
Abstract
Aims
This study aims to evaluate the long-term durability of a unicompartmental knee arthroplasty (UKA) implant using a fixed-bearing all-polyethylene tibial tray with a Cobalt-Chromium (Co-Cr) femoral condyle, stratified by patient age. It also aims to compare implant survivorship between inlay and onlay tibial implantation techniques.
Methods
Data from the New Zealand Joint Registry (NZJR) was used to evaluate survival of Smith & Nephew Genesis II® UKA performed between February 2000 and December 2011 in which two different tibial implant techniques (inlay and onlay) were used. The primary endpoint was revision surgery.
Results
At a minimum follow-up of 10 years, 57 revisions were performed at an average of 6.6 years from index surgery. The revision rate per 100 component years was 1.29 (CI: 0.97 – 1.66), with a significant difference between the over-75 years cohort compared with the under-65 cohort, in favour of the older cohort (p < 0.05). There was a significant difference in survival between inlay and onlay techniques, in favour of the inlay technique (p < 0.05).
Conclusion
Fixed-bearing all-polyethylene tibial UKA show acceptable outcomes at an average 12-year follow-up, especially in elderly patients and use of inlay tibial tray implantation technique.
Introduction
Unicompartmental knee arthroplasty (UKA) remains a valuable treatment option for knee arthritis despite the widespread success of total knee arthroplasty (TKA). Registry data suggest that UKA accounts for approximately 10% of knee arthroplasty procedures globally.1,2 Controversy persists in the literature regarding decision-making in patient selection for UKA, including indications, prostheses and outcomes.1,3–5 Proponents of UKA cite lower peri-operative morbidity, faster post-operative recovery, superior range of motion, better functional outcomes and preservation of bone stock.3,6–10
The all-polyethylene tibial component has declined in global use due to concerns of early failure and limited perceived benefits over alternatives.11,12 Nevertheless, its advantages of reduced cost, bone preservation and elimination of backside wear, remain relevant, particularly in select patient populations such as the elderly or resource-constrained settings.11,13–15 There is a paucity of long-term outcome data specific to all-polyethylene UKA in large cohorts.14,16
An underexplored aspect is the impact of tibial tray preparation technique, inlay versus onlay, on implant survivorship. Although biomechanical studies suggest differential stress distributions, the clinical significance of this in all-polyethylene implants is poorly defined.11,12,16
The aim of this study was to address this knowledge gap by evaluating long-term outcomes of an UKA prosthesis with a fixed-bearing, all-polyethylene tibial tray articulating with a Co-Cr femoral runner related to age at index surgery and tibial tray implantation technique (inlay vs onlay).
Methods
The New Zealand Joint Registry (NZJR), with a capture rate of over 95%, was used to identify all Genesis II® (Smith and Nephew) UKA over the active lifetime of this implant in New Zealand between 2000 and 2011. 17 This implant was introduced into the New Zealand market in 2000 following withdrawal of the Mod III (Marmor) prosthesis and supplanted by a different implant in 2012. Follow-up data were analysed in 2025 to assess survivorship beyond 10 years. The NZJR has National ethical approval granted in 1998, with informed consent obtained from individuals undergoing arthroplasty procedures for collection and use of their data in research.
