
Abstract
Background
To compare the safety and clinical outcomes of 3D-printed guides versus computer navigation for pedicle screw placement in the correction of congenital scoliosis deformities.
Methods
The study was a single-centre retrospective controlled study and was approved by the hospital ethics committee for the analysis all patients under the age of 18 years with at least 2 years of follow-up. Sixty-three patients who underwent surgical correction for congenital scoliosis deformities in our hospital from January 2015 to December 2020 were divided into two groups based on the decision following preoperative doctor‒patient communication. Among them, 43 patients had pedicle screws placed with 3D-printed guider plates, while the remaining 20 patients had screws inserted with the assistance of computer navigation. The perioperative period, follow-up results and imaging data were compared between the groups.
Results
The operation was completed successfully for patients in both groups. The 3D-printed guide-assisted screw placement technique proved to be significantly superior to the computer navigation technique in terms of operation time, screw placement time, and intraoperative blood loss (p < .05), although the former had more frequent intraoperative fluoroscopies than the latter (p < .05). The mean follow-up time was 41.4 months, and the SRS-22 scores significantly improved in both groups over time postoperatively (p < .05). The 3D-printing group had better SRS-22 scores than the navigation group 6 months after surgery and at the last follow-up (p < .05). Compared with preoperative values, the coronal Cobb angle, local kyphotic Cobb angle, C7-S1 coronal deviation (C7PL-CSVL), and sagittal deviation (SVA) were significantly improved in both groups after surgery (p < .05).
Conclusion
Both techniques achieve the purpose of precise screw placement and proper correction of the deformities. In contrast, the 3D-printed guide-assisted screw placement technique showed advantages in terms of operation time, screw placement time, intraoperative blood loss and patient satisfaction with outcomes.
Introduction
In 1959, Boucher was the first to use pedicle structures to drive screws, and in the 1990s, Professor Suk 1 in Korea pioneered the use of pedicle screws for scoliosis, which became the predominant fixation method for scoliosis implant fusion with good correction, a low incidence of pseudoarthrosis, and secure three-column fixation.2–4 However, in congenital scoliosis, it is difficult to place pedicle screws due to anatomical changes such as the narrowing and rotation of the pedicle. 5 Poorly positioned pedicle screws can lead to several complications, such as nerve and vascular injury. 6 The precise placement of pedicle screws becomes the key to the success or failure of this procedure, and for this reason, various assisted screwing techniques and equipment have emerged, including 2D/3D navigation-assisted screwing, portable electronic navigation openers for screwing, guide plate-assisted screwing, and fluoroscopy-assisted screwing. The high accuracy, safety and reliability of CT navigation-assisted stapling have been reported in the literature.7,8 However, the CT navigation technique is associated with disadvantages such as a complicated operation, expensive equipment and long operation time. With the rapid development of digital orthopaedics in recent years, the 3D-printed guide-assisted screw placement technique has been increasingly used in orthopaedic surgery for the treatment of spinal deformities because of its simplicity and because no special equipment is required. 9
A total of 63 patients with congenital scoliosis were treated with 3D-printed guide-assisted screwing and CT navigation-assisted screwing in our hospital over a period of 6 years. In this paper, the safety and clinical efficacy of the two techniques are compared in detail, and their respective advantages and disadvantages are summarized and reported as follows.
Materials and methods
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) age ≤18 years; (2) a diagnosis of congenital scoliosis; and (3) complete case information.
Exclusion criteria were as follows: (1) the presence of congenital heart disease, renal insufficiency, etc.; (2) the presence of haematologic disorders resulting in abnormal coagulation function, etc.; and (3) less than 2 years of follow-up;
General information
Comparison of preoperative general data between the groups.

Surgical methods
After the installation of the spinal cord monitoring device, routine disinfection and towel laying, and according to the preoperative surgical design, surgeons were assisted by a 3D-printed guide plate and CT computer navigation for spinal pedicle screw placement.
