechanical studies have primarily focused on tibial prosthesis placement and stress analysis on the operative side, neglecting the stress and strain on the lateral compartment structures following femoral prosthesis misalignment, including the effects on meniscus, tibial cartilage, and femoral cartilage.9,10
Patient factors, such as osteoporosis, significantly influence the survival of unicondylar replacements. Osteoporosis is common among patients with KOA and is often comorbid in elderly patients undergoing prosthetic arthroplasty.11–13 While osteoporosis is not explicitly mentioned in the indications for UKA, bone loss is strongly associated with postoperative complications. 14 Previous studies have mainly focused on individuals with normal bone mass, assessing stress on the operated structures after UKA.15–17 In light of osteoporosis and prosthesis misalignment, this study raises the question: does prosthesis misalignment exacerbate the progression of postoperative osteoarthritis in the lateral compartment in patients with osteoporosis?
In this study, a parametric modeling approach was employed to assess the biomechanical effects of femoral prosthesis misalignment on the structure of the lateral compartment after UKA in osteoporotic patients. Specifically, normal and osteoporotic knee joints were modeled using fixed platform prostheses, with adjustments to the coronal plane position of the femoral prosthesis to create varus and valgus UKA models in different bone quality groups. This study aims to analyze the effects of various femoral prosthesis positions on the stress and strain of the lateral compartment structure post-UKA in patients with normal bone and osteoporosis. Furthermore, it investigates the correlation between osteoporosis and postoperative osteoarthritis of the lateral compartment to provide clinical practice insights.
Materials and methods
Location of the experiment: Xinjiang Medical University
Establishment of normal bone intact knee joint model
This study was conducted on a 34-year-old healthy male subject who provided informed consent. The study received approval from the Ethics Committee of the Sixth Affiliated Hospital of Xinjiang Medical University. The experiments were performed in the orthopedic laboratory of the Sixth Affiliated Hospital of Xinjiang Medical University. Anatomical reconstruction was based on the subject’s computed tomography (CT) and magnetic resonance imaging (MRI) scans. Radiographs indicated a neutral position of the subject’s right lower extremity knee joint, with no pathological changes or planning abnormalities. Medical imaging was performed using a 64-row spiral CT scanner (Siemens, Germany) and a 3.0 T MRI scanner (Siemens, Germany).
The slice thicknesses for the CT and MRI scans were 1 mm and 0.6 mm, respectively. CT data were used to reconstruct the bone structure, while MRI data were utilized to reconstruct the soft tissue structures. The selection range included 15 cm above and below the center of the knee joint.
Material parameters of the knee joint structure.

Model validation methods
Model validation was conducted based on two methods referenced from previous literature: the axial stress experiment and the anterior drawer experiment.15,18 In the axial stress experiment, a 1000 N axial load was applied above the femur, perpendicular to the midpoint of the medial and lateral condyles (the center of the knee joint). In the anterior drawer experiment, a forward load of 130 N was applied to the tibia at the center of the knee joint. The load distribution of the medial and lateral compartments during axial loading and the anterior tibial displacement distance during the anterior drawer experiment were compared to existing literature to validate the finite element model.
Establishment of UKA models with different femoral prosthesis inclination angles for normal bone and osteoporotic knees
LINK prosthetic material parameters.


Finite element models of UKA with different varus and varus angles of femoral prosthesis.
Observation indices
The observation indices included the peak equivalent stress (von Mises stress) and peak minimum principal stress (compressive stress) of the meniscus, tibial cartilage, and femoral cartilage, as well as the peak strain of the meniscus and tibial cartilage. In the experiment, upward is defined as positive and downward as negative; therefore, the minimum principal stresses and strains are taken as the maximum of their absolute values.