Demographic data and tibial tray implantation technique were collected. Inlay components were recessed into a carved pocket on the tibial surface and therefore relied more on subchondral bone, whereas onlay components were cemented on top of the flat tibial cut and therefore relied on cortical and subchondral bone (Figure 1). Interval to and reasons for revision surgery were analysed. Age at index operation was stratified into four bands (<55 years, 55–64 years, 65–75 years, ≥75 years) for sub-group analysis of implant survival. Inlay (a) and onlay (b) tibial implantation techniques.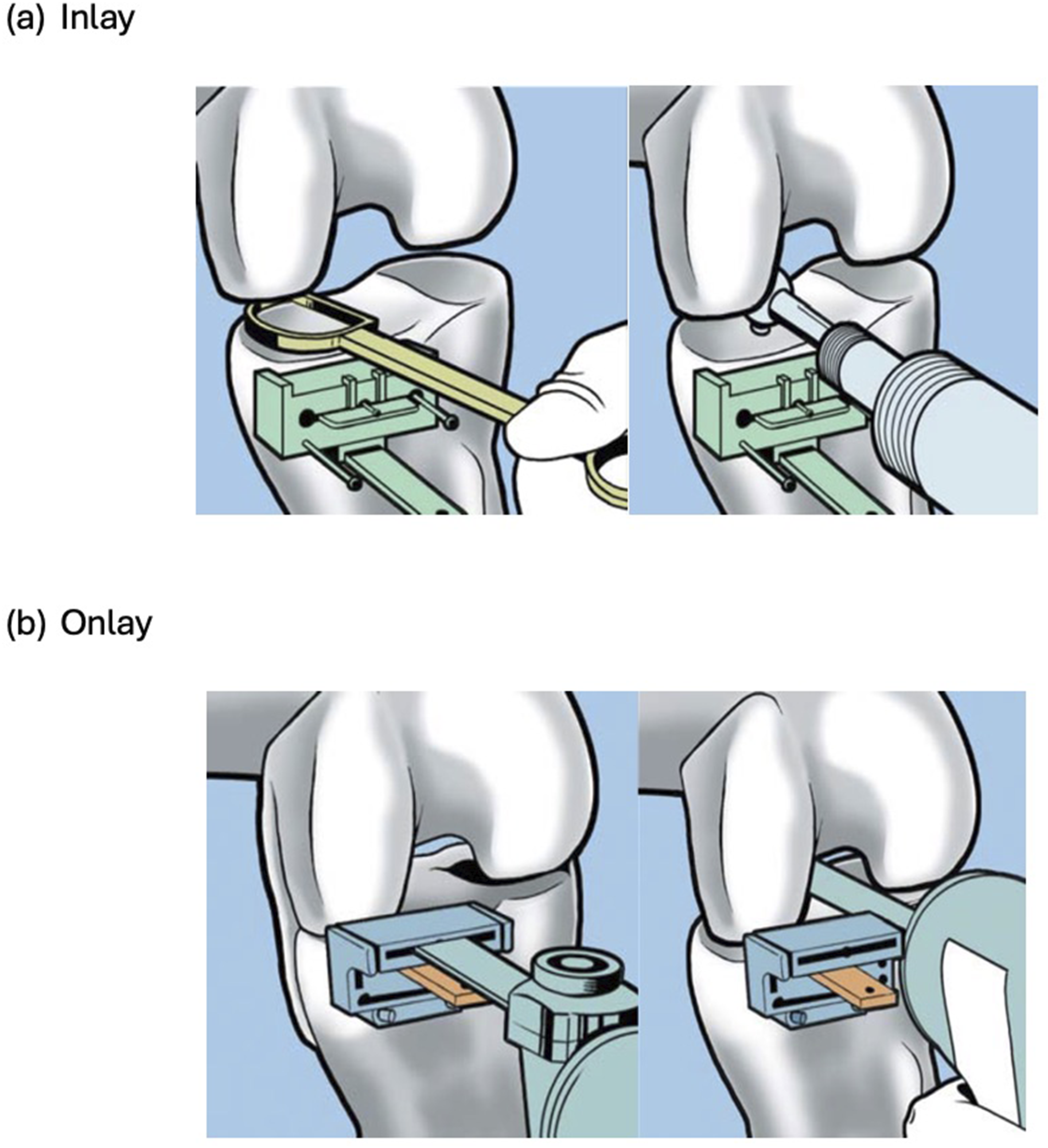
Statistical analysis was performed using SPSS (IBM, USA). Comparisons between groups were performed using chi-square or Fisher’s exact tests, ANOVA and Kaplan-Meier survivorship analysis with log-rank tests. Cox proportional hazards regression was used to estimate the hazards ratio and 95% confidence interval comparing inlay and onlay groups. A p-value of 0.05 or less was considered statistically significant.
Revision rates in the NZJR were provided in the form of rate per 100 component years (RR/100CY). This was derived by dividing the number of implants revised by the observed component years, multiplied by 100. This allowed consideration of the number of years of post-operative follow-up in calculation of the revision rate. Implant survival was censored by mortality.
Results
Study demographics.

Revision rates between inlay and onlay cohorts.

Implant survivorship by age and tibial preparation technique.

