
Abstract
Aims:
In unicompartmental knee arthroplasty (UKA), tibial components must be correctly sized and positioned so that tibial cut surfaces are well covered without marked under- or overhang with impingement of the surrounding soft tissue. We used morphometric data of both medial and lateral tibial plateaus separately to plan UKA and evaluated the compatibility of the measurement data to the dimensions of six currently available tibial prostheses in a Japanese population.
Materials and Methods:
Using computed tomography, we preoperatively examined 60 patients (30 medial and 30 lateral osteoarthritis (OA)) scheduled for primary UKA at our hospital between 2013 and 2017. Each tibial cutting surface was measured in the transverse plane at 2 mm below the respective joint line. We used anteroposterior and mediolateral length to calculate the mediolateral length/anteroposterior ratio of both medial and lateral compartments. We then compared measurements across six current UKA systems: Oxford fixed tibia and fixed lateral tibia, Triathlon, TRIBRID, JOURNEY UNI, and HLS Uni Evolution.
Results:
We found no significant differences in morphometric data between the medial and the lateral OA. The cutting surface of lateral plateau, however, had smaller anteroposterior dimensions, greater mediolateral length, and higher mediolateral length/anteroposterior ratio than those of medial plateau. Therefore, in this Japanese population-based study, Oxford lateral tibia had good compatibility with the measurement data of lateral compartments.
Conclusions:
Lateral compartments had lower anteroposterior length, greater mediolateral length, and higher mediolateral length/anteroposterior ratio than those of medial compartments. We, therefore, strongly recommend using Oxford fixed lateral tibia for lateral OA over other current tibial prostheses because of superior coverage.
Introduction
In unicompartmental knee arthroplasty (UKA), tibial components must be sized and positioned properly so that the tibial cut surfaces are well covered without marked under- or overhang, followed by subsequent impingement of the surrounding soft tissue. 1
Figure 1 shows typical postoperative obvious mediolateral underhang by X-ray after lateral UKA using the Oxford fixed tibia (FTO; Zimmer Biomet, Warsaw, Indiana, USA). This was expected because conventional tibial prostheses, including the FTO, are designed to fit the medial compartment due to low incidence of isolated lateral osteoarthritis (OA) compared with medial OA.

Two weeks postoperative AP and ML X-ray of typical ML underhanging case 3 months after UKA using Oxford fixed tibia. (a) Obvious ML underhanging of tibial prosthesis is observed in AP X-ray. (b) Although AP dimension is well fitting according to ML X-ray. AP: anteroposterior; ML: mediolateral; UKA: unicompartmental knee arthroplasty.
Various adverse effects of tibial component mismatch have been reported. 2,3 Edge loading on the tibial polyethylene and insufficient bony support of the tibial component 2 led to a lower Oxford Knee Score (OKS) and pain score. 3,4 Therefore, a crucial issue regarding achieving proper coverage UKA is avoiding mismatch of the tibial component and proximal tibial cut surface. Various morphological studies of the proximal tibia have been conducted to provide data for proper matching in total knee arthroplasty (TKA). 5 –12 Computer simulation studies revealed morphological differences due to sex and race as well as asymmetry between the medial and the lateral condyle. 5,8,10,12,13 Servien et al. 14 also reported differences between the medial and the lateral plateaus in a Western population. Currently, there are no reports evaluating those of an Asian population and any differences in the necessary components between the medial and the lateral OA. Although asymmetric tibial components have been available in some TKA implants, same-shaped implants have been used for UKA.
Clinical outcomes of lateral UKA have been comparatively unsuccessful next to those of medial UKA. 15 –17 However, it has been reported that careful selection of patients and appropriate use of the prosthesis can result in definite pain relief and better long-term durability of prostheses in lateral UKA. 18 –20
In general, fixed-type prostheses are preferred in lateral UKA because they have been proved to have higher survival rates than mobile-type prostheses. Due to dislocation of the bearing, mobile-type prostheses are associated with higher early failure rates. 15,16,21,22 However, almost all fixed-type prostheses designed to fit the medial compartment do not fit the lateral compartment. 20 The Oxford fixed lateral tibia (FLO; Zimmer Biomet), on the other hand, has different proportions to other current tibial components; they are made exclusively for lateral compartments and are expected to give good coverage of the lateral condyle.
