
Abstract
Study Design
Ambispective cohort study.
Objectives
1) To define the prevalence of neck pain in patients with degenerative cervical myelopathy (DCM). 2) To identify associated factors of preoperative neck pain in patients with DCM. 3) To assess the neck pain response to surgical intervention.
Methods
757 patients with DCM were enrolled at 26 global sites from 2005 to 2011. A total of 664 patients had complete neck pain scores preoperatively (Neck Disability Index, NDI). The prevalence and severity of neck pain preoperatively and at the 6-months follow-up was summarized. Functional assessments of individuals with and without pain were compared. Associations of preoperative neck pain and related factors were evaluated.
Results
Preoperatively, 79.2% of patients reported neck pain while 20.8% had no neck pain. Of individuals with neck pain, 20.2% rated their pain as very mild, 27.9% as moderate, 19.6% as fairly severe, 9.6% as very severe and 1.9% as the worst imaginable. Functional status (mJOA), number of stenotic levels, age, and duration of symptoms did not significantly differ in patients with and without pain. Factors associated with the presence of neck pain were female gender, BMI ≥27 kg/m2, rheumatologic and gastrointestinal comorbidities, and age <57 years. Neck pain improved significantly from the preoperative examination to the 6-months postoperative follow-up (P < .0001).
Conclusion
Here, we demonstrate a high prevalence of neck pain in patients with DCM as well as a link between gender, body weight, comorbidity and age. We highlight a significant reduction in neck pain 6 months after surgery.
Introduction
Degenerative cervical myelopathy (DCM) is a progressive, non-traumatic spinal condition and the most common cause of spinal cord dysfunction in adults worldwide. 1 It is caused by the degeneration of various components of the spinal column, including the vertebral bodies, discs and supporting ligaments. 2 These age-related, degenerative changes can narrow the spinal canal and ultimately compress the spinal cord. Patients with DCM may present with significant neck pain, loss of fine motor function, hand dexterity and coordination, gait dysfunction with long tract signs, and imaging evidence of cervical cord compression. 2 More than 70% of individuals over the age of 60 years demonstrate radiological evidence of cervical degeneration, however, only one-quarter will exhibit signs and symptoms of mechanical neural compression.3-5 Since the proportion of the global population aged 60-65 years or older has increased continually over the last 55 years, 6 and is estimated to grow rapidly by 55.7% from 900 million in 2015 to 1.4 billion in 2030, 7 knowledge about DCM and its treatment must become a clinical research and public-health priority.
Recent studies have improved our understanding of DCM. Surgery has not only been demonstrated to arrest disease progression, but also to improve functional impairment, disability and quality of life in patients with mild, moderate and severe myelopathy.8,9 Other important findings include the observation that outcomes are similar in patients undergoing anterior vs posterior surgery 10 as well as laminectomy with fusion vs laminoplasty, 11 after controlling for important confounders. Findings indicate functional outcomes can be predicted by preoperative severity, duration of symptoms, smoking status, psychiatric co-morbidities, and presence of impaired gait. 12 Lastly, there are significant regional variations in the demographics, causative pathology, management strategies and surgical outcomes in patients with DCM. 13
However, there is limited evidence addressing the prevalence and severity of neck pain in patients with DCM and the response of neck pain to surgery. Previous studies in this field are limited by the use of generalized pain scoring systems, such as the Visual Analog Scale, and a small number of patients.14-16 Therefore, we sought to address the following research questions with this study: 1) What is the prevalence of neck pain in patients with DCM? 2) What are the associated factors of preoperative neck pain in patients with DCM? 3) Does neck pain respond to surgical intervention? We aimed to answer these questions with the following approaches: 1) Determine the prevalence of neck pain in a cohort of patients with DCM as defined by the Neck Disability Index (NDI). 2) Determine associated factors of preoperative neck pain in these patients with DCM. 3) Determine the response of neck pain 6 months after surgery for DCM.
Methods
Seven hundred and fifty-seven patients with DCM were enrolled in either the AO Spine Cervical Spondylotic Myelopathy North America (CSM-NA, ClinicalTrials.gov Identifier: NCT00285337) or the CSM International (CSM-I, ClinicalTrials.gov Identifier: NCT00565734) studies at 26 global sites from 2005 to 2011.8,9 Participating centers were located in North America (n = 12), Latin America (n = 3), Asia Pacific (n = 6) and Europe (n = 5). Centers were selected if they had adequate patient availability and previous research experience. Investigators were neuro- or orthopedic surgeons who specialized in managing spinal disorders. Institutional research ethics board approval and data sharing agreements were obtained at all centers before starting patient enrollment. Subsequent analyses have explored i) regional variations in baseline demographics, surgical strategies and outcomes, ii) the comparative efficacy of anterior vs posterior surgery 10 and laminoplasty vs laminectomy and fusion, 11 iii) the psychometric properties and the minimum clinically important difference of the modified Japanese Orthopedic Score (mJOA),17-19 and iv) imaging and clinical predictors of surgical outcomes and complications.12,20
Inclusion and Exclusion Criteria
Patients were enrolled in one of these 2 studies if they provided written informed consent and if they met the following eligibility criteria: i) age 18 years or older, ii) symptomatic DCM defined by a combination of at least one symptom and at least one clinical sign of myelopathy, iii) imaging evidence of cervical cord compression, and iv) no prior cervical spine surgery. Patients were excluded if they had asymptomatic DCM, active infection, neoplastic disease, rheumatoid arthritis, trauma, ankylosing spondylitis, or concomitant lumbar stenosis.
Data Collection and Quality Assurance
Extensive data were collected, including patient demographics (eg age, sex, weight, height, comorbidities, smoking status), clinical presentation (eg, symptoms, signs, causative pathology), and surgical treatment (eg, spinal levels operated, approach). Functional impairment and disability were also evaluated using a variety of outcome assessment tools. External research monitors performed on- and off-site evaluations to ensure that the data were accurate, reliable, complete, and that the study followed the protocol.