Results
Model validation results
The model comprised a total of 528,624 nodes and 312,573 elements. Under axial loading experiments, the load distribution between the medial and lateral compartments was 58.6% and 41.4%, respectively. The anterior tibial displacement at the center of the knee moved forward by 4.9 mm during the anterior drawer experiment. These results closely matched those reported in the literature, confirming the model’s validity.15,22
Changes in peak stresses in the lateral compartment structure in the osteoporotic group
In the M2 group models, stress concentrations in the meniscus were primarily located at the anterior and posterior horns, with the anterior horn being more significant. The equivalent stress and the minimum principal stress of the meniscus increased with increasing varus angles of the femoral prosthesis and decreased with increasing valgus angles. Specifically, the equivalent stress increased by 4.3%, 6.4%, and 8.2% at varus angles of 3°, 6°, and 9°, respectively, compared to 0° (Figure 2). Stress in the tibial cartilage was mainly concentrated in the medial region of the mid-upper part. The equivalent stress and minimum principal stress of the tibial cartilage increased with increasing varus angles of the femoral prosthesis and decreased with increasing valgus angles. The equivalent stress increased by 2.9%, 3.9%, and 8.9% at varus angles of 3°, 6°, and 9°, respectively, compared to 0° (Figure 3). The equivalent stress and minimum principal stress of the femoral cartilage increased with increasing varus angles of the femoral prosthesis and decreased with increasing valgus angles. The equivalent stress increased by 1.1%, 1.6%, and 3.0% at varus angles of 3°, 6°, and 9°, respectively, compared to 0°. Peak value and distribution of meniscus in two model groups. Peak value and distribution of minimum principal stress of tibial cartilage in two model groups.

Comparison of peak stress changes in each structure between the two groups
For the meniscus, the equivalent stress and minimum principal stress for each varus/valgus angle in the M2 group were greater than those in the M1 group (Figures 2 and 4). For the tibial cartilage surfaces, the equivalent stress for each varus/valgus angle in the M2 group was less than that in the M1 group, but the minimum principal stress in the M2 group was greater than in the M1 group (Figures 3 and 5). For the femoral cartilage, the equivalent stress and minimum principal stress for each varus/valgus angle in the M2 group were greater than those in the M1 group (Figure 6). Stress change of the meniscus with different femoral prosthesis positions in two model groups. A: peak equivalent stress(von mises stress), B: peak minimum principal stress. Stress change of the tibial cartilage with different femoral prosthesis positions in two model groups. A: peak equivalent stress, B: peak minimum principal stress. Stress change of the femoral cartilage with different femoral prosthesis positions in two model groups. A: peak equivalent stress, B: peak minimum principal stress.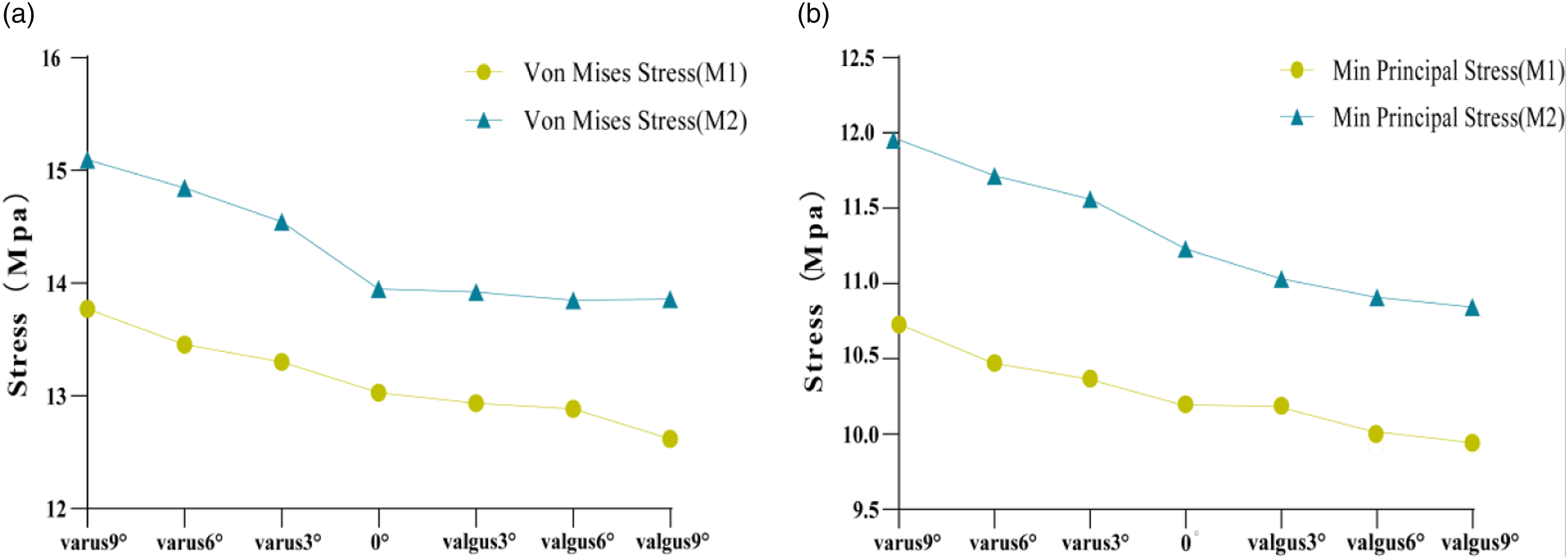


Peak strains of meniscus and tibial cartilage
