
Abstract
Purpose
The purpose of this study was to investigate clinical efficacy of posterior tibial artery perforator technique combined with iliac crest autograft in treatment of medial soft tissue and medial malleolus loss.
Methods
This study involved 11 cases of medial soft tissue and medial malleolus loss from October 2011 to March 2016. Patients were treated with posterior tibial artery perforator technique combined with iliac crest autograft, and given routine treatment, such as rehydration, anti-inflammation, anticoagulation and vasodilation. Ankle function of patients was evaluated according to the American Orthopedic foot and ankle Association (AOFAS) ankle-hind foot scoring system.
Results
All flaps survived without bone exposure, and the appearance of skin flaps was satisfactory. There was one case of arterial crisis, one case of venous crisis, one case of skin edge necrosis and one case of incision infection. Wounds of the above patients were healed. Skin flap was soft and elastic without secondary contracture. The two-point discrimination of skin flap was 5–11 mm. The ankle range of motion was 10–60°. X-Ray showed that grafts healed within 8.6 months. According to AOFAS evaluation, four cases were excellent, four cases were good, and three cases were poor. The excellent and good rate was 72.8%.
Conclusions
In this study, posterior tibial artery perforator technique combined with iliac crest autograft was used to treat medial soft tissue and medial malleolus loss. The findings demonstrated that this treatment was reliable and efficacious.
Keywords
Introduction
The ankle joint, as a kind of heavy-duty joint, bears a huge load in walking, standing and jumping activities. 1,2 Therefore, the ankle joint has high mechanical requirements for mechanical properties.1,2 Medial malleolus loss often involves bone, skin, tendon, ligament and other defects.3,4 Therefore, surgical treatment is complex and injury is difficult to repair.
In recent years, the development of flap technology and imaging technology provides possible conditions for restoration and reconstruction of ankle function.5,6 Medial soft tissue and medial malleolus loss is rare and difficult to treat clinically.7,8 From October 2011 to March 2016, a total of 11 patients with medial soft tissue and medial malleolus loss were treated with posterior tibial artery perforator technique combined with iliac crest autograft, demonstrating satisfactory clinical outcomes. However, cadaveric allografts of appropriate size are often used in large progressive hospitals in some countries. Therefore, patients with medial soft tissue and medial malleolus loss were treated with posterior tibial artery perforator technique combined with iliac crest autograft in this study.
Patients and Methods
Patients
This study involved 11 cases of medial soft tissue and medial malleolus loss in our hospital from October 2011 to March 2016. All patients received posterior tibial artery perforator technique combined with iliac crest autograft, demonstrating satisfactory outcomes. Among these 11 patients, there were 7 males and 4 females, with an average age of 37.5 years (ranging from 19 to 57 years). The average time from injury to treatment was 5.5 h (ranging from 1.5 to 10.5 h). There were 3 cases of machine twist injury, 3 cases of tamp injury, 2 cases of cutting injury, 1 case of explosion injury and 2 cases of crush injury.
Inclusive and exclusive criteria
Inclusion criteria: ① The defect of medial weight-bearing articular surface of medial malleolus combined with distal tibia was less than 1/3. ② Compound tissue defect with peripheral soft tissue defect. ③ There were no brain, chest or abdominal organ injuries. ④ Patients underwent cardiac color Doppler ultrasound, biochemistry determination and coagulation function evaluation. ⑤ Patient was able to tolerate the operation.
Exclusion criteria: ① Patients with a pathological fracture. ② Patients with primary or secondary coagulation dysfunction.