Assessment of Functional Impairment and Disability
Functional impairment was assessed by the mJOA.17,18 This 18-point score evaluates motor function of the upper and lower extremities, sensation of the upper extremities and micturition. A score of 18 represents normal function, whereas a lower score indicates more severe impairment. Categories of myelopathy severity based on the mJOA have been established and validated. 21 Specifically, mild myelopathy is defined as a mJOA from 15 to 17, moderate as a mJOA from 12 to 14, and severe myelopathy as a mJOA from 0 to 11. The minimum clinically important difference in patients with DCM has been estimated to be between 1 and 2 points. 18
Disability was evaluated using the Neck Disability Index (NDI), ranging from 0 to 100, with a higher score representing more disability.22,23 The NDI is a self-reported measurement specific to neck conditions that assesses pain intensity and impairment in the following domains: personal care, lifting, work, headache, concentration, sleeping, driving, reading and recreation. The pain intensity subscore of the NDI was used as the primary measure of pain in this analysis and is comprised of 6 categories: i) no pain, ii) mild, iii) moderate, iv) fairly severe, v) very severe, and iv) worst imaginable pain.
Operative Treatment
All patients underwent surgical intervention of the cervical spine, including decompression with or without instrumented fusion. The surgical approach, number of operated levels, and use of instrumentation was at the discretion of the treating spinal surgeon. Individuals were treated anteriorly by cervical discectomy and/or corpectomy with fusion; posteriorly by laminectomy with or without instrumented fusion or laminoplasty; or using a combined circumferential approach.
Sample Size and Power
The minimum clinically important difference for the NDI main score was reported to be −7.5 points.21,23,24 In a large prospective study of patients with DCM treated with surgical decompression, the standard deviation for change in NDI at 12-month post-operative follow-up was 20 points. Based on these figures, a sample size of 566 patients would have 99.4% power to detect a change in NDI of −7.5 points.
Statistical Analysis
Baseline descriptive statistics were computed. Continuous variables were described using means, standard deviations and ranges, and categorical variables were summarized using frequencies and percentages. Patients were divided into 2 groups based on their preoperative neck pain levels: (i) no pain and (ii) pain, consisting of the NDI subscores mild, moderate, fairly severe, severe or worst imaginable pain. Logistic regression analysis was conducted to predict the association between the presence of neck pain and baseline demographics, causative pathology and previous nonoperative treatment strategies. Odds ratios with 95% confidence intervals were computed. Bivariate analysis using a Chi-square test was performed to assess the relationship between functional status and neck pain. Paired t-tests were conducted to determine differences in mean NDI pain intensity scores between preoperative and 6 months post-surgery time points. The level for accepting statistical significance was set at .05.
All statistical analyses were performed using XLSTAT version 21.1 (Microsoft®) and SAS/STAT version 9.4 (SAS Institute Inc.). Excel 16.23 (Microsoft®) was used for visualizing figures and tables.
Results
Patient Population
Descriptive Statistics of the Population of 664 Patients.
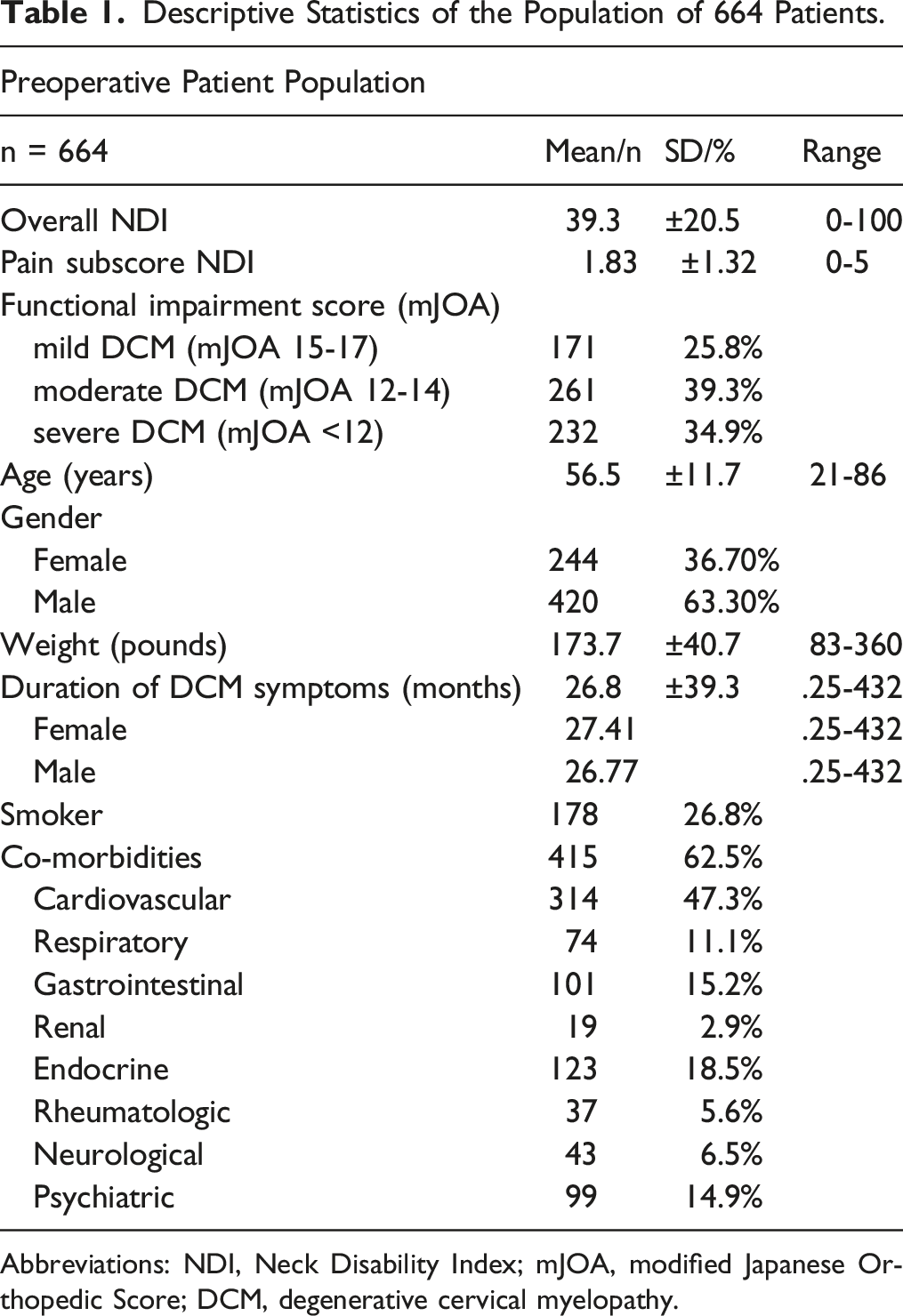
Abbreviations: NDI, Neck Disability Index; mJOA, modified Japanese Orthopedic Score; DCM, degenerative cervical myelopathy.
