
Abstract
Background
Despite the established advantages of partial knee replacements (PKR), their usage remains limited. We investigated the effect of hospital knee arthroplasty (KA) volume and the availability of a frequently used PKR by the total KA supplier on the use of PKRs in a hospital.
Methods
A total of 190,204 total knee replacements (TKR) and 18,134 PKRs were identified in the Dutch Arthroplasty Register (LROI) from 2007 to 2016. For each hospital we determined the annual absolute KA volume (TKR+PKR) into quartiles (<103, 103–197, 197–292, >292 knee replacements/year), and determined whether the TKR supplier provided a frequently used PKR. Hospitals were divided in routine PKR users (≥13 PKRs/year) or occasional/non PKR users (<13 PKRs/year). Based on these parameters, the effect of total KA volume and supplier on PKR usage was investigated, using chi-square tests. Logistic regression analysis was performed to evaluate the influence of the combination of these factors.
Results
In the lowest volume group, around 15% of the hospitals used PKRs, compared to 75% in the highest volume group. Having a TKR supplier that also provides a frequently used PKR resulted in a higher likelihood of performing PKR, especially in low volume hospitals.
Conclusions
Hospitals’ total KA volume and the availability of a frequently used PKR appear to influence the use of PKR.
Introduction
Medial partial knee replacement (PKR) is a successful surgical procedure for end-stage anteromedial osteoarthritis.1–4 Described advantages of a PKR over a total knee replacement (TKR) are lower mortality, less complications, better postoperative clinical outcome and lower costs of surgery.5,6 Nevertheless, the PKR has been a topic of debate due to the diversity in reported long-term survival rates in registry data. Sufficient surgeon and hospital volume, and the use of appropriate indication criteria for primary PKR are essential to obtain optimal results.7–11 Given the described advantages and the known components for successful procedures, a widespread implementation could be expected. However, registers indicate that the actual proportion of PKR in KA patients is still 10–15%,12–15 while probably around 50% of the patients is eligible for PKR.9,11 Factors that influence this discrepancy remain unclear. Possibly, surgeons are still worried about the survival rates of PKRs. Another reason could be that they knowledge about the indications to be used for medial PKR. If the traditional indications described by Kozinn and Scott are used, only 2.2– 4.3% of the patients with knee osteoarthritis are considered eligible for medial PKR. 16 According to Goodfellow et al. applying their more recent and broader indications result in a potential PKR candidate pool of almost 50%. 17 Gaining more knowledge about the right indication for PKR could raise the proportion of PKRs used in KA patients and thereby the hospital proportional volume of PKR.
Barriers and facilitators may play a role in the implementation. Surgeon experience and knowledge, evidence of its performance, support with training and implementation from the supplier, and also patient demand may influence the surgeon’s decision for a PKR or a TKR. In large volume hospitals, optimal settings can be created more easily in specialized units and PKR implementation would be facilitated. On the other hand, if the TKR supplier does not supply a frequently used PKR, the choice for PKR implementation may be less likely. This study investigated potential factors that influence PKR usage. Specifically, we evaluated whether the volume of the KA population in a hospital was associated with usage of PKRs. Also, we examined whether the availability of a frequently used PKR within the product range of the hospital’s TKR supplier was associated with the actual use of PKRs.
Materials and methods
Study population
Data were extracted for all primary PKR and TKR procedures between January 2007 and December 2016. Data were extracted from the Dutch Arthroplasty Register (LROI: Landelijke Registratie Orthopedische Implantaten), which contains data about orthopedic joint implants in the Netherlands since 2007. The completeness of the LROI database is more than 99% for primary KA with a coverage of all hospitals in the Netherlands. 13 This study was a retrospective analysis of prospective registry data. All the available PKRs and TKRs in the registry were included. A total of 98 hospitals (university medical centers, general hospitals, and independent treatment centers) were included, with available data for 10 years, resulting in 980 unique cases. Our primary outcome was the effect of hospital volume on the usage of PKRs. Second, the effect of the availability of a frequently used PKR within the product range of the hospital’s TKR supplier on the actual use of PKRs was analyzed (Figure 1).
