
Abstract
Purpose
Although the understanding of the mechanisms of low back pain due to spinopelvic sagittal imbalance has strengthened, the understanding of the mechanisms of neck pain remains insufficient. Thus, this study aimed to identify the factors associated with preoperative and postoperative neck pain in patients with degenerative cervical myelopathy who underwent laminoplasty.
Methods
In this prospective multicenter study, we prospectively enrolled patients who were scheduled for laminoplasty for degenerative cervical myelopathy. The associations between different variables and the Numerical Pain Rating Scale (NRS) scores for neck pain were investigated using univariate and multiple linear regression models.
Results
In total, 92 patients were included in the current study. The univariate analysis showed that age, sex, cervical lordosis in neutral and extension, and thoracic kyphosis were significantly associated with the preoperative NRS score for neck pain; moreover, preoperative cervical lordosis in extension and range of motion and postoperative cervical lordosis in neutral, flexion, and extension were significantly associated with the postoperative NRS Scale score for neck pain. Stepwise multiple regression analysis showed that the independent factors contributing to preoperative neck pain were preoperative cervical lordosis in extension, sex, and age. The independent preoperative predictor and contributor to postoperative neck pain were preoperative cervical lordosis in extension and postoperative cervical lordosis in extension, respectively.
Conclusions
Cervical lordosis in extension showed significant association with neck pain in patients with degenerative cervical myelopathy. Therefore, when performing laminoplasty for patients with a low cervical lordosis in extension, attention should be paid to residual postoperative neck pain.
Introduction
Symptoms of degenerative cervical myelopathy (DCM) include gait disturbance, numbness of the limbs, and clumsiness.1–3 Neck pain is not a major but often associated symptom of DCM. For DCM patients with progressive neurological symptoms, surgery can provide symptomatic relief. 4 Among several surgical procedures, cervical laminoplasty has been one of the most frequently performed surgical procedures to treat DCM.5,6 However, to our knowledge, there are few reports of improvement in neck pain beyond the minimum clinically important difference with laminoplasty.3,7 This suggests that factors other than the involvement of spinal cord or nerve compression may have a more significant influence on neck pain.
In recent years, while the understanding of the onset mechanism of low back pain due to spinopelvic sagittal imbalance has strengthened, 8 the understanding of the onset mechanism of neck pain remains insufficient. A retrospective study has reported that independent preoperative predictors of moderate to severe neck pain at 2-year follow-up included the presence of anterolisthesis, current smoking, moderate to severe baseline neck pain, and lower 36-item Short Form Survey Mental Component Summary scores. 9 However, whether the postoperative status of these factors was associated with postoperative neck pain has not been explained. 9 Notably, residual neck pain after laminoplasty impairs a patient’s quality of life (QOL). 10 Therefore, identifying the factors associated with neck pain in patients with DCM before and after surgery is crucial in developing strategies to improve neck pain and enhance patient’s QOL. Among preoperative factors associated with preoperative neck pain and postoperative factors associated with postoperative neck pain, we hypothesized that the factors commonly present in the preoperative and postoperative periods would be true factors associated with neck pain. This study aimed to identify factors associated with preoperative and postoperative neck pain in patients with DCM who underwent laminoplasty and factors that predict residual postoperative neck pain.
Materials and methods
Study population
This multicenter study initiated by the Japanese Organization of the Study for Ossification of the Spinal Ligament prospectively recruited patients with DCM who were scheduled for surgical treatment at eight participating institutions between October 2016 and December 2017. 4 Surgical indications and procedures (laminoplasty, anterior decompression and fusion, and posterior decompression and fusion) were determined based on factors of individual patients, such as neurological status, presence of anterior compression, and spinal alignment. Of the patients scheduled for surgery for DCM within the time period, those who underwent laminoplasty were included in this study. The indications for laminoplasty for patients with DCM in this study varied slightly from institution to institution; they were generally that the cervical alignment in the neutral position was not kyphotic or that the k-line in the flexion position was positive. 11 In laminoplasty, the muscles attached to the C2 spinous process were preserved, as well as those attached to C7, as much as possible. Institutional review board approval was obtained before the initiation of the study (M2016-017). At the time of enrollment, written informed consent was obtained from all participants. Demographic data including age, sex, body mass index, and etiology of myelopathy, were collected.