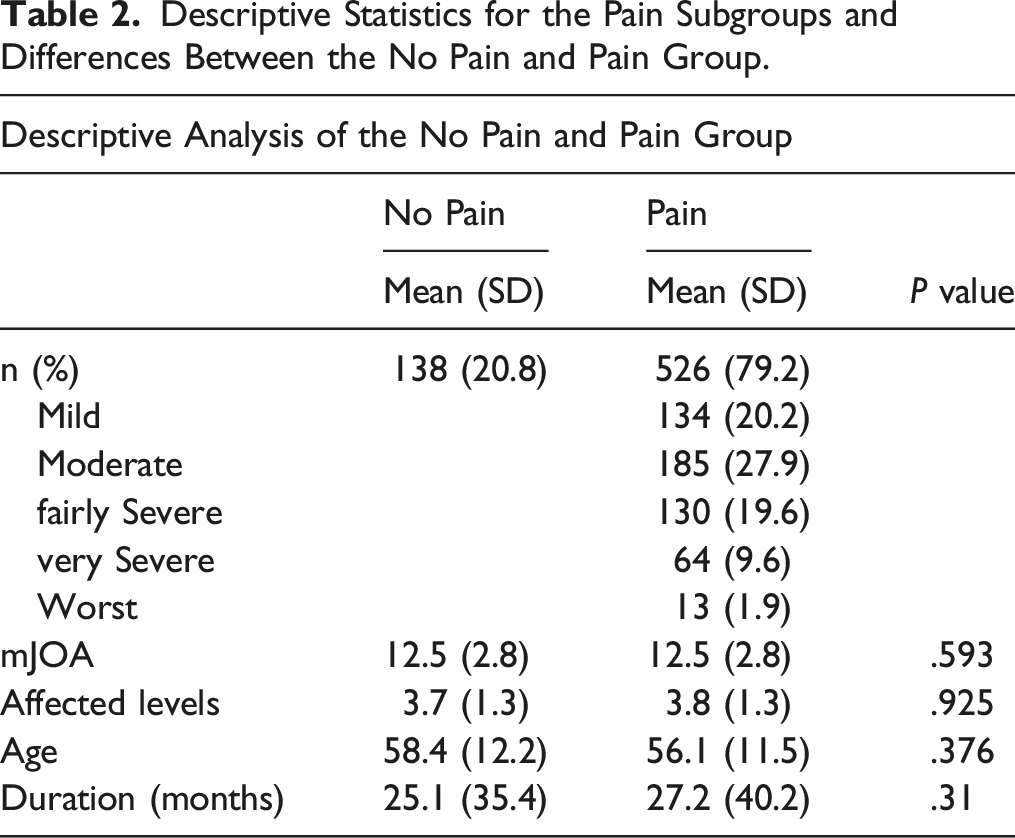
Descriptive Statistics for the Pain Subgroups and Differences Between the No Pain and Pain Group.
Neck Pain Intensity Preoperatively
One hundred and thirty-eight (20.8%) patients reported no neck pain, whereas 526 (79.2%) reported having neck pain of varying intensity (Table 2). Of these, 134 patients (20.2%) rated their pain as very mild, 185 (27.9%) as moderate, 130 (19.6%) as fairly severe, 64 (9.6%) as very severe and 13 (1.9%) as the worst imaginable. Flow chart of the study population and the 6 NDI subscore populations.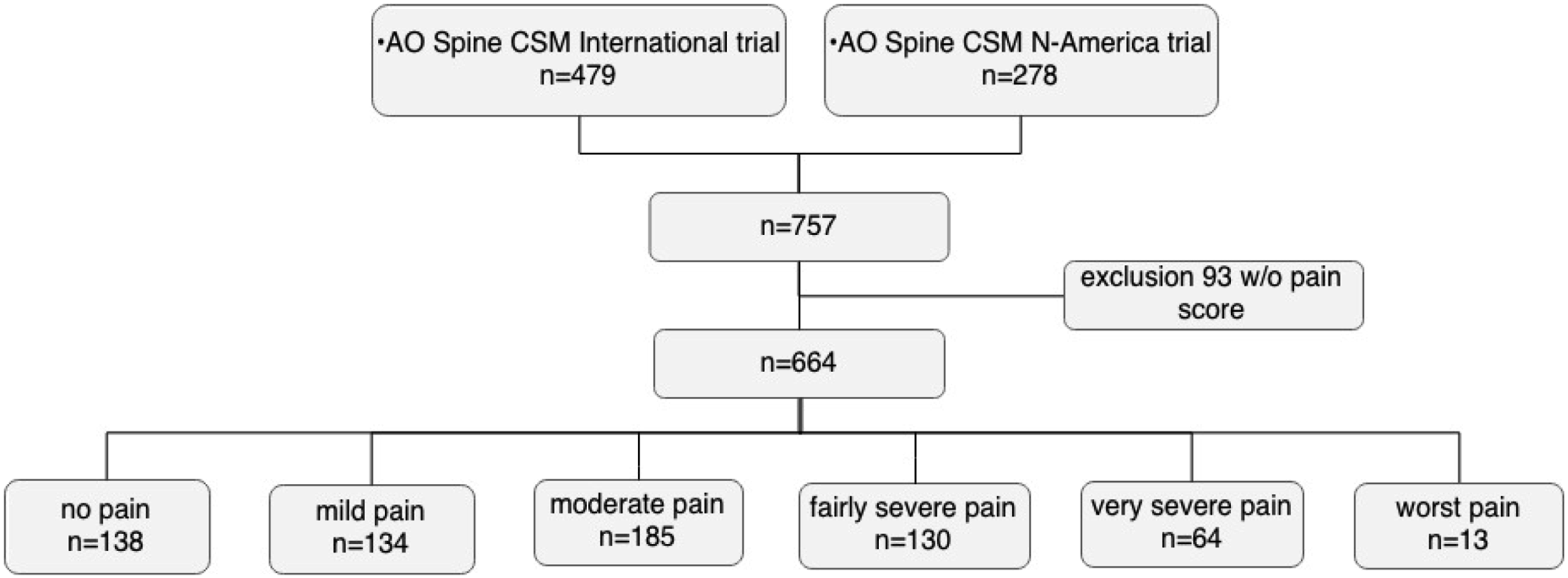
Associated Factors of Neck Pain Preoperatively
Univariable Analysis of Predictors for Neck Pain.