Therapeutic strategy
In the first (Ⅰ) stage of emergency, a series of processes were conducted, including debridement and suture for the ankle joint, exploration and repair (such as nerves, tendons and blood vessels), and vacuum sealing drainage (VSD) negative pressure wound treatment. After VSD resection (5–7 days post the operation), the wound was treated with antibiotics. When the wound state improved (clean wound) and there was no obvious evidence of infection or inflammation, the bone defect area was measured according to CT images of patients' foot and ankle. Then a tissue transplantation, repair and reconstruction plan was formulated. If there were no operative contraindications, such as coagulation dysfunction or active bleeding, the ankle joint skin defect was repaired with posterior tibial artery perforator flap in the second (Ⅱ) stage. The ipsilateral iliac bone was transplanted for internal fixation and bandaged with sterile dressing. Meanwhile, six mini screws (with the diameter from 2 mm to 3 mm, according to the size of fragments) were used for each autologous graft fixation in this study. Moreover, plaster was used to splint the limb during recovery.
Postoperative management
After the operation, patients were given routine treatments, such as rehydration, anti-inflammation, anticoagulation and vasodilation. The flow and pressure of VSD were closely observed and timely adjusted. 9 Low molecular dextran was intravenously dripped (500 mL) once a day for 7 days. Low molecular weight heparin was subcutaneously injected (5000 U) 1–2 times a day for 5 days. Papaverine was intramuscularly injected (30 mg) once every 6 h, and reduced one time every 3 days, until 12 days after the operation. Patients were exposed to a local baking lamp (25°C, 40 cm away from the affected limb). Five coagulation indexes, D-dimer and biochemical indexes of patients were monitored. The changes of vital signs and blood circulation (swelling degree, skin flap temperature, flap color and capillary filling time) were observed. If the biochemical indexes, coagulation factors and effective perfusion pressure were changed, ECG monitoring should be carried out. Patients were also treated with high permeability drugs (mannitol) and hemofiltration technology.
Clinical evaluation
Ankle function was evaluated using the American Orthopedic Foot and Ankle Society (AOFAS) ankle-hindfoot scoring system. 10 AOFAS scoring system includes a maximum of 100 points. AOFAS scoring system is divided into 4 types of outcomes, including >91 points (excellent outcome), 75–90 points (good outcome), 50–75 (fair outcome) and <50 points (poor outcome).
Results
General postoperative findings
All skin flaps survived without bone exposure, and the appearance of skin flaps was satisfactory to the treating surgeons. According to the condition of the donor regions, the wounds healed and the range of the knee joint motion was not affected. Due to the condition of the recipient regions, one patient developed skin flap artery crisis 12 h post the operation, and was diagnosed as anastomotic vascular thromboembolism via ultrasound. The vascular thromboembolism was treated with a Fogarty balloon catheter, as described by a previous study. 11 About 3 h later, the arterial crisis was corrected and the red-white reaction of the skin flap was good. One patient developed venous crisis on the second day post the operation and was diagnosed as anastomotic vasospasm via ultrasound. The suture and congestion were removed and drainage strip was placed. The 2% lidocaine injection and papaverine injection were locally injected around the skin flap. At the same time, patients were administrated with continuous wet compress with thermo-physiological sodium chloride solution. About 6 h post treatment, the venous crisis was corrected and color of the flap was normal. One patient developed skin flap vascular crisis on the third day after the operation and received symptomatic treatment. The size of the skin flap area was about 2 cm × 2 cm. When the blood supply of flap was stable and the necrotic boundary was clear, free skin grafting was carried out, with well survived skin graft. One case of incision infection was treated with surgical debridement, intra-articular irrigation and VSD. After the above 37 days of treatments, the wound healed. The remaining skin flaps survived and the incision healed in the first stage. The average wound healing time was 13.7 days (ranging from 11 to 19 days).
Follow up
Patients were followed up for 14 months (ranging from 5 to 24 months). The follow-up showed that the skin flap was soft and elastic without secondary contracture. The two-point discrimination of skin flap was 5–11 mm. Six weeks post the operation, the patients began non-weight bearing functional exercise of the ankle joint.