The exclusion criteria were comorbidities impairing physical function (e.g., cerebral infarction, cerebral palsy, or severe rheumatoid arthritis), bedridden status or full dependence on a wheelchair before surgery due to severe cervical myelopathy, and difficulty completing a questionnaire due to cognitive impairment.
During this period, 175 patients with DCM were scheduled for surgery, 106 of whom underwent laminoplasty, and 101 patients were available for 1 year of follow-up. Of the 101 patients, 92 patients were included in the current study, excluding nine patients with missing preoperative and 1-year NRS scores.
Radiologic findings
Cervical lordosis (CL) of the spine was defined by the Cobb angle between C2 and C7 on a lateral radiograph in the neutral position. C2–7 range of motion (ROM) was measured on flexion–extension lateral radiographs. The C7 slope was calculated by measuring the angle formed by the horizontal line to the C7 vertebra and the line parallel to the superior endplate of the C7 vertebra. 12 Thoracic kyphosis (TK) was defined by the Cobb angle between the superior endplate and inferior endplate of T1–T12. 13 The C2–7 sagittal vertical axis (C2–7 SVA) is the sagittal distance between a plumb line dropped from the center of C2 and posterosuperior corner of C7. 14 Lumbar lordosis (LL) was defined as the angle between the superior endplate of L1 and the inferior endplate of L5. 15 Sacral slope was measured between the tangent line to the superior endplate of S1 and the horizontal plane. 16 The SVA is the sagittal distance between the C7 plumb line and the vertical line through the posterosuperior corner of the S1 endplate on standing whole-spine lateral radiographs. 17 Pelvic tilt (PT) is the angle between the vertical reference line from the center of the femoral head and the line from the center of the femoral head to the midpoint of the sacral endplate. 18 The T1 pelvic angle is the angle between the line from the femoral head axis to the centroid of T1 and the line from the femoral head axis to the middle of the S1 endplate. 19
Outcome measures
Outcomes were assessed at enrollment and 1 year after surgery using the Numerical Pain Rating Scale (NRS) score for neck pain and upper exterimity pain and numbness (which ranges from 0 to 10, with higher scores indicating more severe pain). For the method of measuring neck pain and upper extremity pain and numbness in this study, patients were given a schematic drawing of the body and asked to self-report the degree of pain and numbness in each area.
Statistical analysis
Data before and after surgery were compared by paired t-test. Then, the associations between various variables and the preoperative or postoperative NRS scores were investigated using a linear regression model. Then, as a method to identify the independent factors contributing to neck pain, the associations between variables and preoperative or postoperative NRS scores were investigated using a multiple linear regression model. First, predictors associated with the dependent variable at a p-value ≤ .25 in univariate regression analyses were carried forward to the second step of the analysis. Second, the remaining predictors were included in a forward-backward multiple regression analysis. Predictors with a p value >.1 were removed. To assess the cut-off point, a receiver operative characteristic analysis was conducted. The number of cases during the study period determined the sample size. For all statistical analyses, JMP version 14 (SAS Institute, Cary, NC, USA) was used, and a p-value <.05 was considered to indicate statistical significance.
Results
Patient demographics
Demographic data of patients.

Abbreviations: Body mass index (BMI); Ossification of the posterior longitudinal ligament (OPLL); Numerical pain rating scale (NRS); Cervical lordosis (CL); Range of motion (ROM); Sagittal vertical axis (SVA); Thoracic kyphosis (TK); Lumbar lordosis (LL); Sacral slope (SS); Pelvic tilt (PT); T1 pelvic angle (TPA).
ΔNRS score=NRS score at preoperative – NRS score at 1 year postoperatively.
Data are presented as mean ± SD.
ap < .05.
Factors contributing to neck pain
Univariate regression analysis. Association of preoperative variables with preoperative neck pain.
