
Abstract
Background:
One of the causes of dissatisfaction following total knee arthroplasty (TKA) is abnormal knee kinematics. A newly designed bi-cruciate stabilized (BCS) TKA system has been developed to produce close-to-normal kinematics because of its anatomic tibiofemoral articular geometry and cam-post mechanism. Although BCS TKA is expected to improve patient satisfaction, no reports have described the appropriate technique or soft tissue handling required to achieve excellent satisfaction with BCS TKA. This study is to identify preoperative and intraoperative predictors of patient satisfaction after BCS TKA.
Methods:
Altogether, we studied 113 knees with primary varus knee osteoarthritis that underwent BCS TKA with a navigation system. Preoperative parameters including Knee Society Score and patient-reported scores [the Knee injury and Osteoarthritis Outcome Score (KOOS)] and intraoperative parameters including coronal, sagittal and axial alignment and joint laxity in each compartment that affected patient satisfaction was evaluated. Satisfaction score was evaluated with use of the 2011 Knee Society Scoring system. The multivariate regression analysis included age and preoperative and intraoperative parameters that correlated with satisfaction scores in the univariate analysis (P < 0.05).
Results:
The mean satisfaction score was 28.2 ± 6.1. Multivariate regression analysis showed that the predictors of patient satisfaction were a preoperative high KOOS score for activities of daily living (P < 0.001), male sex (P = 0.005), older age (P = 0.027), and minimal medial joint laxity during flexion (P = 0.031).
Conclusion:
When performing BCS TKA, surgeons should pay attention to maintaining proper stability of the medial compartment, especially during flexion.
Keywords
Introduction
Total knee arthroplasty (TKA) has been the definitive and best technique for addressing late-stage osteoarthritis (OA) in the knee. With advances in prosthesis technology, prosthetic survival has been gradually extended, with fewer postoperative complications. Nevertheless, about 20% of these patients are reportedly dissatisfied with their surgically restored knees. 1,2
One of the causes for dissatisfaction with TKA is reported to be abnormal knee kinematics, such as a lack of tibial rotation during flexion and paradoxical motion, indicating that there is anterior sliding of the femoral component on the tibia as the knee goes into flexion, largely due to the posterior position of the femur relative to the tibia during full extension. 3
Recently, a newly designed bi-cruciate stabilized (BCS) total knee system [Journey I BCS; Smith & Nephew, Memphis, TN, USA] has been developed to produce close-to-normal kinematics. This procedure substitutes for the lack of cruciate ligaments and menisci by placing a cam-post mechanism and restoring anatomic tibiofemoral articular geometry which includes 3° of the tibial varus angle with an asymmetrical tibial plateau and a medially concave and laterally convex shape relative to the tibial baseplate using 2.5 mm differences in medial and lateral compartment thicknesses. 4,5 However several complications were reported including anterolateral pain from iliotibial band irritation, possibly due to excessive femoral rollback and femorotibial dislocations. Therefore a modified implant called Journey II BCS was developed to prevent complications. The femoral implant design modifications included reducing the mediolateral component width; thinning the edge of the anterolateral flange; and smoothing the intention to degrease soft tissue impingement. The intercondylar box was increased in height to accommodate an enhanced height for the tibial post and also positioned more anterior with respect to the tibial baseplate. 6 This modification has maintained close-to-normal kinematics and led to good clinical and functional short-term results. 7 –9
Some surgeons believe there would be no intersurgeon and intrasurgeon difference, because the implant behaves strictly as a mechanically constraint-guided motion system. However, Victor et al. 4 reported that a surgeon-to-surgeon comparison revealed dissimilarities and the surgical technique handling could have influenced kinematics even in a guided-motion prosthetic design. However, to our knowledge, no previous reports have described an appropriate technique or the soft tissue balance required to achieve satisfaction after BCS TKA. Surgeons should be aware of the factors related to the BCS TKA technique that affect patient satisfaction.
Therefore, the aim of this study was to identify intraoperative predictors of patient satisfaction after BCS TKA. However, not only intraoperative but also preoperative and postoperative factors could be involved. Regarding the postoperative factors, we performed the same postoperative management, including pain control and rehabilitation, in all patients. Hence, the current study assessed preoperative and intraoperative predictors of patient satisfaction following BCS TKA.