This study aims to separately investigate the dimensions of both medial and lateral tibial plateau planning of UKA. Moreover, it evaluates the compatibility of lateral compartment measurement data to the dimensions of current tibial prostheses in a Japanese population.
Materials and methods
This retrospective study protocol was approved by our hospital ethics committee. All patients provided informed consent for inclusion in this study. We reviewed computed tomography (CT) data obtained during routine preoperative planning from 60 lower limbs in 60 Japanese patients (10 males and 50 females). The mean body mass index of all patients was 23.1 ± 3.9 kg/m2 (range 17.2–34.2 kg/m2). Patients were scheduled for consecutive primary lateral and medial UKA in our hospital between 2013 and 2017. There were 30 lateral UKAs between 2013 and 2017, and 30 medial UKAs between 2016 and 2017 for isolated OA.
Image technique
CT scans were performed using a 64-row multi-slice CT system in our hospital. Patients were positioned on the CT table in a supine position. Scans of 1.25-mm slices were performed from the hip joint to the ankle joint with the patient in a knee-extended position with the patella facing upward. The obtained image data sets were imported into 3D software (Aquarius Net; Tera Recon, San Mateo, California, USA). The operating window of the software comprises three multiplanar reformation views of the frontal, sagittal, and axial planes. Each reconstructed image can be simultaneously rotated, cut, and measured arbitrarily in all three operating windows.
Three investigators performed all radiographic assessments and operated the software to measure the angles and lengths on a virtual cut surface of the proximal tibia.
Morphometric measurements of the tibial cut surface
The tibial mechanical axis (TMA) was defined as passing through the knee center and the center of the talar dome. The tibial AP axis was defined according to Akagi’s line, which connects the attachment of the middle of the posterior cruciate ligament (PCL) and the medial border of the patellar tendon (PT) to the tibial tubercle. 23 The tibia was raised along the TMA and moved along the tibial AP line in an anterior direction. The proximal tibial articular surface was cut perpendicularly to the mechanical axis of the tibia with a posterior inclination of 7° and 2 mm below the respective joint lines. We used the tibia AP line as the anteroposterior axis of the proximal tibia. Then, lateral anteroposterior (lAP) and medial anteroposterior (mAP) lines were drawn parallel to the tibia AP line through both tip of medial and lateral intercondylar eminences. We also evaluated the anteroposterior (AP) and mediolateral (ML) length and calculated the ML/AP ratio of both medial and lateral compartments (Figure 2).
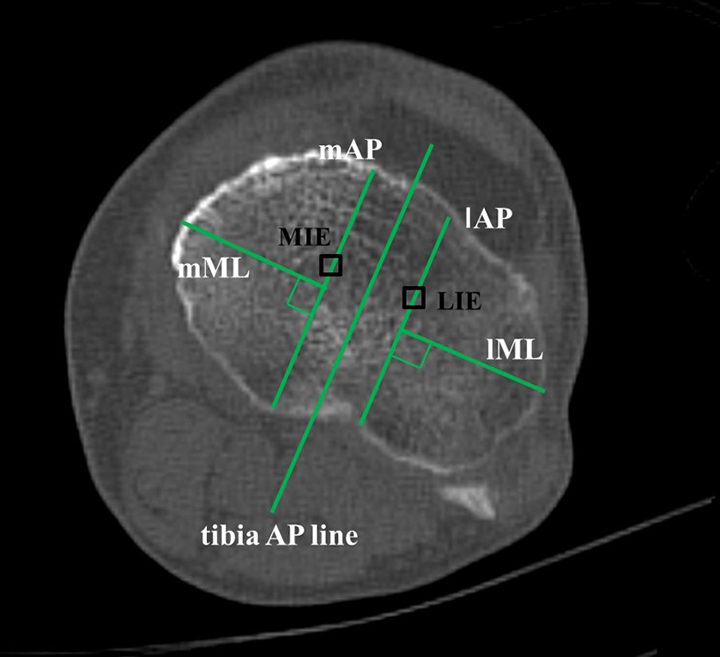
Method of morphometric measurement. Tibia AP line, drawn from the center of the posterior cruciate ligament tibial insertion to the medial border of the patellar tendon, was used as the anteroposterior axis of the proximal tibia. The lAP and mAP lines were drawn parallel to tibia AP line through MIE and LIE. The lML and mML lines were drawn perpendicular to each AP line. AP: anteroposterior; lAP: lateral anteroposterior; mAP: medial anteroposterior; MIE: medial intercondylar eminence; LIE: lateral intercondylar eminence; lML: lateral mediolateral; mML: medial mediolateral.