Guide plate-assisted method: A thin layer CT scan was performed on the patient’s spine, and the original data obtained from the CT scan were imported into the 3D reconstruction software Mimics 10.01 (Materialise, Belgium) in the DICOM format. First, the original mask of the corresponding segment of the spine was obtained by using the threshold selection technique. Second, the structural gap holes resulting from the data conversion were repaired by using the filling technique, and a new mask was obtained. Then, the 3D reconstructed images of the selected structural region were obtained in the 3D reconstruction option. In the MedCAD module, a 4 mm diameter cylinder was used instead of the screw to design the pedicle screw insertion trajectory, and the roller was slowly dragged to observe the relationship between the position of the cylinder through the corresponding bony structures of the pedicle in the 3D interface, axial plane, and sagittal plane. Then, the preliminary design of the screw insertion trajectory was completed, and the model data were saved in STL format. The saved data in UG Imageware software (EDS, USA) were opened, and whether the screw path penetrated the bone cortex from all angles was observed, with fine-tuning if necessary to ensure the safety and accuracy of the screw path. According to the axis line of the design track, the diameter of the screw path was reset to 2.8 mm, the outer diameter of the guide plate screw path was set to 7 mm, and the height was set to 30 mm to complete the design of the directional tube of the guide template. Then, the anatomical data corresponding to the posterior bony surface of the vertebral plate were extracted and reverse thickened by 2.5 mm to create a reverse substrate with the same morphology, the screw tract data were imported, and the two were combined to reconstruct the prototype of the guide plate (the external screw tract was not penetrated) to form an individualized navigation template for pedicle screws with bilateral positioning tubes. In addition, the directional duct was removed, leaving only the substrate part and the 2.8 mm diameter directional hole to complete the design of the fixed-point guide plate. Using photosensitive resin material, the individualized physical guide plate and 3D solid model of the spine were produced. The process of screw placement assisted by 3D guide plate is shown in Figure 1. Detailed procedure of screw placement assisted with 3D printed guide plate. (a): Equip the 3D printed guide plate with the 3D printed spine model to get general placement of the guide plate. (b): Match the 3D printed guide plate with the vertebral plate and other structures to make it fit as closely as possible. (c, d): Using an electric drill, the screw path of the appropriate thickness of the Steinmann pin extension guide plate was driven into the pedicle with a depth of about 2–3 cm. (e): Unscrew the inserted Steinmann pin to complete the preliminary screw path, expand it and screw into the appropriate pedicle screw.
Navigation operation: After exposure, the reference frame was fixed on the spines of the adjacent segments of the operation, and the X-ray machine was used for positioning and confirmation. The point matching method was used to select at least six points on the posterior spine surface with a well-defined bony structure. A guide rod was used to contact the articular protrusion so that it overlapped with the anatomical point of the vertebral arch. on the anterolateral 3D images of the spine. Guided by the navigation system, the screw entry position, direction and depth were determined to complete the screw path.
After screw placement, the vertebral spine was repositioned, and the spinal cord was closely monitored. The corresponding hemivertebral body resection or osteotomy was performed. Ponte osteotomy and bending rod orthosis were performed at the necessary segments according to the specific situation, bone grafting and fusion were performed at the corresponding segments, and the wound was closed layer by layer.
Evaluation indicators
Perioperative data were recorded, including operative time, screw placement time, bleeding volume, intraoperation transmission times, incision length, postoperative drainage, and length of hospital stay. Clinical outcomes were assessed using the Scoliosis Research Society (SRS-22) score. Image examination was performed to determine the accuracy of screw placement according to Gertzbein ∼ Robbins grading criteria. 10 Grades A and B were considered accurate screw placement. Scoliosis and local kyphosis angles, C7-S1 coronal offset (i.e., C7PL-CSVL, horizontal distance between the C7 plumb line and the midsacral perpendicular line), sagittal offset (SVA; i.e., the horizontal distance between the C7 plumb line and the posterior upper corner of the endplate of the upper sacral body), etc., were measured.
Statistical processing
Statistical software SPSS19.0 was used to analyse the data. The measurement data were expressed as (x ± s), and when the data were normally distributed, an independent sample t test was used for comparisons between two groups, and a paired t test was used for comparisons between two time points within groups; when the data were not normally distributed, a rank sum test was used. Count data were tested using the χ2 test or Fisher’s exact test. Grade data were compared between the groups using the Mann‒Whitney U test. Differences for which the p value was <0.05 were considered statistically significant differences.
Results
Perioperative conditions
Malpositioned screws by level and direction.

Perioperative data (x ± s) and comparison between the groups of patients.