Methods
The institutional review board of our hospital approved this study (Number 10462-1). All patients provided written informed consent.
From September 2014 to December 2016, a total of 133 primary knee arthroplasties were performed using the Journey II BCS system. Patients with primary varus OA who underwent knee replacement using the image-free navigation system (Precision N; Stryker Orthopedics, Mahwah, NJ, USA) were included. Exclusion criteria were the following; presence of a valgus deformity (2 knees); navigation system was not used because it had malfunctioned (4 knees); postoperative complications (2 knees: one case of patella clunk syndrome treated with arthroscopic debridement; one infection treated with open debridement and insert exchange); complete data not recorded (12 knees).
Thus a total of 113 knees were evaluated and underwent BCS TKA, none of which required revision. The mean follow-up was 3.1 years (range 2–5 years). The patient population was composed of 91 women and 22 men [mean age 72.9 ± 7.7 years; mean body mass index 26.5 ± 4.3 kg/m2; mean preoperative hip–knee–ankle (HKA) angle 168.8° ± 6.1° (11.2° in varus)].
Preoperative scores were obtained using the Knee Society Score. 10 Preoperative subjective scores were evaluated using the validated version of the Knee Injury and Osteoarthritis Outcome Score (KOOS), a self-reporting questionnaire with 42 items in five separately analyzed subscales of pain; symptoms; activities of daily living (ADL); physical, sports, and recreational function; and knee-related quality of life. Each of the five scores was calculated as the sum of the items included, and the scores were then transformed into a 0- to 100-point scale, with 0 points representing extreme knee problems and 100 points representing no knee problems. 11,12
All procedures were performed by five knee surgeons who used the same surgical technique. A senior surgeon (H.I.) participated in all the procedures either as the chief surgeon or first assistant.
Surgical procedure
A paramedian approach was used for all patients, and the patella was not everted. The distal femur and proximal tibia were cut guided by the navigation system. Femoral alignment was aimed for placement of 90° to the mechanical axis in the frontal plane and 4° of flexion in the sagittal plane. For the tibia, the alignment was aimed at 90° to the mechanical axis in the frontal plane and 3° of the posterior slope in the sagittal plane.
Soft tissue balancing was achieved, and the extension and flexion gaps were measured using a balancer device. The amount of posterior femur resection was adjusted to equalize the extension and flexion gaps in the medial compartment to maintain medial stability.
Femoral rotation was determined to be parallel to the surgical epicondylar axis, allowing residual lateral ligamentous laxity. 13 –15 Tibial rotational alignment was determined using the range of motion (ROM) technique, wherein the knee was put through a full range of flexion and extension, allowing the tibial trial to orientate itself in the best position relative to the femoral component, thereby reducing rotational mismatch of the components. 16
Postoperative rehabilitation
The same rehabilitation protocols were applied in all patients. ROM exercise and walking exercise with a crutch and then a walker were started on the first postoperative day. At 2–3 weeks postoperatively, the patient was discharged from our hospital and completed their rehabilitation protocol with physiotherapists.
Intraoperative gap measurement/ joint laxity
The extension and flexion gaps between the osteotomized surfaces were measured twice by the chief surgeon using a force-controlled, compartment-specific ligament tensioner with a distraction force of 80 N for each compartment. Averages of the measurements were used. The mean joint gaps at extension and flexion were 22.2 ± 1.8 mm and 22.5 ± 2.0 mm, respectively, in the medial compartment and 24.0 ± 2.3 mm and 23.3 ± 2.6 mm, respectively, in the lateral compartment.
For this study, medial and lateral joint “laxity” was defined as the values for the “joint gap minus total thickness of the components (i.e., femoral component, tibial tray, and tibial insert).” The mean joint laxities at extension and flexion were 2.8 ± 1.1 mm and 3.2 ± 1.5 mm, respectively in the medial compartment and 4.7 ± 1.9 mm and 4.0 ± 2.5 mm, respectively, in the lateral compartment.