Data analysis
Data were transformed so that every row in the analysis file consisted of one hospital in a single year. The nationwide PKR usage were analyzed using descriptive statistics. An overview is given of the hospital volumes over the years and the number of hospitals using a (frequently used) PKR.
For every year, hospitals were divided in PKR routine users (≥13 PKRs/year) or occasional/non PKR users (<13 PKRs/year). A cut-off point of 13 was used because Baker and colleagues investigated the effect of hospital volume on risk of revision and recommended to undertake at least 13 PKRs to achieve good results. Badawy et al. did the same kind of study, but we decided to use 13 as cut-off point for routine users, because Badawy described a lower cut-off point of 11.7,8 Subsequently, for each hospital the absolute KA volume (TKR+PKR) was determined per year. The KA volumes were divided into 4 groups based on the quartiles for absolute KA (<103, 103–197, 197–292, >292 knee replacements/year). Finally, it was examined whether the main TKR supplier of each hospital per year could also supply a frequently used PKR (yes/no). For this, a list of frequently used PKRs was generated based on the NJR, SKAR, AOANJRR and LROI per year. When a particular PKR was used in more than 5% of the PKRs in that year the PKR and the accompanying manufacturer were classified as “TKR supplier with a frequently used PKR” for that specific year. This data was joined to our dataset based on the main TKR supplier.
Statistics
Chi-square tests were performed to investigate the effect of KA volume on the use of PKRs, and to investigate whether the availability of a frequently used PKR by the total KA supplier influenced the use of PKRs in a hospital. When both chi-square tests were significant, the interaction effect between the KA volume and the availability of a frequently used PKR on the use of PKRs was examined using logistic regression. When there was an interaction between the KA volume and the availability of a frequently used PKR, we analyzed the data stratified according to the availability or no availability of a frequently used PKR. We analyzed the effect of KA volume (divided into 4 groups based on the quartiles) on the usage of PKRs. P-values <0.05 were considered significant. The statistical package SPSS (version 25, IBM Corp, Armonk, NY, USA) was used for all statistical analyses.
Results
