
Abstract
Objectives
To measure levels of pain and iliac regeneration at the iliac crest donor site during a 10-year follow-up of graft patients.
Methods
This prospective study used a visual analogue scale (VAS) to assess pain at the donor site at 1 month and 1, 3, 5 and 10 years postoperatively. Iliac regeneration status was recorded at 1, 3, 5, 7 and 10 years postoperatively by comparing plain radiographs.
Results
A total of 32 patients participated in the study. Mean VAS scores at 1 month, 1 year, 3, 5, and 10 years were 3.22, 3.39, 3.45, 2.02 and 1.38, respectively. There was no statistically significant difference between pain scores at 1 month and 1 year, but pairwise comparisons revealed significant differences between the other timepoints. The mean iliac regeneration rank scores at 1, 3, 5, 7 and 10 years were 1.36, 2.22, 2.97, 3.75 and 4.70, respectively; all pairwise comparisons were statistically significant.
Conclusion
The iliac donor site showed a declining trend in pain, which appeared to have started 3 years postoperatively. Long-term follow-up showed that the ilium is readily able to repair itself.
Introduction
Iliac graft harvesting is associated with considerable postoperative pain and discomfort. 1 The pain at the donor site may persist and represents a significant source of postoperative morbidity. The incidence of relevant pain after bone-graft harvesting from the iliac crest at 3 months, 6 months and 2 years is reportedly 29%, 38% and 19%, respectively.2,3 However, long-term follow-up of the donor site has not extended to 10 years.
The aim of the present study was to describe the results of a 10-year follow-up of the status of the iliac donor site, particularly with respect to pain and bone regeneration.
Patients and methods
Study population
Adult patients scheduled to undergo internal fixation for various fractures using autogenous bone grafts were sequentially enrolled in this prospective study at the Department of Orthopaedics, Third Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China between January 2000 and December 2002. Patients with an American Society of Anesthesiologists (ASA) physical status of 1 or 2, aged between 30 and 40 years, were eligible for participation. Patients with multiple fractures, or fractures that required a secondary operation for non-union, were excluded from this study. Smokers were also excluded from the study. Institutional ethics committee approval was obtained from the Third Hospital of Hebei Medical University. Written informed consent was obtained from all patients.
Iliac crest bone harvesting
An autograft was harvested from the anterior iliac crest in all patients. An incision of nearly 7 cm in length was made just below the anterior iliac wing, parallel to the iliac crest and centred over the iliac tubercle. Next, the skin was retracted to identify the iliac crest, and a scalpel was used to create an incision down onto the crest by stripping off the muscle from either the inner or outer wall of the ilium. Following the contour of the bone, a sharp dissection was carefully made to avoid straying out of the plane and into the soft tissue. The dissection was extended around the corner of the crest onto the ilium using a Cobb elevator to obtain a complete 3 × 2 cm block of the ilium. Dissection was very carefully performed to avoid retraction of the inguinal ligament and a resultant inguinal hernia. The wound was irrigated with antibiotics and saline, and soft tissue haemostasis was achieved with bipolar cautery. The wound was closed, and internal fixation of the corresponding parts of the fracture was performed. One dose of cefuroxime (2.0 g) was given by intravenous administration preoperatively, followed by two additional doses during the first 24 h postoperatively.
Assessment of iliac pain and iliac bone regeneration
Patients self-reported their pain using a visual analogue scale (VAS; 0, no pain; 10, worst pain imaginable) at 1 month and 1, 3, 5 and 10 years postoperatively. Plain radiographs of the hip graft site were obtained preoperatively and at 1, 3, 5, 7 and 10 years postoperatively, and the status of iliac regeneration was determined by two senior orthopaedic trauma physicians (L.Q. and Y.Z.). The status of iliac regeneration was divided into four levels, based on the comparison with plain preoperative radiographs. At level I, the amount of new bone volume was <30% of the original bone volume; at level II, the amount of new bone volume was ≥30% to ≤50% of its original volume; at level III, the amount of new bone volume was >50% to ≤70% of its original volume; at level IV, the amount of new bone volume was >70% of the original bone volume. The levels of iliac regeneration (I–IV) were given the rank scores of 1, 2, 3 and 4, respectively.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®.
The Friedman test and Wilcoxon signed-rank test were used to generate mean rank scores.
A P-value of <0.05 was considered to be statistically significant.
Results
Thirty-six patients were asked to participate; four patients declined. The mean age of the patients (20 male, 12 female) was 33 years (range 31–39 years). The ASA physical status of 30 patients was level 1, and that of two patients was level 2 because of controlled hypertension. Of the 32 patients, the autologous iliac crest bone of seven patients was used for humeral shaft fracture transplantation, that of 20 patients was used for femoral shaft fracture transplantation, that of three patients was used for tibial shaft fracture transplantation, and that of two patients was used for radial and ulnar fracture transplantation. No postoperative infections occurred in any patient. All fractures had healed by 9 months postoperatively (range 6–13 months). All patients returned to their previous activities or occupations.
Status of postoperative bone regeneration at the iliac crest bone graft donor site, as determined by two senior orthopaedic trauma physicians, based on comparison with plain preoperative radiographs, in patients (n = 32) who underwent iliac crest bone graft harvesting.

Data presented as n of patients unless otherwise stated.
Status of iliac regeneration was divided into four levels: level I, amount of new bone volume <30% of original bone volume; level II, amount of new bone volume ≥30 but ≤50% of its original volume; level III – the amount of new bone volume was >50% to ≤70% of its original volume; level IV, amount of new bone volume was >70% of original bone volume.