Postoperative evaluation
Radiographic evaluation
The HKA angle was measured using full-length, standing radiography. Frontal alignment of the femoral and tibial components—frontal femoral component angle (FFC), frontal tibial component angle (FTC)—was measured using full-length radiography. The femoral component sagittal alignment and tibial slope—lateral femoral component angle (LFC), lateral tibial component angle (LTC)—were also measured using lateral radiography. Rotational alignment of the femoral and tibial components was evaluated using computed tomography images. The rotational femoral component angle was defined as the angle between the line of the anterior cutting surface and the surgical epicondylar axis. The rotational tibial component angle was defined as the angle between the line connecting the medial border of the tibial tuberosity with the center of the posterior concavity of the tibial tray and the line passing through the anteroposterior center of the tibial tray. 17,18
The postoperative HKA angle was 179.4° ± 2.1°. The components of 102 patients (90.3%) were mechanically aligned (within 0° ± 3° of the mechanical axis), and those of 11 patients (9.7%) were outside that range. The mean component alignments were as follows: FFC 89.5° ± 1.7°, FTC 89.2° ± 1.4°, LFC 86.0° ± 1.5°, LTC 86.6° ± 1.6°. The rotational femoral component angle was 0.3° ± 1.6° internal rotation, and the rotational tibial component angle was 2.0° ± 4.0° external rotation.
Clinical evaluation
Postoperative scores were evaluated using the Knee Society Knee Score (KSKS), Knee Society Function Score (KSFS), and KOOS at the latest follow-up visit. ROM was also recorded. Satisfaction score was evaluated using the 2011 Knee Society Scoring (KSS) system. 19,20
Statistical analyses
Data were analyzed using the Bell Curve 2016 (SSRI Co., Ltd., Tokyo, Japan) software package for Microsoft Windows, and tests for normality and distribution were performed using the Kolmogorov–Smirnov test. We compared preoperative and postoperative parameters (ROM, KSKS, KSFS, KOOS) using a paired t test. We performed Pearson’s correlation analysis to assess the correlation between preoperative and intraoperative parameters and patient satisfaction and the unpaired t test to compare the patient satisfaction scores between the two groups for qualitative data (female or male, mechanically aligned or not). The relations between the satisfaction score and the preoperative and intraoperative parameters were calculated using a multivariate regression analysis. All significance tests were two-tailed, and a significance level of P < 0.05 was used for all tests.
Results
Preoperative and postoperative ROM, KSKS, KF, and KOOS results are shown in Table 1. All parameters improved significantly after the operation. The postoperative satisfaction score according to the 2011 KSS was 28.6 ± 6.1.
Comparisons of preoperative and postoperative ROM and scores.
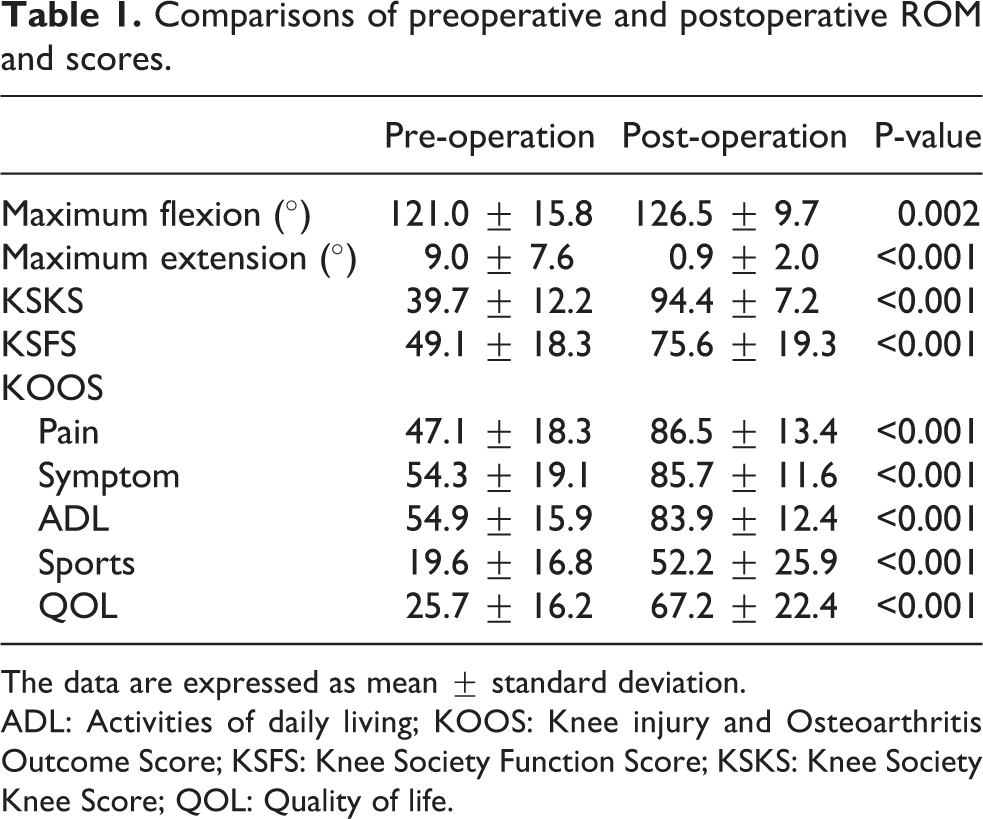
The data are expressed as mean ± standard deviation.