A total of 190,204 TKRs and 18,134 PKRs were registered in the study period (January 2007 and December 2016). A total of 98 hospitals over a study period of 10 years were included, resulting in 980 unique cases. KA volume of these hospitals is increasing over time in the Netherlands, with also a large relative increase for PKR (Figure 2). The number of hospitals that use PKR in the Netherlands increased from 19% to around 50% between 2007 and 2009, and remained more or less the same up to 2016. The number of hospitals that had a supplier with a frequently used PKR fluctuated over the years from 40% in 2007 up to 61–93% in the period 2012–2016 (Table 1). Flowchart of study methods. Hospital volumes, PKR use and availability of frequently used PKR from 2007 to 2016.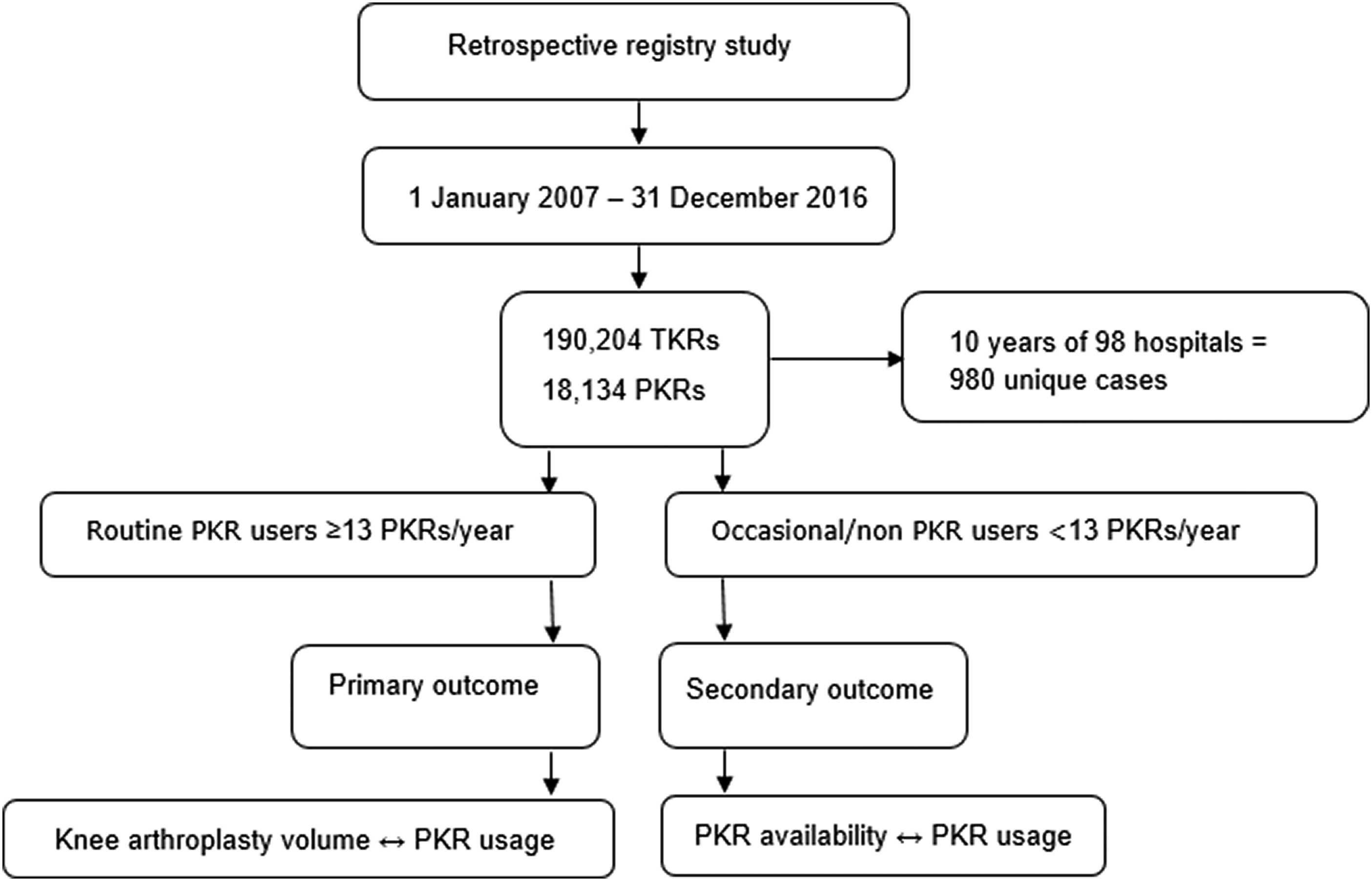

The use of PKRs was significantly different between the KA volume groups (p < 0.001). In the lowest volume group (<103 knee replacements/year) around 15% of the hospitals used PKRs in comparison to around 75% in the highest volume group (>272 knee replacements/year) (Figure 3). Change in KA volumes in the Netherlands from 2007 to 2016.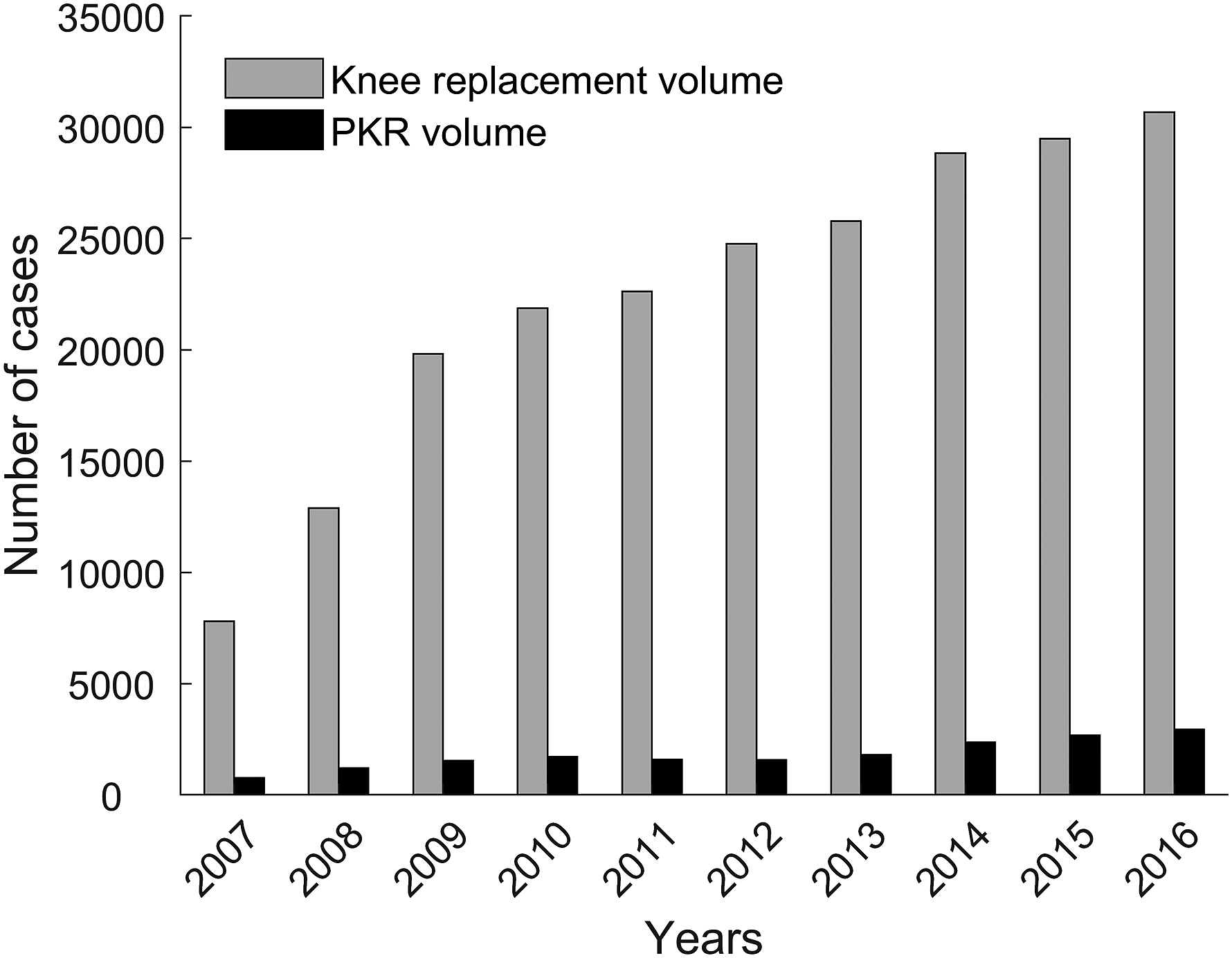
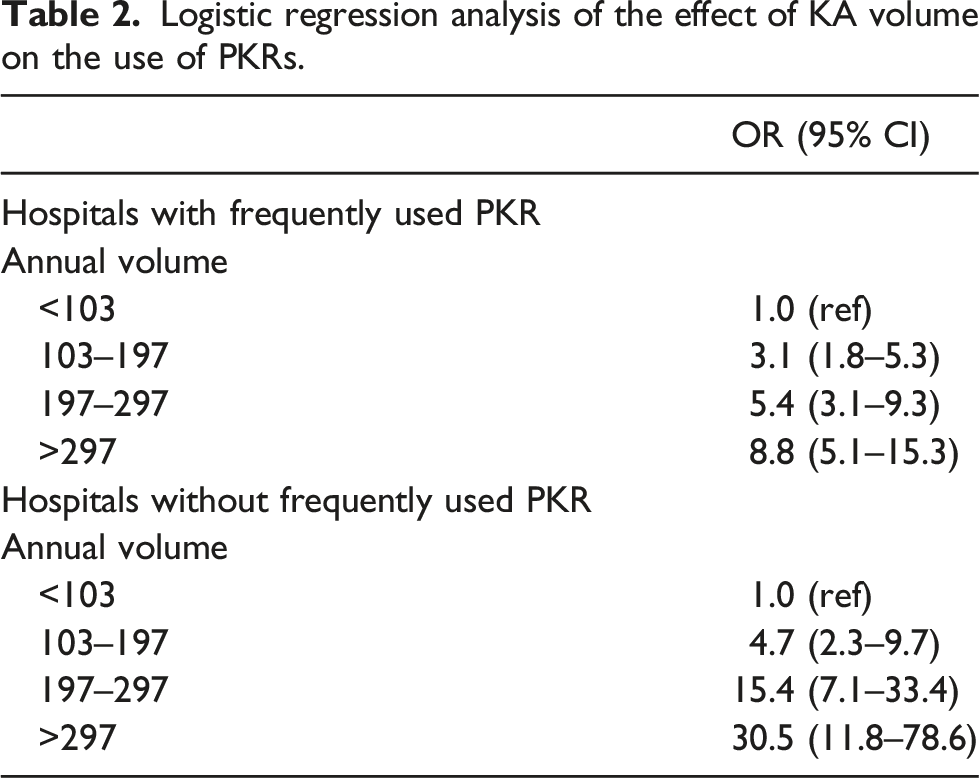
Logistic regression analysis of the effect of KA volume on the use of PKRs.