Finally, we estimated the morphometric data of six current tibial prosthetic systems: FTO and FLO (Zimmer Biomet), Triathlon (Stryker, Kalamazoo, Michigan, USA), TRIBRID (KYOCERA Medical Corporation, Osaka, Japan), JOURNEY UNI (Smith and Nephew, Memphis, Tennessee, USA), and HLS Uni Evolution (Corin, Cirencester, UK). Oxford distributes have two fixed-type prostheses. One of the fixed type is bilateral use (FTO) and another (FLO) is for the lateral compartment only. We simulated the sizing using the data of six tibial components, assuming that an under- and overhang of up to 3 mm could be allowed. A previous study reported that medial overhang of the tibial component of 3 mm or more can significantly worsen the OKS and pain score. 3 We chose the optimal implant size based on the AP length and examined the proportion of cases either underhanging or overhanging more than 3 mm in the lateral compartments.
Statistical analysis
All values are presented as mean ± standard deviation (SD). Results were analyzed using a statistical software package (StatView 5.0, Abacus Concepts Inc., Berkeley, California, USA).
Using paired t-test (p < 0.05), we evaluated the differences of AP length and ML length and ML/AP ratios between the medial and the lateral compartment in two groups (the medial OA group and the lateral OA group). The differences of ML/AP ratios of both the medial and the lateral compartment between two groups were also evaluated using unpaired t-test (p < 0.05).
Post hoc power analysis was performed using G*Power 3. 24 For a sample size of 30 versus 30 elements in two groups and a type I error (α) of 0.05 (unpaired t-test), the study is expected to provide a power (1 − β) of 0.92 for detecting an effect size of 0.8.
Results
Measured morphometric data are summarized in Table 1.
Morphometric data of tibia plateau in each group (medial OA and lateral OA).

AP: anteroposterior; ML: mediolateral; OA: osteoarthritis; N.S: not significant.
Morphometric data of medial compartments in two groups (medial OA and lateral OA)
Average mAP dimensions were 47.9 ± 3.0 mm (range 40.9–59.0 mm) and 46.9 ± 3.1 mm (range 43.3–53.5 mm) for medial OA and lateral OA, respectively.
Average mML dimensions were 26.7 ± 3.2 mm (range 22.5–38.4 mm) and 24.9 ± 1.3 mm (range 22.7–26.5 mm) for medial OA and lateral OA, respectively.
Average ML/AP ratio of medial compartment was 0.554 ± 0.06 (range 0.45–0.73) and 0.528 ± 0.06 (range 0.48–0.59) for medial OA and lateral OA, respectively.
None of the parameters (AP length, ML length, and ML/AP ratio) had significant differences between the medial OA and the lateral OA.
Morphometric data of lateral compartment in three groups (medial OA and lateral OA)
Average lAP dimensions were 46.2 ± 3.4 mm (range 39.8–57.4 mm) and 45.1 ± 2.7 mm (range 39.9–50.3 mm) for medial OA and lateral OA, respectively.
Average lML dimensions were 33.1 ± 3.9 mm (range 27.3–43.4 mm) and 30.9 ± 2.3 mm (range 26.8–33.9 mm) for medial OA and lateral OA, respectively.
Average ML/AP ratio of lateral compartments was 0.711 ± 0.08 (range 0.60–0.93) and 0.679 ± 0.05 (range 0.61–0.74) for medial OA and lateral OA, respectively.
None of the parameters (AP length, ML length, and ML/AP ratio) had significant differences between the medial OA and the lateral OA groups.