ADL: Activities of daily living; KOOS: Knee injury and Osteoarthritis Outcome Score; KSFS: Knee Society Function Score; KSKS: Knee Society Knee Score; QOL: Quality of life.
Univariate analysis for preoperative factors
Figure 1 shows a positive correlation between patient satisfaction and KOOS ADL (P < 0.001) and symptoms (P = 0.003). The satisfaction score for men was 31.5 ± 8.7, and that for women was 27.4 ± 8.2, with the men achieving a significantly higher satisfaction score (P = 0.044). The preoperative HKA (P = 0.459), body mass index (P = 0.631), extension angle (P = 0.532), flexion angle (P = 0.830), KSKS (P = 0.212), KSFS (P = 0.286), and the KOOS subscales of pain (P = 0.089), sports function (P = 0.337), and quality of life (P = 0.147) showed no correlation with satisfaction.

Correlations between satisfaction score of the 2011 Knee Society Scoring System and preoperative activity of daily living score and symptom score of the Knee injury and Osteoarthritis Outcome Score. Satisfaction score was positively correlated with (A) activity of daily living score (R = 0.39, P < 0.001) and (B) symptom score (R = 0.36, P = 0.003).
Univariate analysis for intraoperative factors
The femoral rotational angle was positively correlated with satisfaction (Figure 2).

Correlation between satisfaction score and femoral rotational angle. Satisfaction was positively correlated with femoral rotational angle (R = 0.29, P = 0.034).
Medial joint laxity during both extension and flexion were negatively correlated (Figure 3). Postoperative HKA (P = 0.443), FFC (P = 0.552), FTC (P = 0.619), LFC (P = 0.376), LTC (P = 0.390), tibial rotational angle (P = 0.802), lateral joint laxity during extension (P = 0.120), and lateral joint laxity during flexion (P = 0.051) showed no significant correlation with satisfaction. The mean satisfaction score for the mechanically aligned group was 28.7 ± 8.6 and that of the outlier group 26.5 ± 8.5. There was no significant difference between the two groups (P = 0.437).