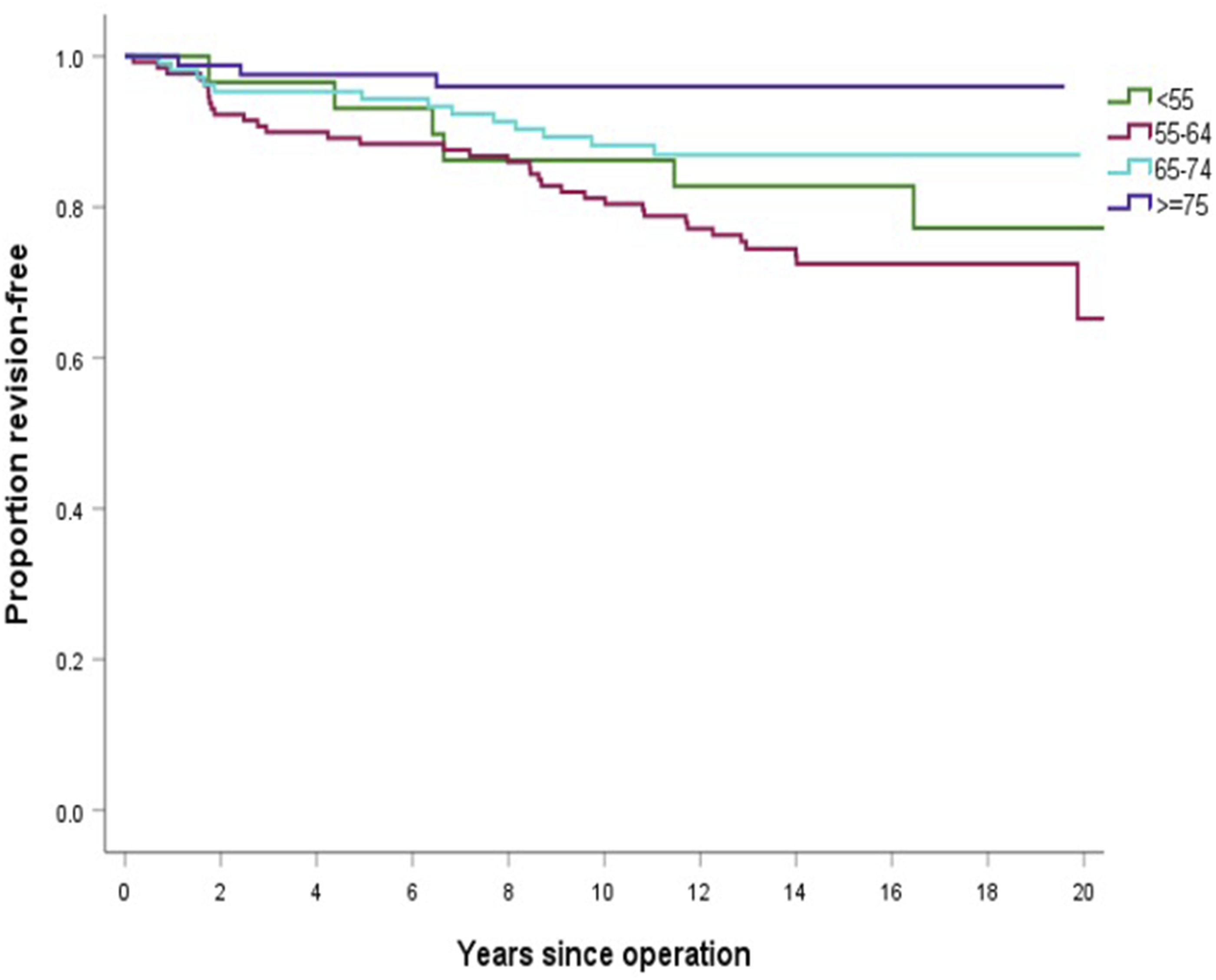
Cumulative Kaplan-Meier survivorship for 350 smith & nephew genesis II unicompartmental knee replacements stratified by age.
Revision rate per 100 component years for inlay and onlay cohorts.