Female, 13 years, 10 months. (a, b): Preoperative appearance, child’s height 127 cm, weight 26 kg, BMI 16.1. (c): Preoperative anteroposterior radiographs, showing a main bend Cobb angle of 132°, C7PL-CSVL:10.7 mm. (d): Preoperative lateral radiographs, measuring a localized posterior convex Cobb angle of 103°, SVA:32.6 mm. (e): Preoperative 3D CT reconstruction showing multiple thoracic vertebral body developmental malformations. (f): 3D-printed guide design, reconstruction of the 3D structure of the spine based on CT scan data, and creation of individualized guides. (g): Postoperative anteroposterior X-ray film, measured main bend Cobb angle: 30°, main bend correction rate was 77.27%; C7PL-CSVL was 2.5 mm. (h): Postoperative lateral radiographs, measured local kyphosis Cobb Angle 42°, correction rate 59.22%; the SVA was 12.3 mm.

Postoperative 3D CT data showing the location of each pedicle screw in the above typical case. (f): This figure showing that the right pedicle screw of T10 breached the inner wall of the pedicle by approximately 4.1 mm, which was judged as grade D screw placement according to the Gertzbein-Robbins criteria. (a-e, g-k): these figures showing that the rest of the pedicle screws determined to have grade A or B placement. The accuracy rate of screw placement in this case was 94.7%.
Follow-up results
Follow-up information (x ± s) and comparison between the groups of patients.

p value*: Comparison between 6 months and 1 month after surgery/comparison between the last follow-up and 6 months after surgery.
Imaging evaluation
Image measurement results (x ± s) and comparison between the groups.
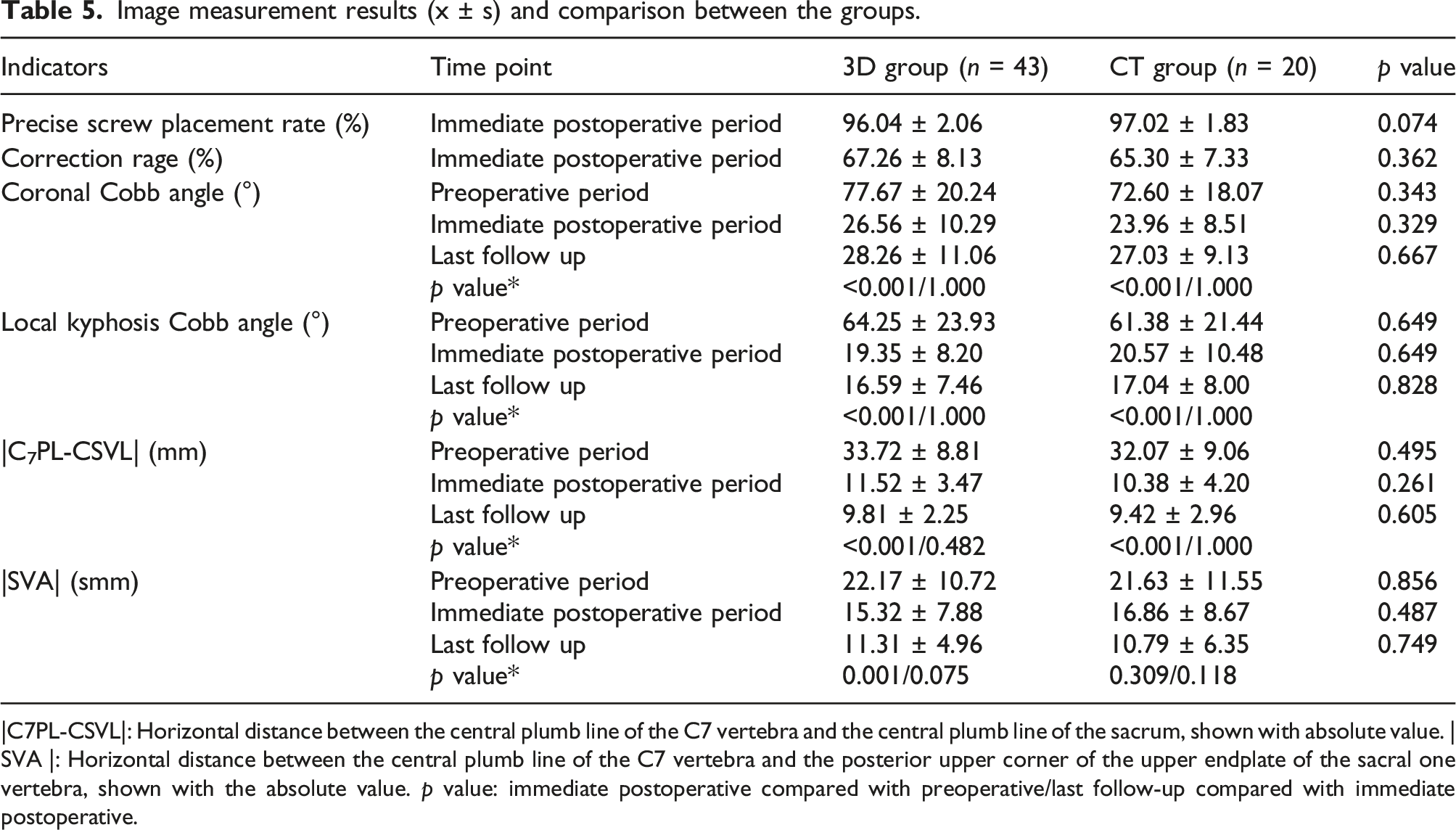
|C7PL-CSVL|: Horizontal distance between the central plumb line of the C7 vertebra and the central plumb line of the sacrum, shown with absolute value. |SVA |: Horizontal distance between the central plumb line of the C7 vertebra and the posterior upper corner of the upper endplate of the sacral one vertebra, shown with the absolute value. p value: immediate postoperative compared with preoperative/last follow-up compared with immediate postoperative.