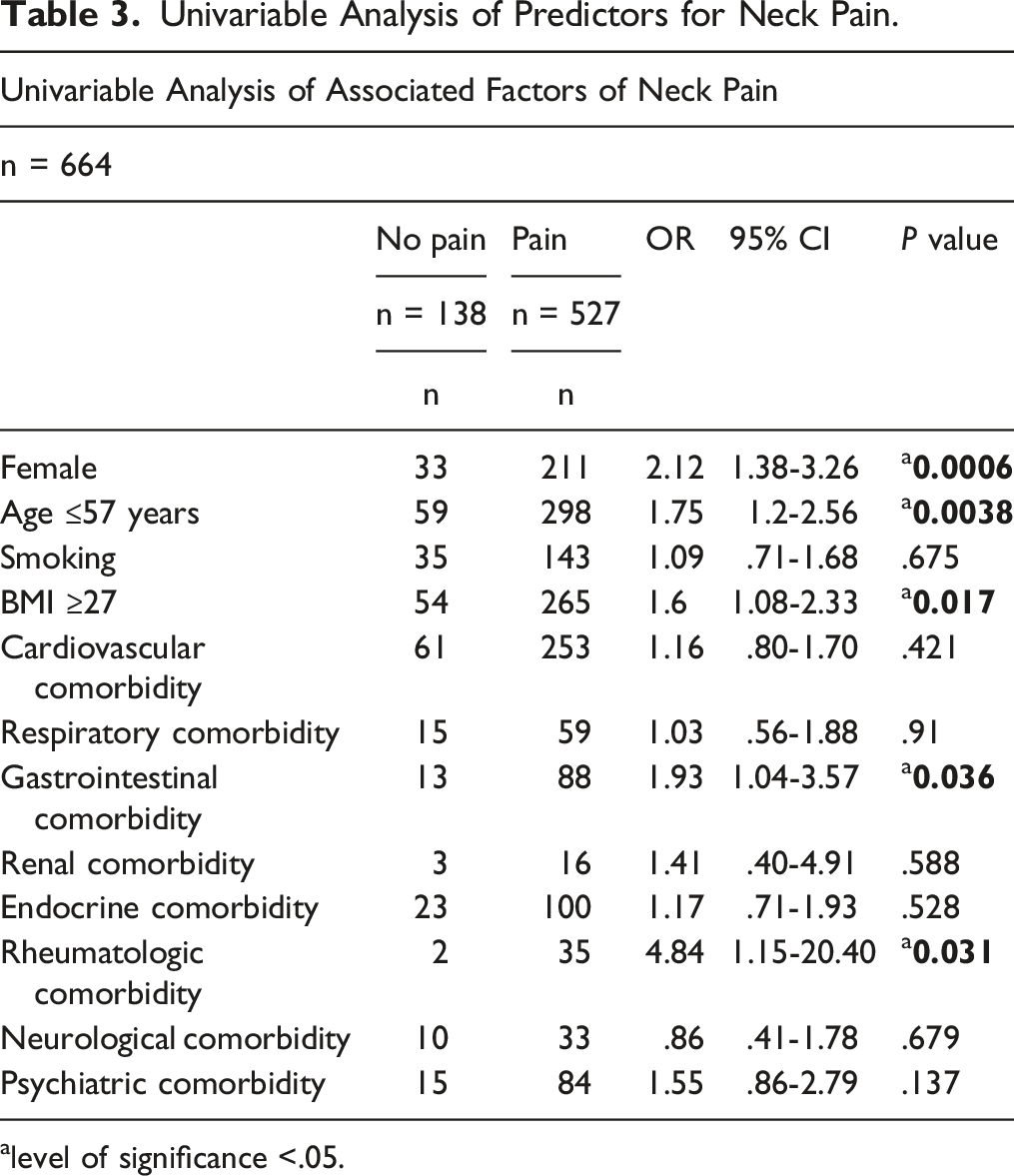
alevel of significance <.05.