Three months post the operation, the patients underwent partial weight-bearing exercise. Then, the patients underwent X-ray examination of the anteroposterior and lateral position of the ankle every 2–3 months. The X-ray findings showed that the average healing time of the grafts was 8.6 months (ranging from 6 to 13 months). At the last follow-up, the blood supply of limbs was good, and the appearance, sensation and swelling degree were improved. While, the skin flap demonstrated good blood supply and stable ankle joint. The ankle joint had different degrees of extension and flexion function, and the range of extension and flexion activity was 10°–60°.
According to the AOFAS evaluation standard of foot and ankle function, 4 cases were excellent (36.4%), 4 cases were good (36.4%), 3 cases were poor (27.2%), with the excellent and good rate of 72.8%.
Skin flap repair of typical case
A 26 years old female patient developed partial bone and soft tissue defects of the right medial malleolus after a traffic accident. A series of treating processes, including debridement and suture, nerve tendon vascular exploration and repair, VSD coverage, were conducted. The patient’s wound was seriously contaminated. VSD was replaced twice after the operation, and sterile dressing was strictly changed (Figure 1(a)). After the wound condition was improved, it was confirmed that the wound was clean and without obvious evidence of infection or inflammation (Figure 1(b)). About 37 days after the operation, the skin defect of the right ankle was repaired with the nutrient flap of medial malleolus perforator of the posterior tibial artery under epidural anesthesia. The ipsilateral leg skin was separated and the free skin graft was conducted (Figure 2(a)). The ipsilateral iliac bone was separated and fixed with a free iliac bone graft (Figure 2(b)). General images for damaged limb. (a). General image post stage I debridement. (b). Preoperative skin defect, bone defect, perforator site. The ipsilateral leg skin (a) was separated for free skin autograft and ipsilateral iliac bone (b was separated and fixed for free iliac bone autograft.

X-Ray characteristics of typical case
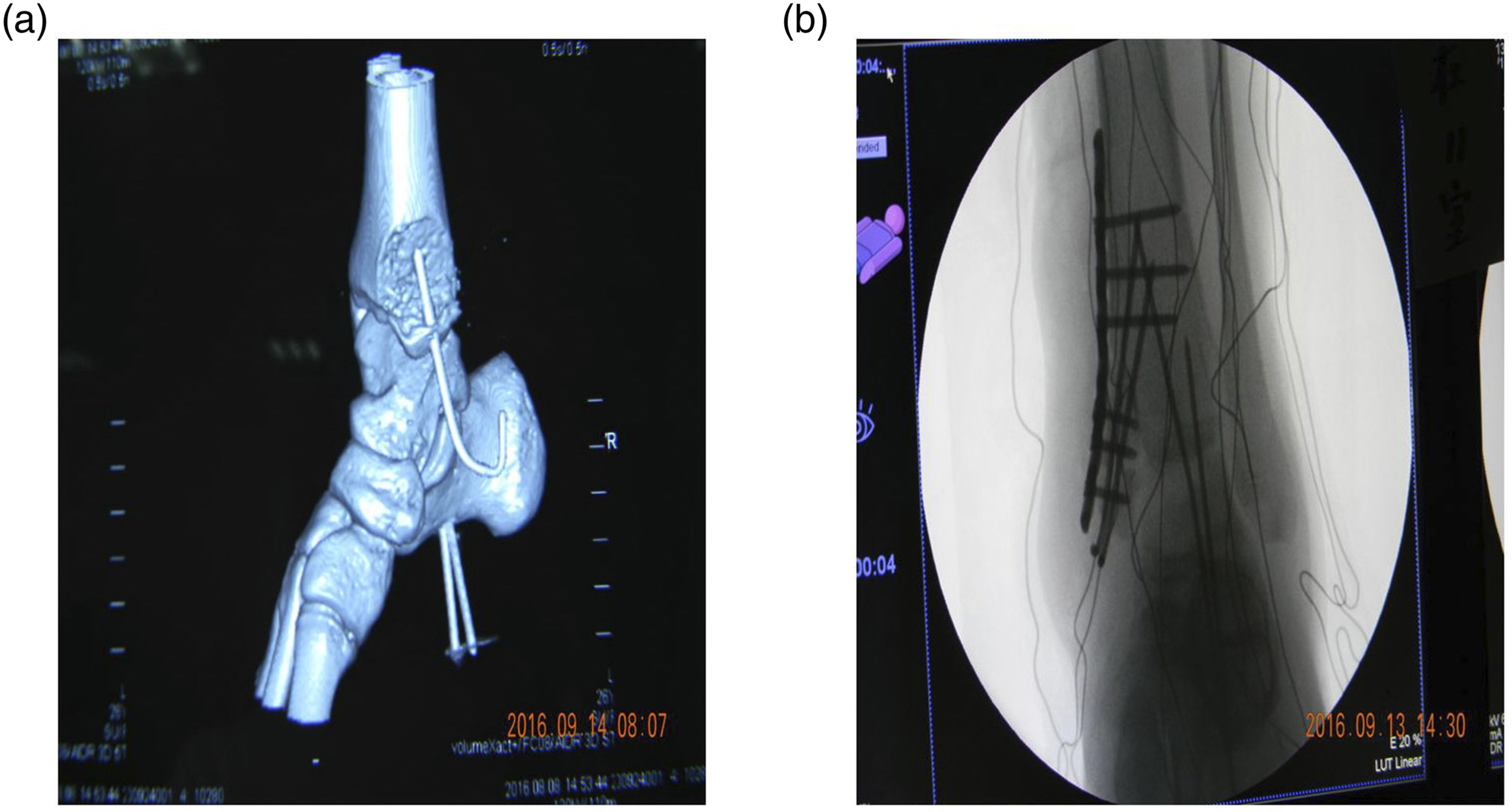