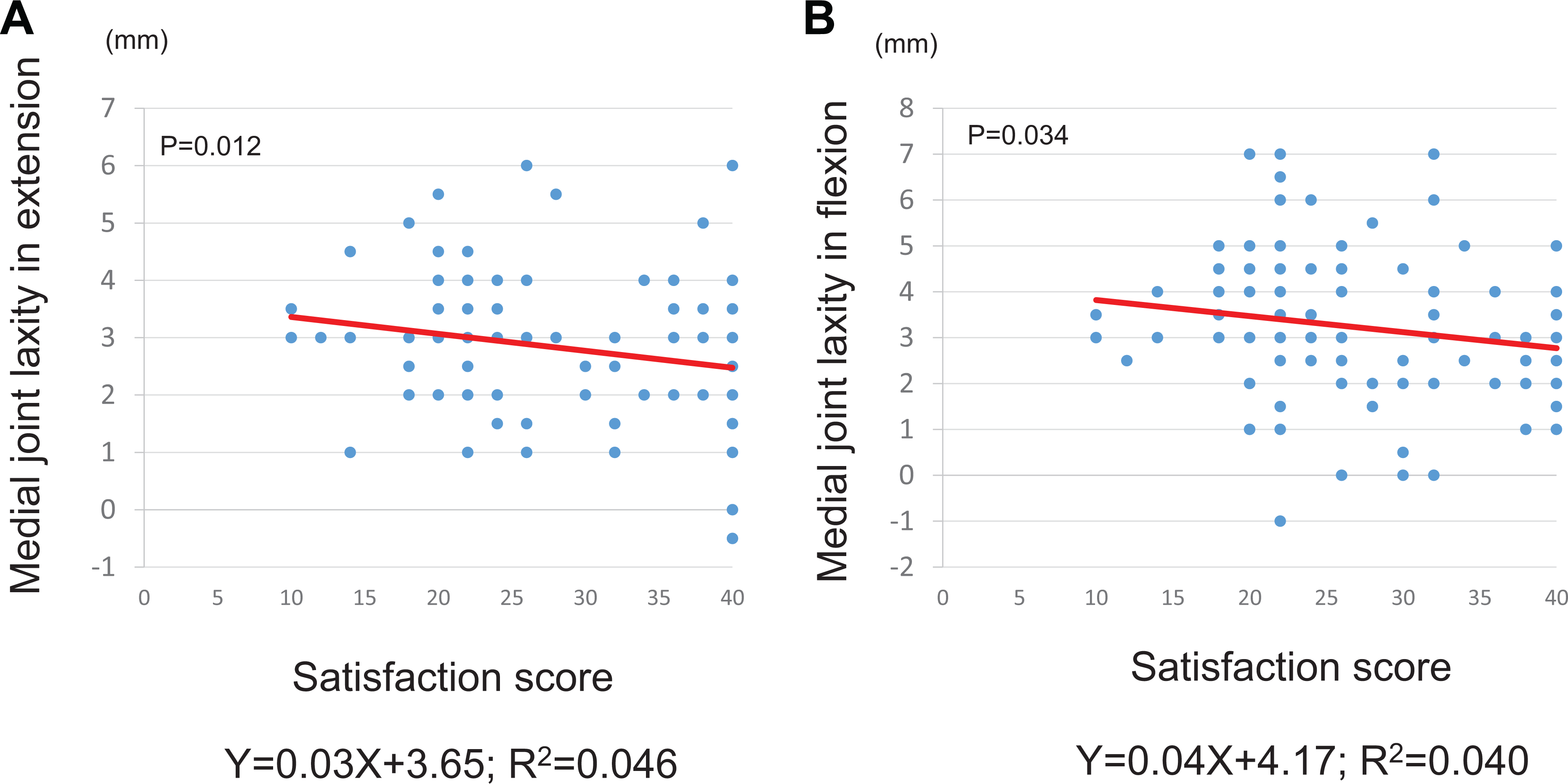
Correlations between satisfaction score and medial joint laxity in extension and in flexion. Satisfaction score was negatively correlated with (A) medial joint laxity in extension (R = −0.21, P = 0.012) and (B) medial joint laxity in extension (R = −0.20, P = 0.034).
Multivariate regression analyses
We conducted multivariate regression analyses to assess the parameters that affected the satisfaction score. We used age and preoperative and intraoperative parameters that had correlated with the satisfaction score (P < 0.05). The KOOS symptoms subscale was excluded because of multicollinearity. Multivariate analysis showed that preoperative higher KOOS ADL (P < 0.001), male sex (P = 0.005), older age (P = 0.027), and less medial joint laxity during flexion (P = 0.031) were predictors of patient satisfaction (Table 2).
Results of multivariable regression analysis.

ADL: Activities of daily living; KOOS: Knee injury and Osteoarthritis Outcome Score.
Discussion
The most important finding of this study was that the intraoperative predictor of patients’ satisfaction after BCS TKA was medial joint stability during flexion. We also found that some preoperative factors—high KOOS ADL, male sex, older age—predicted satisfaction after BCS TKA.