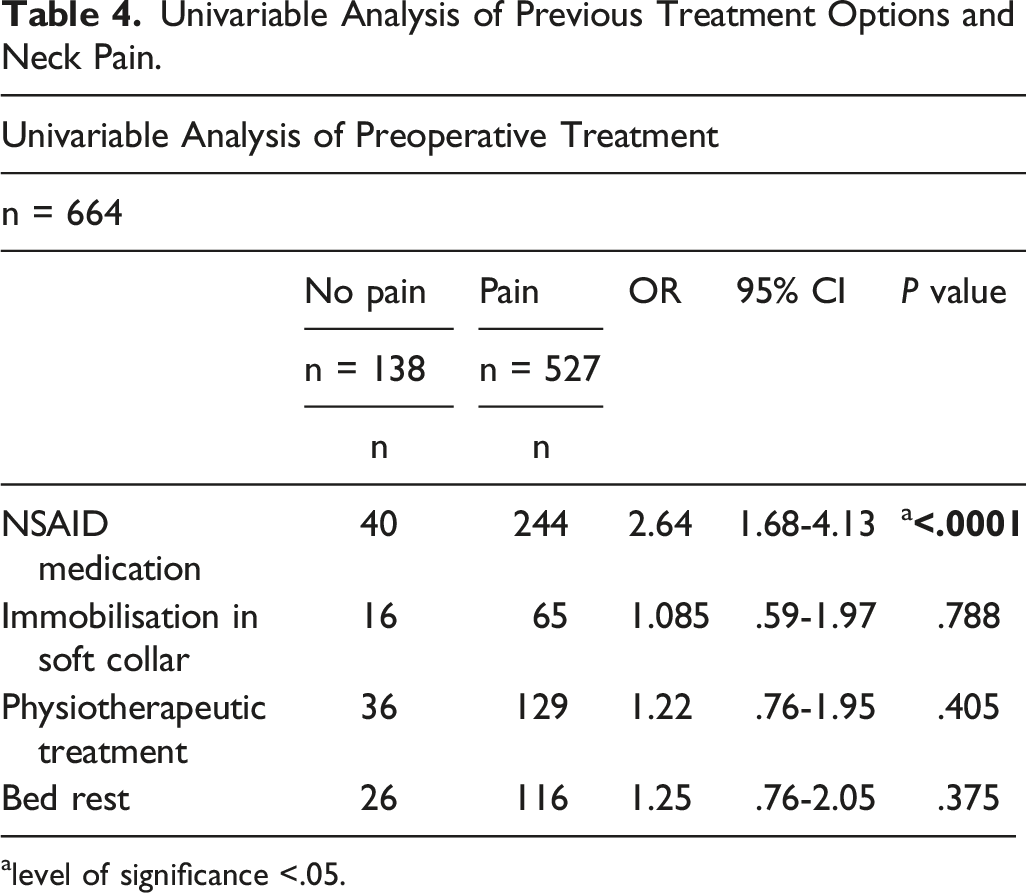
Univariable Analysis of Previous Treatment Options and Neck Pain.
alevel of significance <.05.
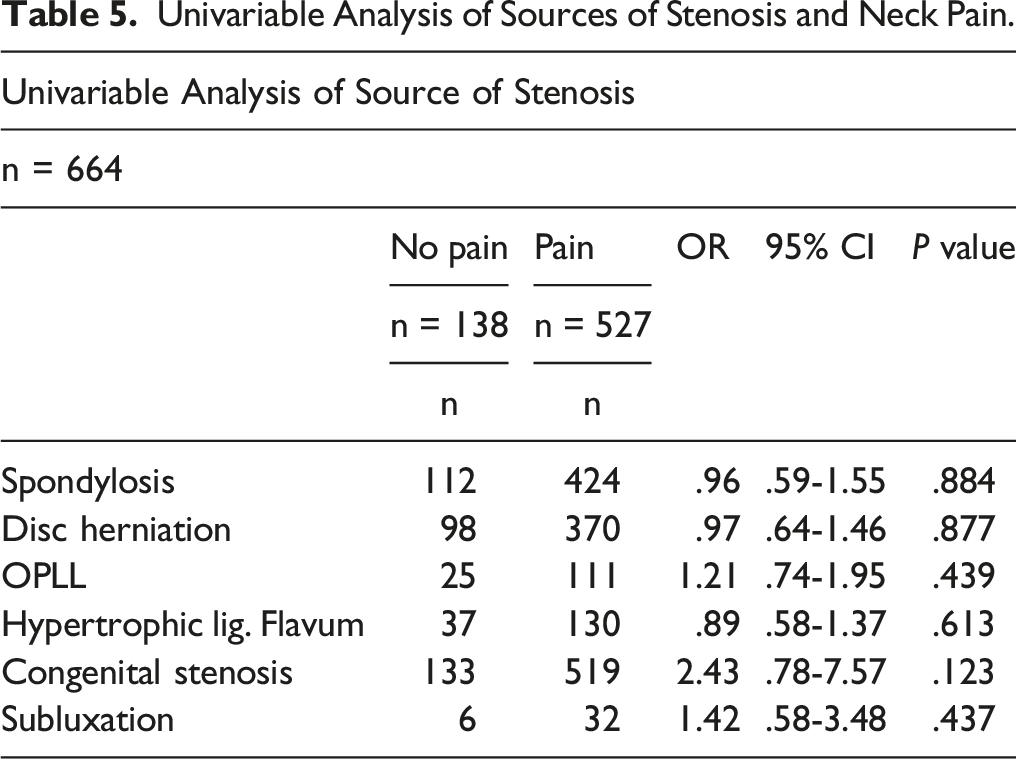
Univariable Analysis of Sources of Stenosis and Neck Pain.
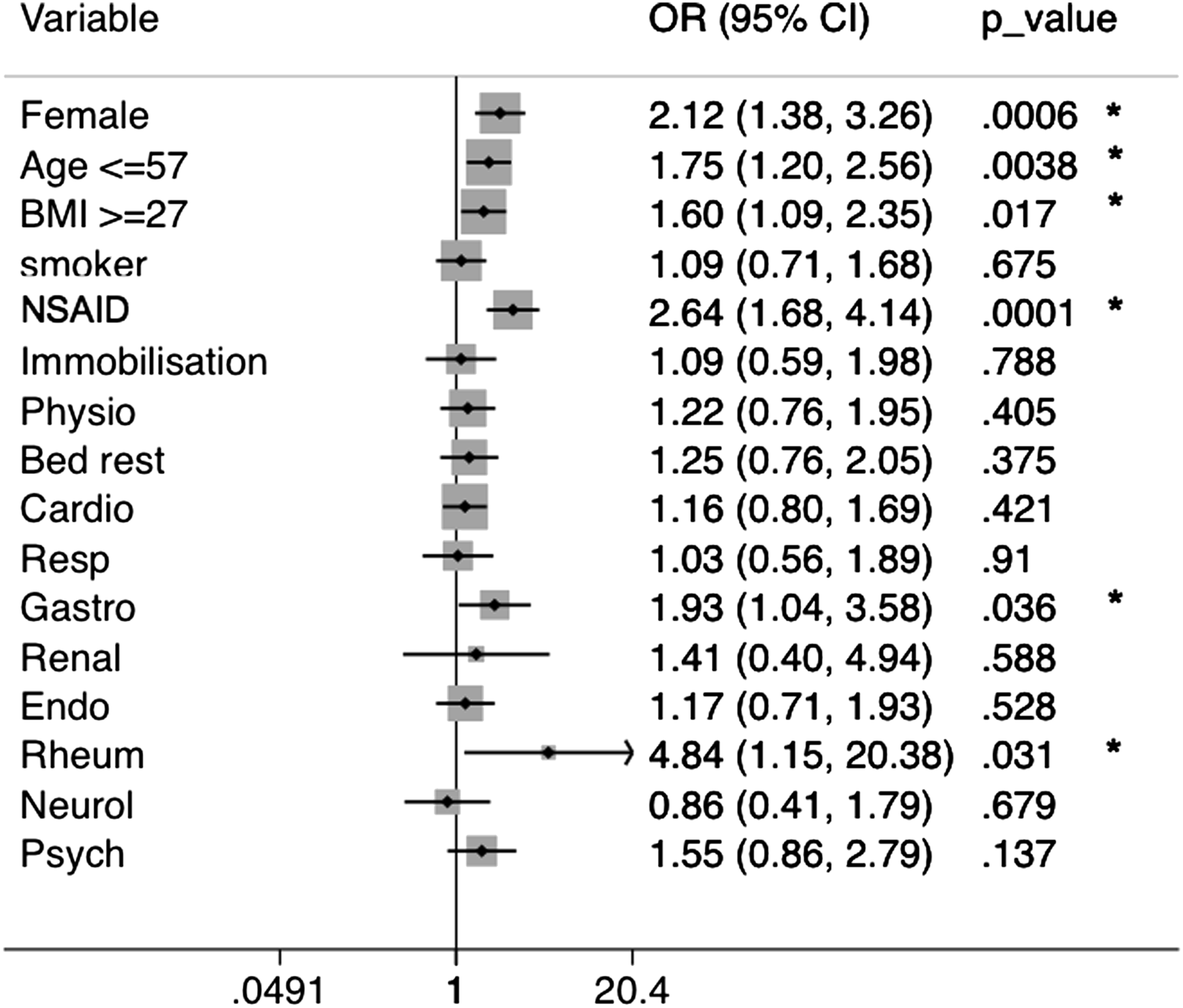
Forest plot of risk factors associated with neck pain.
Female gender (OR 2.12, CI 1.38-3.26, P = .0006), BMI ≥27 kg/m2 (OR 1.6, CI 1.08-2.33, P = .017), and age <57 years (OR 1.75, CI 1.2-2.56, P = .0038) were significantly associated with the presence of preoperative neck pain. Smoking status (OR 1.09, CI 7.1-1.68, P = .675), mJOA (OR 1.00, 95% CI 0.94-1.07, P = .980), age (OR .98, 95% CI 0.97-.99, P = .037), and duration of symptoms (OR 1.00, 95% CI 0.99-1.01, P = .572) were not predictors of neck pain.
Patients with gastrointestinal (OR 1.93, 1.04-3.57, P = .036) and rheumatologic comorbidities (OR 4.84, CI 1.15-20.4, P = .031) were also more likely to have neck pain. All other co-morbidities were not associated with the presence of pain, including respiratory (OR 1.03, CI 0.56-1.88, P = .91), renal (OR 1.41, CI 0.40-4.91, P = .588), endocrine (OR 1.17, CI 0.71-1.93, P = .528), neurological (OR .86, CI 0.41-1.78, P = .679) or psychiatric disorders (OR 1.55, .86-2.79, P = .137).