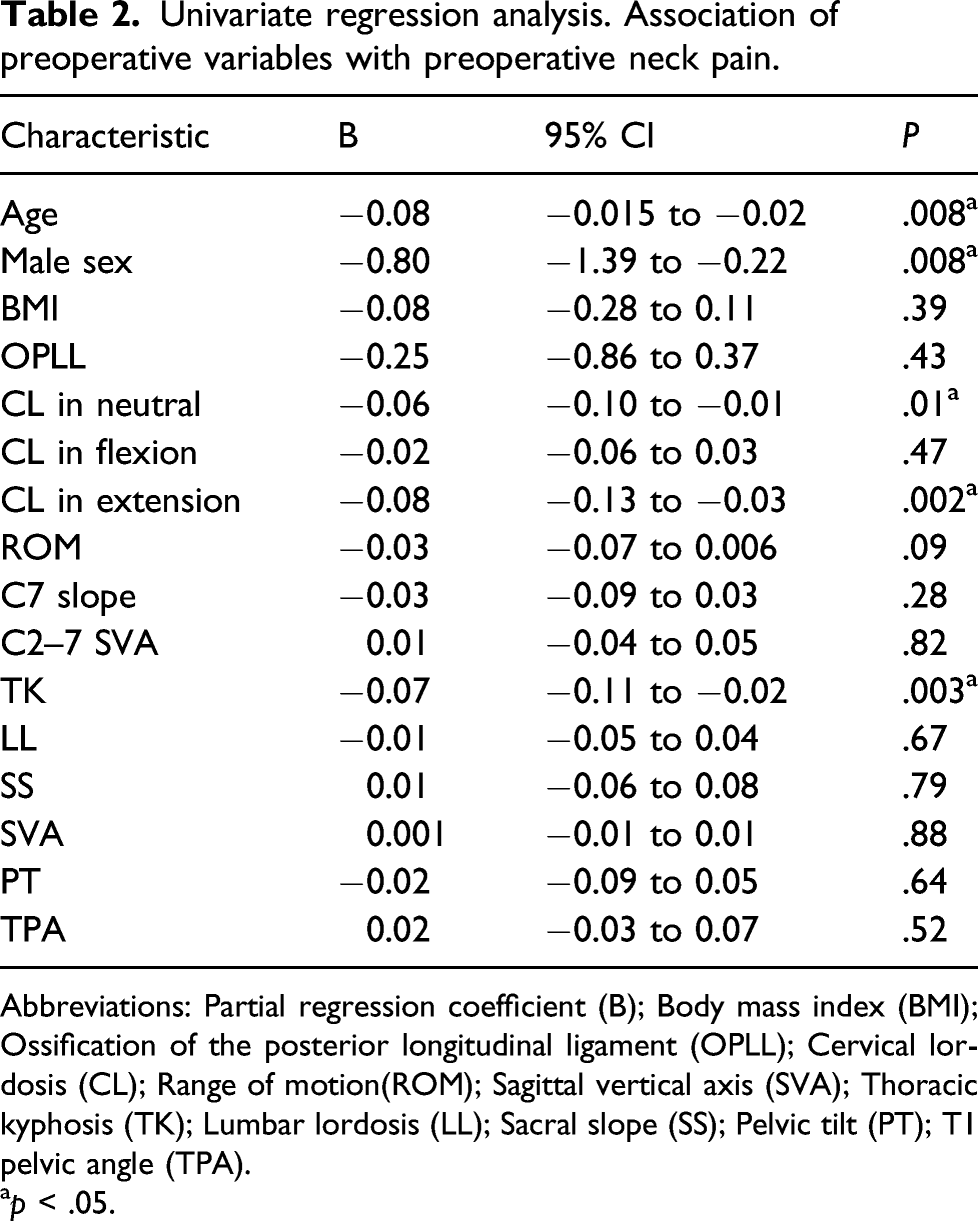
Abbreviations: Partial regression coefficient (B); Body mass index (BMI); Ossification of the posterior longitudinal ligament (OPLL); Cervical lordosis (CL); Range of motion(ROM); Sagittal vertical axis (SVA); Thoracic kyphosis (TK); Lumbar lordosis (LL); Sacral slope (SS); Pelvic tilt (PT); T1 pelvic angle (TPA).
ap < .05.
Univariate regression analysis. Association of preoperative and postoperative variables with postoperative neck pain.

Abbreviations: Partial regression coefficient (B); Body mass index (BMI); Ossification of the posterior longitudinal ligament (OPLL); Cervical lordosis (CL); Range of motion (ROM); Sagittal vertical axis (SVA); Thoracic kyphosis (TK); Lumbar lordosis (LL); Sacral slope (SS); Pelvic tilt (PT); T1 pelvic angle (TPA).
ap < .05.