Levels of iliac regeneration (I–IV) were given mean rank scores of 1, 2, 3 and 4, respectively.
P < 0.001 for all postoperative comparisons; Friedman test and Wilcoxon signed-rank test.
Extent of postoperative pain at the bone graft donor site, scored using a visual analogue scale (VAS) in patients (n = 32) who underwent iliac crest bone graft harvesting.
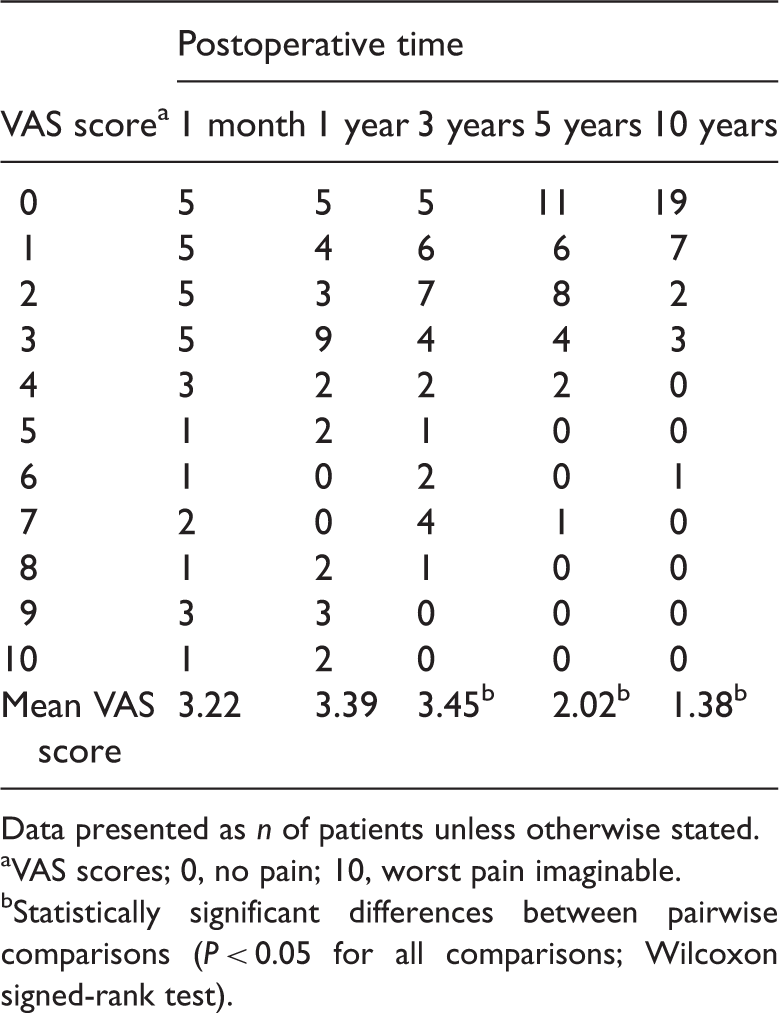
Data presented as n of patients unless otherwise stated.
VAS scores; 0, no pain; 10, worst pain imaginable.
Statistically significant differences between pairwise comparisons (P < 0.05 for all comparisons; Wilcoxon signed-rank test).
Discussion
Iliac crest autografting is considered to be the gold standard grafting technique in fracture internal fixation procedures and in some spinal fusion surgeries. 1 Harvesting of the iliac crest graft is associated with morbidity, particularly persistent pain at the graft harvest site, in up to one-third of patients.4,5 However, the most recent studies have reported incidences of relevant pain with a follow-up of ≤3 years. 5
The present study is is the first prospective study to examine pain and bone regeneration with a follow-up of 10 years. In this study, we found that pain was significantly lower 3 years postoperatively compared with 1 year postoperatively. This reduction in pain was primarily exhibited because fewer patients reported severe pain as the postoperative time increased. This result may affect the number of orthopaedic surgeons who propose reconstruction of the iliac crest to reduce pain.
Several methods to reduce graft site pain are currently available. For example, Tanishima et al. 6 recommended rounding off the graft harvest site edges. Reconstruction of the graft site with resorbable mesh has been shown to reduce early postoperative pain. 7 Continuous application of 0.2% ropivacaine through an iliac crest catheter with iliac crest bone grafting was demonstrated to be an effective method for pain relief for the first 48 h, and the benefit of this technique was still present after 3 months. 8 However, most of these were retrospective studies with shorter follow-up times, which seriously affected their credibility. This present study revealed a declining trend in pain, which appeared to have started 3 years postoperatively, suggesting that pain relief does not require ilium reconstruction.
This present study also observed the phenomenon of bone regeneration. The results demonstrated that the ilium exhibited a good ability to repair itself in the long term. This was perhaps related to the choice of patients, who were younger people (aged 30–40 years) with fractures and no medical comorbidities (ASA physical status of 1 or 2). This present study selected younger rather than older patients with spinal diseases to ensure successful completion of a 10-year follow-up; thus, the extent of iliac regeneration may have been exaggerated in this study. This present study sought to determine whether bone regrowth at the harvest site was associated with pain relief, but it was unable to determine this because the sample size was too small. This problem requires further investigation in a multicentre prospective study with a larger sample size.
In conclusion, this present study demonstrated that the iliac crest bone graft donor site showed a declining trend in pain over the follow-up period, which may have started at 3 years postoperatively. Analysis of plain radiographs demonstrated that the ilium was readily able to repair itself over the long term.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.