Soft tissue balancing is one of the most important factors for successful TKA, 21 –23 although a poor relation between the intraoperative soft tissue balance and clinical outcomes using physician-derived clinical scores has been reported. 24 Recently, several articles reported the relation between intraoperative soft tissue balance and patient-reported scores. Matsumoto et al. 25 reported that a relatively loose flexion gap improves patient-reported clinical outcomes, including satisfaction with cruciate-retaining TKA. In contrast, Azukizawa et al. 26 reported that intraoperative medial joint laxity during flexion decreases patient satisfaction after cruciate-sacrificed TKA. The current study revealed that medial joint laxity during flexion decreased satisfaction following BCS TKA. Although BCS TKA is reported to alleviate mediolateral instability in flexion range by its prosthesis design, excessive laxity in flexion will not be appropriate for BCS TKA similar to other prostheses designed for TKAs.
Accurate limb alignment is also essential for TKA success. 21 –23,27 It is one of the most commonly accepted principles of TKA that one should aim for mechanical alignment. 27,28 In the current study, the satisfaction scores of the mechanically aligned group and the outlier group were not significantly different. Recently, the importance of mechanical alignment has been questioned, 29 –31 and several studies showed that some mild varus alignment after TKA leads to better results for patients with varus OA. 32,33 In this study, however, we included nine patients with “mild” varus (HKA ≥174° to <177°) whose average satisfaction score was 25.3 ± 7.7, whereas the satisfaction score of the mechanically aligned group was 28.3 ± 8.6. Although the difference was not significant, mechanical alignment should be an appropriate target for successful BCS TKA. Further study is necessary to identify the ideal target for BCS TKA.
With regard to preoperative predictors of satisfaction, there are several previous studies. 34 –36 Kahlenberg et al. 36 listed five factors which was reported by more than one study in their systematic review about patient satisfaction after TKA as follows: (1) higher baseline patient-reported function, (2) better mental health, (3) severe degenerative change, (4) older age, and (5) male gender. Among four factors except for mental health which we didn’t assessed in the current study, three factors (baseline patient-reported function, age, gender) applied to the current study while one factors (severity of OA) didn’t apply. In other words, the BCS prosthesis might be the first choice for patients with severe knee pain whose degenerative OA changes on radiography were not sufficiently severe to achieve high satisfaction of the patients.
The mean KSS 2011 score indicating satisfaction following BCS TKA was 28.6 ± 6.1. Patient satisfaction after TKA is reported to differ by race. 34 Several reports from Asia assessed patient satisfaction using KSS 2011. The reported satisfaction scores of other TKA designs (posterior stabilized, cruciate retaining, cruciate sacrificing) ranged from 21 to 26. 25,26,37 –42 BCS TKA might be recommended for surgeons because just maintaining medial stability in flexion proved to be enough to achieve excellent patient satisfaction. However, to know whether BCS TKA is truly superior to other TKA designs, we must compare the satisfaction scores between BCS and other designs of TKAs in patients with similar demographics.
There are several limitations. First, this was retrospective study with a relatively small number of patients. In particular the total number of male patients are only 22. Second, the follow-up period was relatively short. Third, we did not assess the patients’ preoperative mental health, which has been reported to influence patient satisfaction. 34,35,36 Fourth, joint laxity in the current study was calculated using the osteotomy gap, not the component gap. Matsui et al. 43 reported that there was no significant difference between the component gap width at 90° flexion and the osteotomy gap width at 90° flexion. Therefore, evaluation of the joint laxity in flexion, which was proved to be one of the predictors of patient satisfaction after BCS TKA in the current study, is appropriate. Nevertheless, the osteotomy and component gaps during extension are reportedly different because the posterior femoral condyle of the component tightens the posterior capsule, resulting in a smaller joint gap during full extension. 44 These differences might affect our results that medial joint stability during flexion was one of the predictors of patient satisfaction while the medial stability during extension wasn’t.
Conclusions
Preoperative and intraoperative predictors of patient satisfaction after BCS TKA were the preoperative high KOOS ADL score, male sex, older age, and medial joint stability during flexion. When performing BCS TKA, surgeons should pay attention to ensure appropriate soft tissue balance of the medial compartment especially during flexion.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.