Preoperative immobilisation in a soft collar (OR 1.08, CI 0.59-1.97, P = .788), physiotherapy treatment (OR 1.22, .76-1.95, P = .405) or bed rest (OR 1.25, CI 0.76-2.05, P = .375) did not affect pain status. In contrast, patients with neck pain were more likely treated with NSAID medications at the time of assessment (OR 2.64, CI 1.68-4.13, P < .0001).
The cause of cervical canal stenosis was not significantly associated with the presence of pain. Specifically, patients were not likely to have more pain if they had spondylosis (OR .96, CI 0.59-1.55, P = .884), cervical disc degeneration (OR .97, CI 0.64-1.46, P = .877), ossification of the posterior longitudinal ligament (OR 1.21, CI 0.74-1.95, P = .439), hypertrophic ligamentum flavum (OR .89, CI 0.58-1.37, P = .613), congenital stenosis (OR 2.43, CI 0.78-7.57, P = .123) or subluxation (OR 1.42, CI 0.58-3.48, P = .437). The number of stenotic levels was not associated with the presence of neck pain (OR 1.02, 95% CI 0.88-1.18, P = .826).
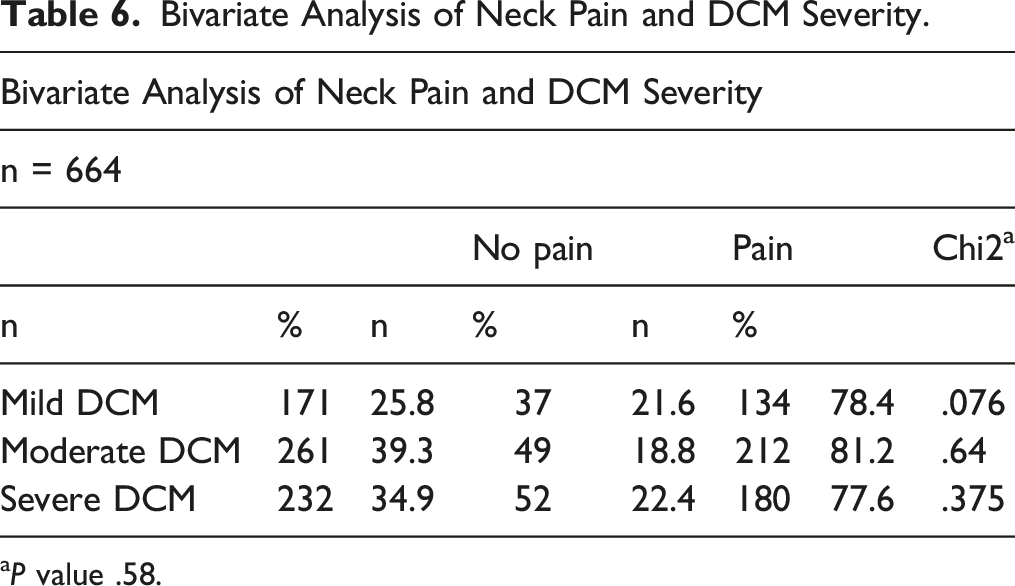
Bivariate Analysis of Neck Pain and DCM Severity.
aP value .58.