Effect of KA volume on the actual use of PKR, divided by hospitals with and without a frequently used PKR.
In the group with a TKR supplier without a frequently used PKR, the effect of KA volume on the use of PKRs was even higher than in the hospitals with a frequently used PKR (Table 2, Figures 3 and 4). In the lowest volume group, we found a two times higher odds of using PKRs in the hospitals with a TKR supplier also offering a frequently used PKR (Figure 3). With increasing KA volume, hospitals worked more often with a supplier with a frequently used PKR (p < 0.001) (Figure 5). mean absolute PKR volume used in the different knee volume groups divided by hospitals with and without a frequently used PKR.
Discussion
In this Dutch arthroplasty register study, 98 hospitals that performed a total of 190,204 TKRs and 18,134 PKRs were analyzed between 2007 and 2016. To our knowledge, this was the first study that investigated whether the total KA volume of a hospital influences the actual use of PKRs, and in addition to create awareness about the possible effect of having a TKR supplier with or without a frequently used PKR. Availability of a frequently used PKR differs among the KA volume groups. *Hospitals shown for each year separately (980 cases in total).
The main finding was that hospitals with higher KA hospital volume were more likely to use PKRs. This effect was stronger in the group with TKR suppliers without a frequently used PKR in their product range. Moreover, the smallest volume hospital group showed a two times higher odds of using PKR in the hospitals with a TKR supplier also offering a frequently used PKR. These findings could indicate a larger influence of KA suppliers on the implementation of PKR in low volume hospitals.
The effect of KA volume and the availability of a frequently used PKR on the actual PKR use described in this study has not been reported earlier. Many studies report on the effect of PKR volume on outcome, especially with regard to the survival,7,9,10,18,19 but never on the effect of volume on the actual use and certainly not in combination with the supplier. Previous studies showed a better survival in hospitals with a higher absolute or proportional PKR volume. This may be in line with our results that generally, high volume hospitals more often use PKRs, knowing that a sufficient absolute as well as proportional surgeon volume is needed in order to achieve good results.7–10,18 These better results in higher volume hospitals are also seen in hospitals with a higher TKR volume, however not in survival rate but more in length of stay and length of uninterrupted institutional care. The absence of the effect of volume on survival in TKR may be caused by the overall higher absolute volume in TKR. 20
However, there may also be other explanations for this result. The supplier of knee implants may enable the use of PKR and can also assist in education to create more specialized and dedicated teams. This will lead to an increase in number of hospitals using PKR but not necessary to more PKR usage within the hospital, which is needed to achieve optimal PKR results.7–10,18 This demands an intrinsic motivation by the surgeon and the hospital to adopt the complete PKR philosophy with applying the strict inclusion criteria for this procedure and achieving sufficient volume. The discrepancy of an even stronger increase in PKR use in larger volume hospitals with a supplier without a frequently used PKR implant in their product range as found in this study, may especially reflect this intrinsic motivation. These hospitals frequently have contracted a second supplier for their PKR procedures, indicating an internal motivation to perform PKR and resulting in higher PKR use in this study. The inter-supplier competition may also enhance PKR usage. This is reflected by the finding that the highest volume group without a frequently used PKR supplier performs more than twice as many PKRs than the hospitals with a supplier with a frequently used PKR.