Stepwise multiple regression analysis: independent predictors of neck pain.
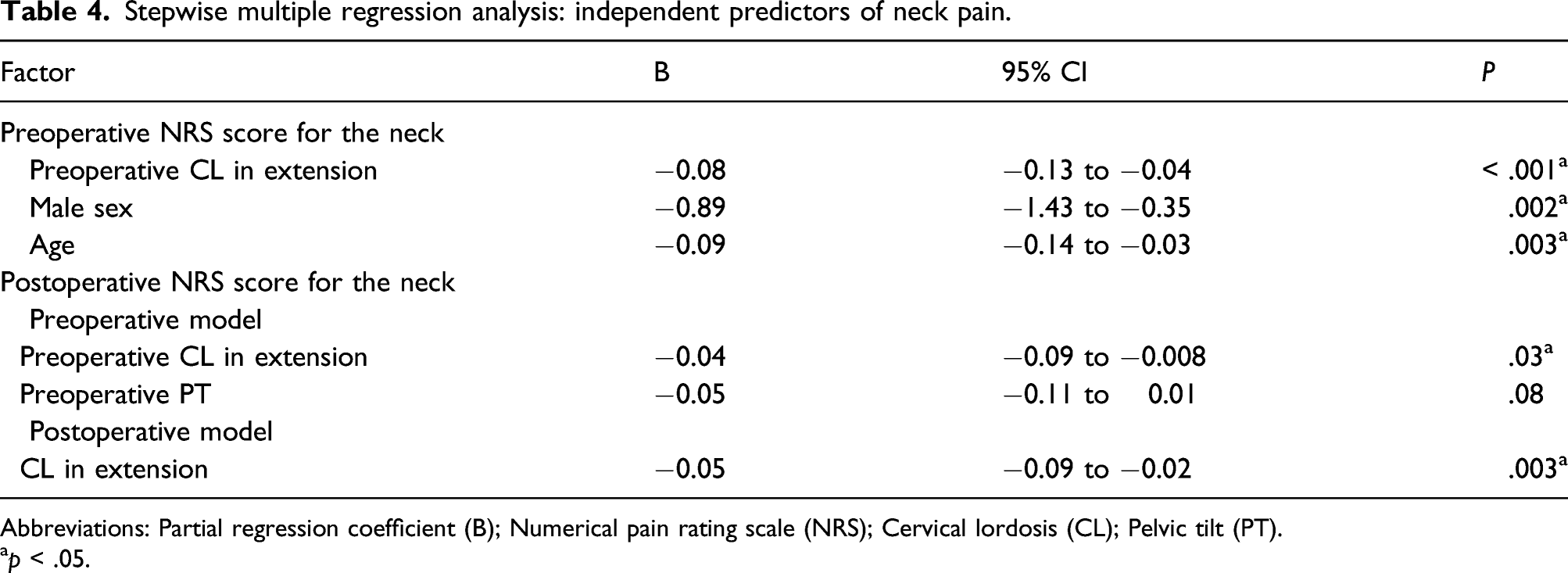
Abbreviations: Partial regression coefficient (B); Numerical pain rating scale (NRS); Cervical lordosis (CL); Pelvic tilt (PT).
ap < .05.
Lastly, we determined the cut-off value of preoperative CL in extension in predicting postoperative residual neck pain by receiver operating characteristic analysis. The optimum cut-off value of preoperative CL in extension was determined to be 28.0°. At this level, the sensitivity and specificity were 0.85 and 0.52, respectively.
Discussion
The NRS score for neck pain improved significantly from a mean of 2.6 points to 1.9 points at 1 year postoperatively in this study. In general, improvements in pain severity of ≤1.5 points on the NRS could be seen as clinically insignificant. 20 Thus, laminoplasty did not improve neck pain to a clinically significant degree in this study. Similar to the results of this study, there were no clinically significant differences in neck pain before and after laminoplasty in previous studies.7,21,22 Therefore, it may be necessary to inform patients preoperatively that neck pain, a common symptom of cervical myelopathy, may not improve to a clinically significant degree even if surgical decompression of the spinal cord is achieved.