Discussion
Accurate screw placement using the pedicle screw technique for scoliosis remains difficult, especially in the presence of abnormal pedicle development. In this retrospective study, 3D-printed guide-assisted screw placement was compared with intraoperative CT-guided screw placement. The accuracy of 3D-printed guide-assisted screw placement was slightly lower than that of CT navigation-assisted screw placement, but the difference was not statistically significant. 3D-printed guide-assisted screw placement was effective in reducing the operative time in screw placement.
Clearly, there are some shortcomings of this study. First, this study was a retrospective study, and the selection of surgical methods was inconsistent. Especially in the later period of the study, most patients chose 3D-printed guide plate-assisted screw placement for surgery, resulting in an uneven distribution of cases between the groups in this study. Second, 3D spinal models for patients in the CT navigation group were not created to help surgeons understand the specific conditions of the spinal deformity. Third, the sample size was small, especially for the CT navigation group. Last, in this study, only 3D-printed guide plate-assisted screw placement and CT navigation-assisted screw placement were compared, with no evaluation of techniques such as freehand screw placement, although there have been many similar studies.
A total of 814 pedicle screws were implanted in this group, including 30 screws with grade C, D and E placement, 22 in the 3D group and eight in the CT group. Common features of these poorly positioned screws were the poor development of the pedicle and the thin or severe rotation of the vertebral body, which are the main causes of poorly placed pedicle screws. Another possible reason for the poor position of the screws in the 3D group was that the pedicle screws were not placed in the screw path prepared by the guide plate, which should be confirmed and improved in our future work. Moreover, other reasons for the poor positioning of the screws in the CT group was that only four to six screws could be placed in one CT scan, these screws were preferentially placed in the most deformed areas, and not all the pedicle screws were placed by the CT guide. In addition, the accuracy of screw placement is related to the location of screws. It is generally believed that the accuracy of screw placement in thoracic vertebrae is lower than that in lumbar vertebrae, and inaccurately placed screws are more likely to cause vascular injury.11,12 Other factors include osteoporosis, although this is less common in children. Fortunately, there was no cases of reoperation due to poor screw positioning.
In this study, there were 20 patients who underwent CT navigational screw placement, with 263 screws placed, with an accuracy rate of 97.02%, which was similar to relevant literature reports.13–15 However, in the process of use, we found that CT navigational screw placement has the following deficiencies. First, computer navigation is complex and has a long learning curve, requiring professional assistance and cooperation and good communication between the surgeon and the relevant operators. Second, navigation equipment is relatively expensive and needs to be used in conjunction with intraoperative CT and special surgical beds, which requires a large economic investment and thus a certain economic burden for medical institutions. Third, navigation instruments and intraoperative CT machines occupy a large area, and a large space is needed to facilitate operation, which requires a certain size of the operating room. Fourth, during the intraoperative CT scan, the length of each scan was relatively short, approximately 4-6 segments. If the scan range is large, two or more scans are needed. Fifth, complicated intraoperative navigation operations, CT scanning and data reconstruction take a certain amount of time, thus prolonging the operation time and increasing the risk of bleeding and infection. Sixth, the intraoperative CT scan radiation dose is relatively large, which will cause certain radiation damage to patients and operators, especially paediatric patients, and some scholars have similar views.16,17
3D-printed guide screw placement greatly overcomes the disadvantages of computer-guided screw placement and leads to a high accuracy rate of screw placement. In this group, there were 43 patients who underwent guide plate-assisted screw placement, and 551 screws were placed, with an average screw placement accuracy rate of 96.04%. Ming Luo et al. 18 reported that 244 screws were inserted in 15 patients with lateral curvature with Cobb angles greater than 90° by using 3D-printed guide plate fixation. The accuracy rate was 93%, which was significantly better than that of manual fixation and could shorten the operative time of screw placement. There are two advantages. First, the operation is simple, the learning curve is short, and even less experienced surgeons with proper training can achieve accurate screw placement. Second, the cost is low, and no other auxiliary equipment, such as intraoperative CT and carbon fibre surgical beds, is needed. However, there was an increase in the number of fluoroscopies in the 3D-printing group relative to the navigation group.