In contrast, a remarkable finding in the smallest volume group (<103 knee arthroplasties/year) was that the percentage of hospitals using PKRs was twice as high in the group with a TKR supplier that also provides a frequently used PKR. Low absolute volume hospitals have a higher risk of revision for PKRs. This was shown with LROI data of the same patient group, 10 but also in register data of the Norwegian Arthroplasty Register, Nordic Arthroplasty Register Association and National Joint Registry for England and Wales.7,18,19 A study of Liddle et al. showed also that proportional volume must be high to get a good result on the survival of PKRs. 9 Therefore, our finding that PKR usage is twice as high in low volume knee replacement hospitals when a frequently used PKR is provided by the TKR supplier might be cause for concern. Combining the evidence on absolute and proportional volume on the risk of revision in PKRs and the fact that around 50% of the patients is eligible for a PKR, it seems justified to perform PKR in hospitals with KA populations of 50–100 patients or larger. 11 Thereby taking into account that each individual surgeon should perform at least 10–13 PKRs per year.7,8 In this study, we found an association between performing PKR (yes/no) and the availability of a frequently used PKR in the product range of the hospital’s TKR supplier. Although we cannot draw conclusions on a possible correlation based on our results, it is possible that the TKR supplier can lower the threshold to start performing PKRs. This was also seen in the group of hospitals performing 103–197 knee arthroplasties/year. In this study, we did not investigate whether the individual surgeons in these centers performed at least 10–13 PKRs annually, but more importantly, it would be hard to achieve the advised number of PKRs annually for each individual surgeon, keeping in mind that the mean proportional PKR volume in the Netherlands over the last years is 10%. Thus, strict in-hospital referral would be required to achieve 10–13 PKRs per year per surgeon. A recent review of Kugler et al. investigating the association of hospital volume-outcome in TKR, proposed a centralization of TKR to high volume hospitals, so a between hospital referral could be another option to consider. 21
The finding that the availability of a frequently used PKR seems more important in hospitals with a low KA volume should create some awareness. In frequently used hospitals patients are more likely to be offered a PKR as a treatment option compared to low volume hospitals. Mainly in low volume knee replacement hospitals, the presence or absence of exposure to PKR by the TKR suppliers, appears to influence PKR usage. This may reflect the intrinsic motivation of the surgeons in high volume centers to perform PKR as a part of their specific expertise regardless of the availability, whereas in low volume centers “easy access” may lower the threshold for PKR usage but does not necessarily lead to adaptation to the PKR philosophy by the general orthopedic surgeon. We recommend that orthopedic surgeons to be aware of this effect and evaluate whether sufficient PKR numbers can be achieved to ensure good results, keeping in mind that around 50% of their KA population is eligible for a PKR.9,11 In addition, in-hospital referral may help in achieving the desired PKR surgeon volume needed to have good results.
The most important limitation of the present study is that, although we showed an association between PKR availability by the TKR supplier and PKR usage, our data do not allow further analysis into a possible causal relationship. Another limitation was that treatment options may be more extensive in specialized units. The extent of specialization of a KA unit cannot be derived from an arthroplasty register. Therefore, hospital volume was used as a proxy for the presence of specialized units. Although in general this may be valid, it may be possible that smaller hospitals do have specialized units and perform PKRs in sufficient numbers.
Conclusions
In conclusion, data from the Dutch Arthroplasty Register showed that hospitals with high absolute KA volumes were most likely to perform PKR. This volume effect was even stronger in hospitals with a TKR supplier without a frequently used PKR. With this result, we want to create awareness about the possible effect of having a TKR supplier with or without a frequently used PKR.
Footnotes
Author contributions
IK: study design, data analysis, and drafting of manuscript. KK: study design, data analysis, and revision of manuscript. AH and SB: revision of manuscript. LS: data acquisition, statistics, and revision of manuscript. RG: interpretation of data and revision of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
As the study was based on registry data, ethical approval was not needed.
Consent for publication
The data used in this study is anonymous, so consent was not needed.
Data availability
The data that support the findings of this study are available from LROI/Dutch Arthroplasty Register, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of LROI/Dutch Arthroplasty Register.