Before the operation, the anteroposterior X-ray (Figure 3(a)) and lateral X-ray film (Figure 3(b)) of the ankle joint were taken to determine the degree and location of ankle joint injury. All skin flaps survived well post the operation. CT image showed that the ankle was well fixed (Figure 4(a)). X-Ray at 3 months showed partial callus formation and the patients underwent partial weight-bearing exercise (Figure 4(b)). The anteroposterior X-ray film (a) and lateral X-ray film (b) of the ankle joint prior to operation. CT image and X-ray image post the operation. (a). Image for CT determination showing well fixed ankle. (b). Image for X-ray at 3 months.
Postoperative recovery of typical case
The suture was removed 14 days after the operation, and the incision healed in the first stage (Figure 5(a)). Six weeks post the operation, non-weight bearing functional exercise of the ankle joint was started. The anteroposterior X-ray film (Figure 5(b)) and lateral X-ray film (Figure 5(c)) of the ankle were reexamined every 2–3 months. After 3 months of follow-up, the right ankle joint was in good state and began to load. The postoperative X-ray showed that the ankle joint space was normal. After 11 months of follow-up, the range of ankle flexion and extension was 45–60°, and the gait was normal. The overall photos of follow-up showed good wound closure (Figure 5(d)). There was no obvious pain when walking. The score was 92, and ankle function was excellent. Healing for medial soft tissue and medial malleolus loss of typical patient. (a). The suture of patient. (b). The anteroposterior X-ray film of ankle. (c). The lateral X-ray film of ankle. (d). General image for the follow-up (11 months post the operation) showing well closed wound.
Discussion
Clinically, there are four types of medial malleolus loss,7,8,12-16 including medial malleolus soft tissue and partial cortical bone loss (type Ⅰ), medial malleolus soft tissue and non-weight bearing articular surface loss (type Ⅱ), medial soft tissue and medial malleolus loss (type Ⅲ) and distal tibia soft tissue and weight bearing articular surface loss (type Ⅳ). Among them, the medial soft tissue and medial malleolus loss (type Ⅲ) is more complicated with a large number of tissue structure defects, which make surgical repair more difficult. 17 At the same time, the incidence rate of medial soft tissue and medial malleolus loss (type Ⅲ) is significantly higher than that of type Ⅳ. Therefore, this study mainly focused on the application of posterior tibial artery perforator technique combined with iliac crest autograft in treating the medial soft tissue and medial malleolus loss. In this study, a series of iliac bone autograft with skin flaps were used in the early stage. Artificial joint replacement or arthrodesis was feasible, if severe dysfunction occurred in the end stage.