Comparison of morphometric data between medial and lateral compartments in medial OA and lateral OA groups
The lateral compartment had shorter AP length and longer ML length than the medial plateau in each group (p < 0.05).
The ML/AP ratio was greater for the lateral plateau than for the medial plateau in each group (p < 0.05).
Morphometric data of six tibial prostheses available in Japan
AP and ML dimensions and the aspect ratios (AP/ML) of each prosthesis are summarized in Table 2.
Sizes and ML/AP ratios of tibial components available in Japan.

OFT: Oxford fixed tibia; OFL: Oxford fixed lateral tibia; AP: anteroposterior; ML: mediolateral.
Some tibial implants (FTO, Triathlon, and TRIBRID) had an aspect ratio closer to that of the medial tibial plateau, while FLO was closer to the lateral plateau.
Proportion of cases underhanging or overhanging more than 3 mm in lateral OA groups
In the lateral OA group, the proportion of cases under- or overhanging more than 3 mm were 83.3% for FTO, 0% for FLO, 90% for Triathlon, 96.7% for TRIBRID, 80% for JOURNEY UNI, and 43.3% for HLS uni evolution (Table 3).
Proportion of cases under- or overhanging more than 3 mm in the lateral OA group.

FTO: Oxford fixed tibia; FLO: Oxford fixed lateral tibia.
Discussion
In this study, the shape of the lateral tibial plateau differed from that of the medial plateau in medial and lateral OA. Morphometric measurement data of the proximal tibia of an Asian population had good compatibility with the Oxford lateral tibia (FLO). To the best of our knowledge, this is the first study to describe the morphometric measurements of the proximal tibia, the medial and lateral compartments separately, and how these data can be adapted for choice of Oxford partial knees in an Asian population.
In the present study, we found a significant difference in the morphometric parameters between the medial and the lateral compartment for the two groups. These results suggest that the shape of the lateral tibial plateau differs from that of the medial plateau in the lower AP dimension, greater ML dimension, and higher ML/AP ratio, which is similar to the previously reported findings. 14 Although it was recently reported that the asymmetric tibia plate had better total tibial coverage compared to the symmetric tibia plate in TKA, 25 no tibial prostheses were adapted to the shape of the lateral compartment in UKA. Therefore, if we use conventional bilateral prostheses for the lateral compartment, ML underhang will inevitably occur.
Although we encountered typical postoperative mediolateral overhang by X-ray images after lateral UKA using FTO, we found no cases of under- or overhanging of more than 3 mm, in contrast to higher rate of other tibial prostheses in coverage simulation. These results suggest that FLO, therefore, is beneficial for achieving better coverage in lateral OA.
Additionally, there were no significant differences in morphometric data between the medial and the lateral OA. The results also suggest that proportions of medial and lateral condyle are similar between the medial OA and the lateral OA, respectively. This also implies that the compartment being affected by OA or not does not effect on the shape of tibia, despite the possibility of changing proportion due to degeneration. This shows the functionality of lateral UKA using FLO as an alternative method of TKA in both primary isolated lateral OA and lateral progression of arthritis following medial UKA, previously reported as the most common reason for revision surgery. 26
We studied only Japanese patients undergoing UKA. This is the major limitation because the shape of the tibia might be different in other populations. A second limitation is that the rotation of tibia cut surface may change depending on the rotation, and these effects should also be investigated in future studies. Thirdly, our study only evaluated in the case of resection less than 2 mm below the joint line. Indeed, the tibial bone cutting level may change depending on various factors such as proximal tibial morphology, the amount of bone erosion, and surgical procedures. Additionally, the level of the tibia cut can affect the surface area and bone coverage. Therefore, the assessment of coverage at various tibial cutting levels should be considered in the near future. Finally, although current results suggest that using FLO for lateral OA may improve coverage, future long-term studies are needed to verify good coverage leading to better clinical outcomes and superior long-term survival.
In conclusion, these results are important reference data for designing proper UKA tibial components specifically for a Japanese population. The proximal tibial cut surface was asymmetric. Lateral compartment has lower AP length, greater ML length, and higher ML/AP ratio than those in medial compartment. We therefore strongly recommend using Oxford fixed lateral tibia for lateral OA over other current tibial prostheses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.