CL in extension decreased significantly from a mean of 26.8°–22.5° at 1 year postoperatively in this study. The postoperative decrease in CL was presumably due to the invasion of the posterior elements of the cervical spine. Although CL in extension was still involved in neck pain at 1 year postoperatively as it was preoperatively, the fact that both neck pain and CL are reduced postoperatively is an interesting phenomenon. We believe that preoperative neck pain may be related to factors other than cervical alignment and degeneration of facet joints, such as neurogenic pain due to pressure on the cervical spinal cord or nerve root. The fact that NRS scores for neck pain statistically decreased postoperatively compared to preoperatively, despite the added surgical invasion of the neck, may be an indirect proof that compression on the cervical spinal cord is related to preoperative neck pain. As low back pain improved after surgery for lumbar spinal canal stenosis in the prospective studies,23,24 it is not surprising that cervical spinal cord compression can induce neck pain.
The stepwise multiple regression analysis showed that CL in extension was an independent predictor of neck pain at each time point. These results are slightly different from the results of a previous prospective study that found no correlation between neck pain and cervical parameters before or after laminoplasty. 7 However, the previous study had a small sample size of 35 patients in the cervical spondylotic myelopathy group and 22 patients in the ossification of the posterior longitudinal ligament group and did not measure CL in extension. 7 Regarding the relationship between neck pain and radiological factors, the relationship between neck pain and cervical range of motion has been examined.25,26 And in the results of those papers, cervical range of motion was not significantly associated with neck pain after laminoplasty.25,26 Interestingly, Fujimori et al. 25 reported that change in neck pain after laminoplasty was associated with change in the C2-7 Cobb angle on extension. Unfortunately, they did not directly examine the correlation between CL in extension and neck pain.
A prospective study found that anterior decompression with fusion improved neck pain from 3.7 points preoperatively to 2.1 points postoperatively, which exceeds the clinically significant improvement of 1.5 points.4,20 Moreover, a retrospective study has shown that anterior fusion procedures provide good axial pain relief. 27 In addition, in the present study, preoperative CL in extension was an independent predictor for postoperative neck pain. Therefore, to improve neck pain, it may be better to choose anterior decompression with fusion, if possible, for patients with severe neck pain and low CL in extension preoperatively. This treatment strategy should be prospectively studied in the future.
According to the prediction model in this study, preoperative neck pain was stronger in patients with less cervical extension angle. A common feature of myelopathy is an increase in symptoms while extending the neck. This occurs because the ligamentum flavum will bulge in response to neck extension, thus exacerbating stenosis. 28 Therefore, the association between preoperative CL in extension and neck pain may be related to spinal cord compression due to neck extension. Furthermore, degeneration of the facet joints may be involved in the reduction of the cervical extension angle. However, even after the cervical spinal cord compression was relieved after surgery, neck pain was stronger in patients with less cervical extension angle. Accordingly, postoperative neck pain may have originated from either posterior muscle or facet joints rather than spinal cord compression. Therefore, procedures less damaging to the posterior muscle or facet joints may be effective in reducing neck pain after laminoplasty. Shiraishi et al. 29 performed a posterior muscle-preserving selective mono-laminoplasty for cervical myelopathy and reported no worsening of postoperative neck pain.
This study has several limitations. First, the patients did not have the same etiology (cervical spondylotic myelopathy or ossification of the posterior longitudinal ligament), which may have affected the clinical and radiographic outcomes. However, the proportion of different etiologies did not differ significantly among the groups in this study (Table 2 and 3). Thus, in the present study, we included both etiologies for analyses. Second, the final prediction model showed R2 = 0.28, R2 = 0.09, and R2 = 0.10, which means that this model explains 28%, 9%, and 10% of preoperative and postoperative neck pain, respectively. Therefore, various factors other than those found in this study are involved in neck pain. According to Cohen’s guidelines, the fitted multiple regression model depends on R2, and if the value of R2 is between 0.02 and 0.12, the model is weak; between 0.13 and 0.25, it is moderate; and ≥0.26, it is good. 30 Accordingly, the fit of the preoperative prediction model was found to be good, at least statistically. Further prospective studies are required to address these limitations and validate the results of this study.
Conclusion
Loss of CL in extension significantly contributed to neck pain in patients with DCM. Therefore, when performing laminoplasty for patients with a low CL in extension, attention should be directed to residual postoperative neck pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japanese Health and Labor Sciences Research Grant (grant number 201911033B to AO).