Clinically, iliac bone autograft repair has no serious complications and demonstrates good biomechanical properties 18 and fibrocartilage ability.19,20 Therefore, iliac bone is considered to be the first choice for the bone transplantation. In recent years, the posterior tibial artery medial supramalleolar perforator flap has been widely applied in clinical repair, which effectively solves the problem of soft tissue defect of dorsum of foot and ankle.21,22 Therefore, this study used the posterior tibial artery perforator technique combined with iliac crest autograft to repair the medial soft tissue and medial malleolus loss. However, in most countries with bone banks, allogeneic bone grafts are used to treat the medial malleolus loss. While, treatment of iliac crest does not require additional surgery, and allogeneic bone transplantation is more suitable for patients.
According to the intraoperative experience, we should pay attention to the following points. First, CT scan is conducted on the affected side before the operation, and X-ray films are taken on the healthy side of the ankle joint. The width, length and articular surface angle of medial malleolus are measured to accurately establish the bone model and match the surface of iliac cartilage with the surface of the ankle joint. Second, the amount of iliac bone autograft is 10%–20% more than that of the defect. Third, the position, shape and diameter of the perforator are determined by the preoperative color Doppler, so as to select the appropriate flap and finally solve the problem of wound coverage. Fourth, it is necessary to stop bleeding before closing the donor regions to avoid hematoma compressing the proximal blood vessels of limbs, resulting in the disorder of flap blood supply. Fifth, due to the skilled operation, no serious donor region complications, such as nerve injury, pain and certain dysfunction, are found. Sixth, the choice of operation time is more important. The most appropriate operation time is about 7–10 days after the first stagy of emergency operation. Because the wound is in the inflammatory reaction stage at 3–7 days after the operation, the possibility of infection in the affected area after flap transfer is high, and the survival rate is low. If more than 2 weeks, fibrous tissue will proliferate, which may affect the treatment of vascular anastomosis, leading to vascular embolism and flap necrosis. However, the length of postoperative time is only a reference index. The most important reference standard is to confirm that the wound is clean and there is no obvious evidence of infection or inflammation.
This study also showed a few limitations. First, during follow-up, the iliac bone autograft caused bone resorption and articular cartilage atrophy for a long time. Second, compared with the free operation of common deep iliac circumflex vascular iliac composite flap, the operation risk of the present treating method was significantly reduced, however the clinical effects need long-time observation and strict follow-up. Third, some radio-images (CT or X-ray images) and damaged limbs images were small, backward or distorted, because these were difficult to take during the operation. Fourth, this study was a case series, however a randomised control trial (RCT) would be better, but would be unlikely to be feasible because of the small number of injured cases (small sample size).
Conclusion
In this study, the posterior tibial artery perforator technique combined with iliac crest autograft was used to treat medial soft tissue and medial malleolus loss. The findings demonstrated that posterior tibial artery perforator technique combined with iliac crest autograft treatment was reliable and effective.
Footnotes
Author contributions
Xiaodong Li and Pei Wang conceived the work, interpreted the data, and substantively revised the work. Pei Wang designed the work. Xiaowei Yan, Qiang Xie, Rui Gu analyzed and interpreted the data. Xiaodong Li drafted the work. Xiaowei Yan, Qiang Xie, Rui Gu, Zhixue Wang, Fei Liu, Lei Sui, Changyu Yu, Pei Wang substantively revised the work. All the authors approved the submitted version and agreed to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by the Ethical Committee of Affiliated Hospital of Chengde Medical College. All patients involving in this study has been approved and provided the written form consents.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available, but are available to be provided privately on reasonable request.