This study showed that 3D-printed guide screw placement was effective in reducing screw placement time and saving operative time. The average screw placement time was 83.4 min less than that in the navigation group, and even the 3D-printed guide plate screw placement time was less than half of the time used in the CT navigation group. Although all procedures in this group were performed by one team, this longer time for the CT navigation group may also be related to the long learning curve and lack of proficiency in CT navigation techniques. In a multicentre study including 4588 patients, the duration of surgery was found to be an independent risk factor for postoperative complications in spine surgery. 19 Therefore, a shorter duration of surgery is beneficial in reducing the risk of infection and postoperative complications. The imaging of the patients in this study showed a correction rate of 67.26% ± 8.13% in the 3D-printing group and 65.30% ± 7.33% in the navigation group. The literature reports that the correction rate of scoliosis with posterior surgery alone is generally 40%–70%.20–22 In contrast, Lawrence et al. treated seven children with severe spinal deformities using individualized 3D-printed models and guides and achieved an impressive correction rate of 83%. 23 Patients in both groups were satisfied with the correction of the deformity and achieved the expected results, and we believe the main reason for this is that good pedicle screw positioning provides better holding power and orthopaedic ability. Second, good screw positioning can effectively avoid nerve and vascular damage, and the surgeon can perform deformity correction surgery with more confidence and peace of mind.
The experiences in using guide plate-assisted screw placement are as follows. First, according to the surgeon’s screw placement habit and patient anatomical structure, it is necessary to fully communicate with engineering staff before making the guide plate so that the intraoperative use of the guide plate can be more convenient. Second, a more detailed and complete preoperative design and plan should be created, including osteotomy position, osteotomy mode, spinal shape after osteotomy, the predicted fixation rod shape and the specific type of each screw. In particular, the right screw should be prepared before the surgery to be used directly during the surgery so that the operation time and blood loss can be reduced. Third, appropriate lengthening of the incision, especially the caudal end of the incision, is needed. The blockage of the muscle wall requires appropriate extension of the incision to ensure adequate apposition between the guide plate and the vertebral plate, articular eminence, etc. Fourth, the guide plate and the model should be used in combination. During the intraoperative operation, the guide plate should be compared with the general position on the model and then placed in the body for use so that the position of the guide plate can be better determined. Fifth, Kirschner wire with a diameter of 2.5 mm is generally used during intraoperative operation, while the diameter of the guide hole is designed to be 2.8 mm, which makes the operation easier.
This study has the following limitations. First, this study was a retrospective study, and the sample size of navigation group was small. Second, 3D printing guide plate requires data collection, modeling, design, printing and disinfection, which need time and cost. Third, there was no control group and hand screw.
Conclusion
In this retrospective study, 3D-printed guide plate-assisted screw placement and CT navigation-assisted screw placement can both achieve precise screw placement and proper correction of deformities. In contrast, the 3D-printed guide-assisted screw placement technique has advantages in terms of operation time, screw placement time and intraoperative blood loss, and no special equipment is needed, making it easier for wider application. However, further confirmation is needed in prospective studies.
Footnotes
Author contributions
HLY, XHF, and LC contributed to the study design. XHF and LC contributed to the data analysis and drafted the manuscript. HLY directed data collection and provided administrative support for the project. All authors contributed to interpretation of the data, commented on the manuscript, revised the manuscript, revised the manuscript, and approved the final version for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [Grant number: 81171735], the Provincial Natural Science Foundation of Shaanxi [Grant number: 2017JC2-04] and Air Force Military Medical University.
Ethical statement
Informed consent
Informed consent was obtained from all individual participants and their legal guardians included in the study.
Data Availability Statement
The data are available from the corresponding author upon reasonable request and with permission from the Xijing Hospital, Air Force Military Medical University.