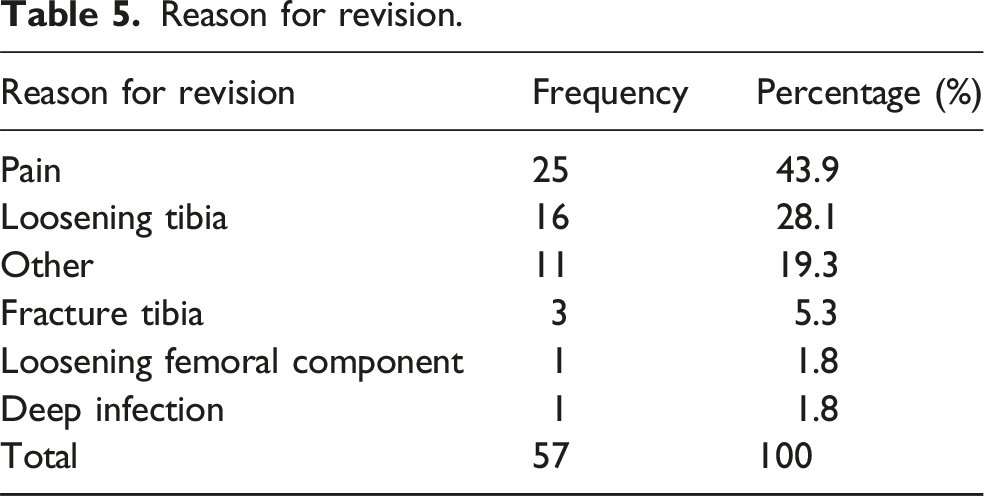
Reason for revision.
Discussion
UKA remains a well-established and effective procedure in appropriately selected individuals with isolated end-stage compartmental knee arthritis. Compared to TKA, UKA is associated with preservation of cruciate ligaments and unaffected compartments, shorter operative time, reduced blood loss, higher patient reported outcome scores and lower risk of serious medical complications including venous thromboembolic phenomena.6–10 Despite these advantages, concerns persist regarding UKA survival relative to TKA, as well as unresolved debates surrounding different UKA design concepts such as fixed versus mobile tibial bearings, metal-backed versus all-polyethylene tibial components and inlay versus onlay implantation of all-polyethylene tibial trays.1,3,5
UKA survivorship and age
The revision rate in our cohort (1.29 per 100 component years) was higher than that of TKA in the NZJR (0.44 per 100 component years), consistent with prior reports showing UKA carries up to a four-fold increased revision risk compared to TKA.2,18–23 Although UKA has a higher revision rate, conversion to TKA is generally technically less demanding than revision TKA, which may lower the surgical threshold for UKA revision. Outcomes after UKA to TKA revision remain mixed, with age at index surgery being a critical factor influencing survivorship.22,24–27
A 15-years prospective randomized controlled trial by Newman et al. demonstrated superior survival in UKA compared to TKA in individuals over 65 years 28 Conversely, Pearse et al. found poorer outcomes in individuals under 65 undergoing revision UKA to TKA. 22 These findings align with recommendations by the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) UKA Manual, which supports UKA as a cost-effective and safe option for elderly patients. 15
In our study, individuals aged 75 years and older had 15-years survivorship of 96%, consistent with literature reporting excellent outcomes in older cohorts (Table 3 and Figure 2). For instance, Bruce et al. reported a 10-years survivorship of 92.4% in individuals over 70, while NZJR data show highest UKA survival (94.8% at 10 years) in the 81–85 age group, with a progressive decline thereafter.14,20
While these data support the durability of UKA in older populations, they must be interpreted with caution. The apparent survivorship advantage may be partly attributed to selection bias, as elderly patients typically have lower functional demands and higher competing mortality risks. These factors can reduce the likelihood of revision, thereby inflating survivorship estimates independent of implant performance.
UKA revision indications
In prior studies, aseptic loosening and osteoarthritis progression were the most common failure modes for UKA.29,30 In contrast, our registry-based study identified “pain” as the leading reason for revision (43.9%), with osteoarthritis progression contributing less frequently (Table 5). This pattern is consistent with registry data reporting revision for pain in 48.8% of UKA cases and a higher incidence of unexplained pain after UKA compared to TKA (23% vs 9%, p < 0.001).21,22
However, the prominence of pain as a revision indication represents a critical limitation when interpreting registry-based outcomes. Pain is inherently subjective and susceptible to variability in clinical interpretation, reporting thresholds, and coding practices. Chen et al. recently highlighted inaccuracies in the reporting of NZJR revision data, noting over-reporting of unexplained pain and under-reporting of objective causes for revision such as progression of osteoarthritis. 31 These findings indicate that registry-reported revision indications may not reliably reflect true implant failure modes.