The presence of neck pain was independent of the severity of DCM (P = .58). Specifically, patients with mild DCM experienced neck pain in 78.4% (n = 134) of cases, whereas individuals with moderate or severe DCM described neck pain in 81.2% (n = 212), and 77.6% (n = 180) of cases, respectively.
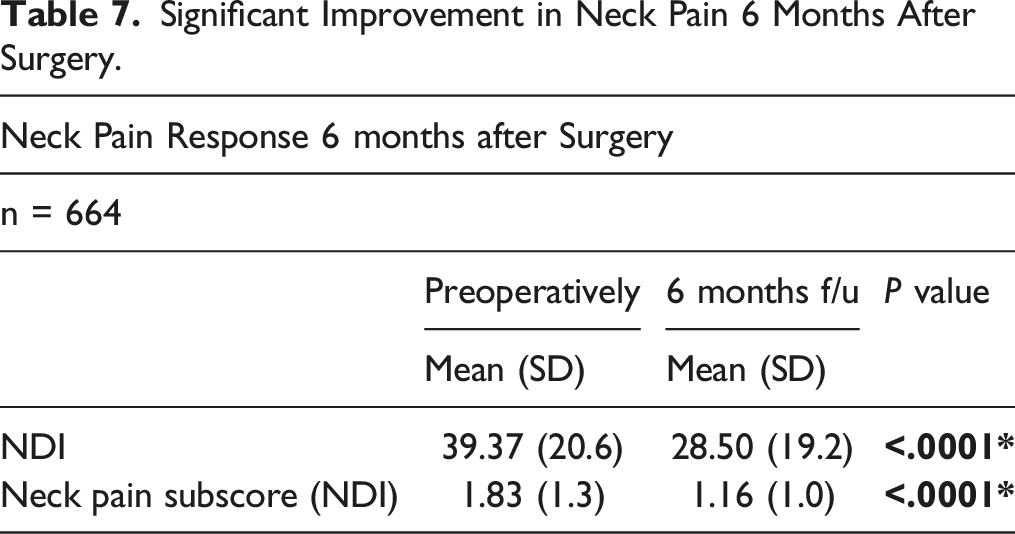
Neck Pain Response Six Months Postoperatively
Significant Improvement in Neck Pain 6 Months After Surgery.
Subgroup Analysis by Surgical Approach.

Discussion
The present study represents the first multicenter, international analysis examining the prevalence of neck pain, associated factors and the short-term response to surgery in patients with DCM. With this ambispective evaluation of 664 individuals from 26 global sites, we demonstrated a high prevalence of neck pain in almost 80% of individuals with DCM. Furthermore, we were able to identify associated factors of neck pain and found a significant response of neck pain to surgical intervention. This work is particularly important given emerging evidence indicating that patients with DCM rate neck pain as the most important symptom they experience. 25
Female patients were more likely to report neck pain than males. Previous studies showed a similar finding in females with low back and leg pain, whereas female patients tended to present with a more advanced disease state at the time of assessment.26,27 In contrast, we could not observe a gender difference in the duration of DCM symptoms. In general, chronic pain conditions were reported to be higher in the female population, 28 and neck pain has previously been described to occur more frequently in women.29-31 However, a gender difference in pain has not been reported in patients with DCM before.
Individuals at the age of 57 years or younger presented with more severe neck pain. This finding has not been demonstrated in patients with DCM previously. It might reflect a more advanced stage of cervical spondylosis with a concomitant effect of a reduced range-of-motion in the elderly patient population, resulting in less neck pain.
Smoking status was not associated with more neck pain in our patient population. In contrast to this finding in patients with DCM, in the general population smokers were shown to suffer more frequently from neck pain than non-smokers. 28 In terms of functional improvement after surgery in patients with DCM, non-smoking status was previously reported to be associated with better functional outcomes.12,29
Patients presenting with a BMI of 27 kg/m2 or higher preoperatively were more likely to have neck pain. This finding is consistent with previous results from Wilson et al, 32 demonstrating an association between a higher BMI and increased disability 1 year postoperatively in patients with DCM. In a healthy population of middle-aged individuals, the same association of BMI and neck pain has been demonstrated, based on a large prospective study. 31
Neck pain was associated with gastrointestinal comorbidities. This fact might be related to side effects from long-term NSAID use. As our patient questionnaire did not include the duration of NSAID intake, we could not evaluate this effect for our cohort. However, Machado et al 33 demonstrated an increased risk of gastrointestinal reactions by 2.5 times in patients taking NSAID’s due to spinal pain. Therefore, our findings implicate the need for further evaluation of potential side effects of NSAID’s in this patient population with a high pain prevalence.
The cervical spine has been shown to be involved in up to 80% of patients with rheumatoid arthritis (RA).2,33 Furthermore, it is known that DCM occurs in 5% of patients with RA.2,34,35 Therefore, our finding of an association between neck pain and rheumatological comorbidities seems to be consistent with this evidence.
None of the radiologically assessed sources of the cervical stenosis, such as disc herniation or spondylosis, was associated with more neck pain. Similarly, in a review recently published by Hill et al, 36 no associations between MRI findings and outcomes of neck pain could be identified. In the future, more advanced imaging techniques, especially in the field of microstructural MRI, might close this knowledge gap.
The response of neck pain to surgery has only been evaluated in a handful of studies so far and they are limited by generalized pain scoring systems, such as the Visual Analog Scale, and a small number of patients.14-16 However, we demonstrated a high prevalence of neck pain preoperatively and also a significant reduction in neck pain 6-months after surgery. Therefore, the role of surgery in improving neck pain might be a reasonable treatment option in the future. Surgical intervention in patients with severe neck pain might play a more important role, as we could not establish an effect of preoperative conservative treatments such as physiotherapy, immobilization in a soft collar or bed rest, on neck pain.