The sites of strain concentration in the meniscus and tibial cartilage of the UKA models in both groups were consistent with the sites of stress concentration. Meniscus and tibial cartilage strains increased with increasing varus angles of the femoral prosthesis and decreased with increasing valgus angles in both groups. Compared with 0°, meniscal strain in the M2 group increased by 0.8%, 1.9%, and 4.8% at varus angles of 3°, 6°, and 9°, and decreased by 0.3%, 1.3%, and 2.4% at valgus angles of 3°, 6°, and 9°, respectively. For the same femoral prosthesis angle, the meniscus and tibial cartilage strains were greater in the M2 group than in the M1 group. Compared to the M1 group, the mean increase or decrease in meniscus strain for each angle was 1.4%, and the mean increase or decrease in tibial cartilage strain was 30.8% in the M2 group (Figure 7). Strain variations for different structures with different femoral prosthesis positions in two model groups. (a) meniscus. (b) tibial cartilage.
Discussion
Despite the unique clinical advantages of unicompartmental knee arthroplasty (UKA), its long-term survival rates are inferior to those of total knee arthroplasty (TKA). Patient selection and prosthesis positioning are critical factors affecting the prognosis of UKA. Both osteoporosis and prosthesis misalignment have been suggested to contribute to postoperative internal knee stress abnormalities. However, whether these factors contribute to the progression of postoperative osteoarthritis in the lateral compartment remains unclear. This study demonstrated that stress and strain in the meniscus, tibial cartilage, and femoral cartilage of the lateral compartment increased with greater varus angles of the femoral prosthesis and decreased with greater valgus angles. At the same angle of inclination, the stresses and strains in the M2 (osteoporotic) group were greater than those in the M1 (normal bone) group, except for the equivalent stresses in the tibial cartilage, which were smaller in the M2 group.
In the M2 group model, stresses on the meniscus, tibial cartilage, and femoral cartilage of the lateral compartment increased with greater varus angles and decreased with greater valgus angles. One reason for this may be that the contact area between the femoral cartilage and the tibial component of the lateral compartment increases with increasing varus angles and decreases with increasing valgus angles.2,15 Another reason may be that in osteoporosis, the elastic modulus of both cortical and cancellous bone decreases, reducing the stress they bear. This reduced stress is transferred to other structures, increasing the contact stress between the lateral compartment structures and the surgical side structures.16,23 A third reason may be the misalignment of the femoral prosthesis, which changes the load distribution between the medial and lateral compartments. Varus angles increase the load on the lateral compartment, while valgus angles decrease it, combined with the antagonism of the lateral collateral ligaments in valgus angles. 24 Previous studies have confirmed increased stresses on the polyethylene (PE) insert and cancellous bone under the prosthesis during varus angles. Although valgus alignment decreases stress on the lateral compartment structures, it increases stress on the structures on the operative side and affects knee stability.