Accordingly, the high proportion of revisions attributed to pain in our study should be interpreted cautiously. Rather than indicating a mechanical failure mechanism, this likely reflects limitations in data collection and reporting compliance. This underscores the need for improved standardisation and validation of revision coding in arthroplasty registries to enhance the accuracy of outcome assessments and clinical interpretability of registry-derived outcomes.
Inlay versus onlay tibial implantation
Tibial component loosening is a growing cause of UKA failure.28,30,32,33 Biomechanical studies suggest that inlay and onlay preparations affect stress distribution at the bone-implant interface. With an inlay preparation, a recess is created within the tibial plateau allowing the implant to fit into the prepared bone defect, which preserves bone around the outer edge of the tibia and captures the tibial tray. In comparison, an onlay preparation involves bone resection across the top of the tibial plateau of the affected compartment, typically for placement of a metal-backed plastic bearing, which is in theory, to be supported by the underlying cortical bone. 12 Walker et al. undertook finite element analysis based on computed tomography scans and found that inlay designs produce significantly higher peak stress and strain at the tibial surface compared to onlay components. 12
Despite theoretical concerns of the influence of implant material on adaptive bone remodeling of the proximal tibia, clinical comparisons between inlay and onlay preparation techniques in all-polyethylene tibial components remain limited. In a Level III systematic review, Costa et al. found no significant difference between all-polyethylene and metal-backed designs. 11 Similarly, Lee et al. reported equivalent outcomes between metal-backed and all-polyethylene tibial components in a fixed-bearing UKA over 10 years 13 All-polyethylene fixed-bearing tibial designs reduce revision risk due to bearing dislocation, backside wear observed in metal-backed tibial trays and depending on tibial preparation technique, may preserve bone stock by reducing bone cut from the tibia. Polyethylene wear has less frequently been cited as a cause of failure after UKA. 16
We found a significantly lower revision rate in the inlay group (0.90 vs 1.61 per 100 component years; p = 0.023), suggesting tibial preparation technique may influence implant longevity (Table 4). This may reflect better cortical rim preservation with inlay preparation, promoting enhanced fixation whilst preserving bone stock. Additionally, time to revision was shorter in the onlay group (5.7 years vs 8.3 years).
While inlay preparation demonstrated superior survivorship, it is important to note that surgeon experience and compartment involvement differed between groups. Inlay procedures were more commonly primarily performed by consultants, whereas onlay procedures had greater involvement by a trainee under direct consultant supervision. Furthermore, lateral UKA was more frequent in the onlay group. Both factors – seniority of primary surgeon and compartment involved – may independently influence revision risk and should be considered as potential confounders.
Previous studies evaluating inlay and onlay techniques in isolation have shown good long-term outcomes, but few directly compare the two techniques.14,16 To our knowledge, this is the first national registry-based study to evaluate inlay versus onlay tibial preparation technique for all-polyethylene UKA in a real-world cohort.
Limitations
Our findings must be interpreted with caution and are applicable only to fixed-bearing all-polyethylene tibial component UKA designs similar to the design evaluated in this study. The authors acknowledge the limitations of a retrospective registry study design. Inlay procedures were more often primarily performed by consultants and lateral UKA procedures, which may partially explain the observed differences in revision rates. Unmeasured confounders including BMI, radiographic progression, surgeon volume and nuances related to surgical technique were not available and may further contribute to unmeasured confounding. Nonetheless, this is the first study to compare inlay and onlay all-polyethylene tibial UKA using long-term registry data.
Conclusion
UKA with a fixed bearing all-polyethylene tibial component demonstrates favorable long-term survivorship in individuals over 75 years old. Inlay tibial preparation was associated with a signficiantly lower revision risk compared to onlay, potentially due to improved cortical rim preservation and fixation stability.
These findings support the use of all-polyethylene inlay UKA in carefully selected elderly patients with good bone quality and lower activity demands. Results should be interpreted with consideration of registry limitations and potential confounders.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.