Strengths and Limitations
The large size of our patient cohort allowed for 99.8% power to detect a change in the neck disability index. The multicenter and global study-design not only allowed the collection of this large patient cohort, but also provides a good basis for a subsequent generalization of our findings. Adopting the neck disability index for this patient cohort allowed for a detailed analysis of neck pain in patients with DCM for the first time. Furthermore, the extensive preoperative data collection allowed for the evaluation of various associated factors of neck pain.
The study is somewhat limited by the lack of a non-operatively treated comparison cohort, but as surgical intervention has been shown to be superior to non-operative treatment in patients with moderate and severe DCM, such a study-design might prove challenging to implement. Nonetheless, it is recognized that evaluation of the role of nonoperative management in DCM has been relatively unexplored and is an area of clinical investigation which needs to be addressed. 37 We also acknowledge that capturing outcomes at 6 weeks, 3 months and then 6 months would have allowed us to have a more comprehensive understanding of how such outcomes evolve over time.
Conclusion
Footnotes
Acknowledgments
The authors thank and acknowledge the patients, researchers, and participating study sites. MM was supported by the Swiss National Science Foundation (SNF) and the Balgrist Foundation, Switzerland. MGF would like to acknowledge support from the Robert Campeau Family Foundation/Dr. C.H. Tator Chair in Brain and Spinal Cord Research at UHN as well as the DeZwirek Family Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
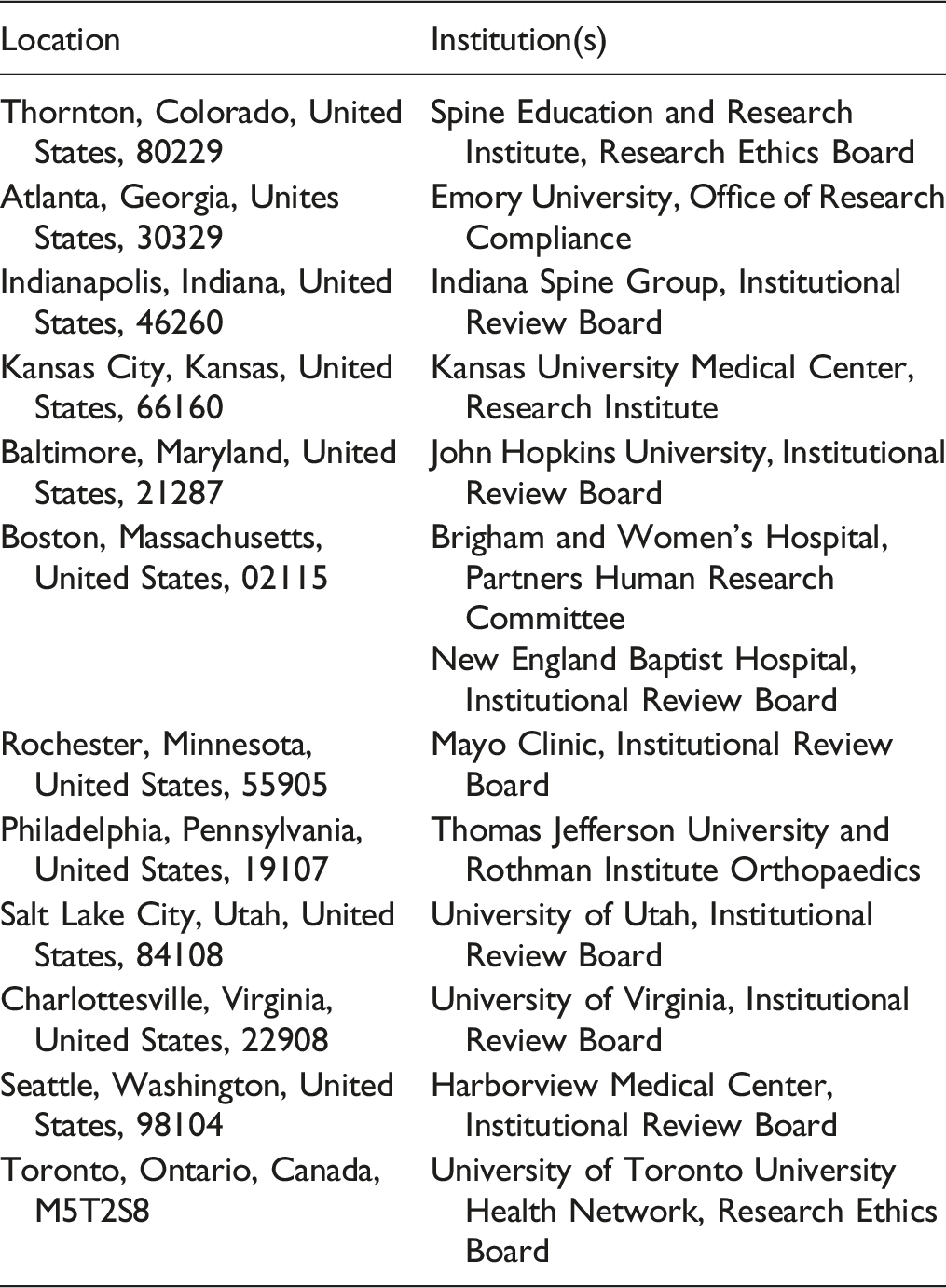
This work has not been presented previously. This was a post-hoc analysis of a dataset that combined the AOSpine CSM North America (CSM-NA; ClinicialTrials.gov NCT00285337) and AOSpine CSM International (CSM-I; ![]() NCT00565734) studies. These were single-armed, prospective, multi-center cohort studies conducted at 26 global sites that aimed to evaluate the efficacy of surgical decompression in patients with DCM with regard to functional status, disability, and quality-of-life (QOL) outcomes. Individual institutional review boards involved in NCT00285337, NCT00565734 clinical trials are shown above.
NCT00565734) studies. These were single-armed, prospective, multi-center cohort studies conducted at 26 global sites that aimed to evaluate the efficacy of surgical decompression in patients with DCM with regard to functional status, disability, and quality-of-life (QOL) outcomes. Individual institutional review boards involved in NCT00285337, NCT00565734 clinical trials are shown above.
Ethical Approval
Approval for the study was obtained from the University Health Network Research Ethics Board (07-0763.18) and the study was conducted in accordance with ethics guidelines.