This study also found that the stresses in the meniscus and femoral cartilage were greater in the M2 group models than in the M1 group models at the same femoral prosthesis tilt angle. The minimum principal stress in the tibial cartilage was also greater in the M2 groups than in the M1 groups. This may be due to stress shifting in osteoporosis, where the lateral compartment absorbs some of the shifted stresses, resulting in increased stresses in the meniscus and femoral cartilage.16,23 Additionally, the meniscus and articular cartilage have low elastic moduli of 59 MPa and 10 MPa, respectively. In osteoporosis, their ability to convert stress into elastic potential energy increases, and the confrontation of elastic stresses may result in an increase in the minimum principal stress. However, the equivalent stresses in the tibial cartilage in the M2 group models were less than those in the M1 group models. Osteoporosis leads to changes in the functional units of cartilage and subchondral bone. Subchondral bone, with its greater stiffness and strength than the overlying cartilage, absorbs most of the stress transmitted from the articular surfaces. Reduced density of the subchondral bone, with its reduced ability to dissipate loading stresses, may result in lower equivalent stress in the tibial cartilage, which is detrimental to maintaining cartilage homeostasis. 25
In this study, the strains in the meniscus and tibial cartilage were greater in the M2 (osteoporotic) groups compared to the M1 (normal bone) groups for each inclination angle, and the sites of major strains were consistent with the sites of major stresses. In osteoporosis, the meniscus and tibial cartilage, which are the primary load-bearing structures, endure more stress transferred to the lateral compartment, resulting in increased strain. The lateral meniscus, which is “O”-shaped with a high lateral margin and a low medial margin, primarily experiences strain in the anterior horn edge region where it contacts the femoral cartilage. This, combined with a poorer blood supply to the medial two-thirds compared to the lateral side, can lead to meniscal tearing and abrasion. The tibial cartilage, compared to the meniscus, experiences greater strain due to several factors: stress transfer in osteoporosis, a larger contact area with the femoral cartilage, and the main site of strain being located in the medial region of the mid-upper portion of the bone just below the intercondylar eminence.26–32
Osteoporosis makes the structures of the lateral compartment more sensitive to femoral prosthesis misalignment, resulting in abnormal stress and strain. To improve prosthesis positioning, computerized navigation systems can be utilized, which combine computer technology and imaging to enable real-time tracking and positioning of the prosthesis during surgery. For example, the MAKO robotic arm system allows for the reestablishment of the flexibility of independent gaps through implantation and alignment correction, balancing soft tissue tension for functional stability. Both intramedullary femoral guided instrumentation (IM) and ligamentous tensor-guided extramedullary orientation (FuZion®) improve the accuracy of prosthesis fitting and better equalize the pressure between the two compartments. For treating osteoporosis after arthroplasty, some medications have shown promise, such as bisphosphonates, estrogens and estrogen receptor agonists, calcitonin, and gene therapy, although extensive studies are still required to confirm their efficacy.
This study has several advantages. Firstly, the osteoporotic knee model and postoperative model were established by adjusting the parameters to reflect the actual conditions of patients and compared with normal bone. Secondly, two different stress patterns (Equivalent Stress and Min-Principal Stress) were observed, as well as the degree of strain on the structures. Finally, in contrast to previous UKA studies, this study focused on the effect of prosthesis position on the structures of the lateral compartment.
However, this study has some limitations. First, the finite element (FE) model was based on imaging data from a single volunteer, which may not represent the variability seen in a broader population. Second, the effects of anisotropy and viscoelasticity were not considered for the articular cartilage, which may affect the accuracy of stress and strain predictions. Third, the study only analyzed the forces under vertical static loading and did not include dynamic simulations such as knee flexion and rotation. Finally, this study focused solely on changing the position of the femoral prosthesis in the coronal plane and did not analyze conditions such as translation, rotation, forward flexion, and backward roll, nor did it change the position of the tibial prosthesis. These aspects will be the subject of future studies.
Conclusions
In osteoporotic knees undergoing medial fixed platform unicompartmental knee arthroplasty (UKA), varus malalignment of the femoral prosthesis may lead to increased stress and strain in the meniscus, tibial cartilage, and femoral cartilage of the lateral compartment. Compared with normal bone, osteoporosis may exacerbate these stress and strain levels in the affected structures. The findings confirm that osteoporosis contributes to abnormal stresses in the lateral compartment structures post-UKA, which may, in turn, accelerate the progression of osteoarthritis in the lateral compartment during the postoperative period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.