
Abstract
Purpose
To evaluate the vertebral bone mineral density and the value of stand-alone oblique lumbar interbody fusion (SA OLIF) for the management of single-level adjacent segment disease (ASD) and primary lumbar degenerative diseases.
Patients and methods
Seventy-eight patients undergoing single-level SA OLIF was divided into index surgery group (n = 36) or revision surgery group (n = 42) at single center. The vertebral body Hounsfield units (HU) value was measured to assess bone mineral density of operated level by the preoperative CT. The following data were retrospectively collected and compared between the two groups: demographic, surgical data, clinical results, and complications.
Results
No differences were found between the two groups in surgical data. The fusion segment HU values in the revision group were significantly higher than that in the index group (147.4 ± 35.3 vs 129.2 ± 38.4 p = .033). There were significant differences while comparing fusion segment HU values to L1–L4 horizontal plane (147.4 ± 35.3 vs 126.1 ± 28.4, p = .000) and L1 (147.4 ± 35.3 vs 126.8 ± 26.2, p = .000) in revision group, meanwhile, no statistically significant difference was observed in index group (p > .05). The cage subsidence was observed in the revision group (n = 2) and index group (n = 9) (p = .045). The patients with cage subsidence had significantly lower vertebral HU values.
Conclusion
SA OLIF is valid alternative to the traditional posterior approach in the management of ASD with good clinical outcomes at short-term follow-up. Increased HU values of fusion segment may play a role in the management of ASD by SA OLIF.
Keywords
Introduction
Instrumented lumbar fusion approaches provide a good adjunct to stabilizing motion segments following surgery for lumbar degenerative conditions. However, spinal fusion increases the stress on the adjacent motion segments and puts the patients at risk for developing adjacent segment disease (ASD).1–3 The incidence of ASD following previous lumbar arthrodesis has been widely reported in the literature from 0 to 100%. 4 Zhang et al. 5 reported that the incidence of adjacent segment degeneration was 5.9% and rates of revision surgery for ASD was 1.8% per year according to their systematic review and meta-analysis. Revision surgery for ASD through a traditionally posterior approach can results in some improvement of symptoms and functional status. However, it is often associated with significant morbidity and can be technically demanding.6,7 Many challenges exist due to scarring, laminectomy defects, retained hardware, and increased risks of various surgical morbidities. These include devitalizing the paraspinous musculature, incidental durotomies, neurologic injuries, wound infections, and ASD recurrence. 8 In recent years, the minimally invasive retroperitoneal lateral lumbar interbody fusion (LLIF) approach has become an effective surgical option for arthrodesis in the lumbar spine. This technique is also alternative for the treatment of ASD, while decreasing risk of complications associated with direct dissection through the spinal canal. 9 Oblique lumbar interbody fusion (OLIF), unlike the transpsoas and transforaminal techniques, is the proposed solution to the approach-related disadvantages of LLIF technique. It can be used as a stand-alone procedure to manage isolated degenerative disc diseases, or spondylolisthesis.10–12 A few author reported short-term good outcomes of stand-alone OLIF (SA OLIF) for ASD with shorter operative time and hospital stay, lesser blood loss, and lower risk of dural injury comparing with posterior reoperation.13,14
Cage subsidence is a potentially devastating complication after SA OLIF procedures. Several potential risk factors have been examined in the literature including bone quality, over distraction, insufficient cage width, construct length, lateral plating, and endplate injury.15,16 Dual-energy X-ray absorptiometry (DXA) is widely used clinically to diagnosis osteoporosis and represents the current gold-standard for bone mineral density (BMD) assessment. However, various limitations of DXA have been described such as distortion of estimated bone mass values caused by overlying soft tissue, vascular calcifications, spinal degenerative changes, pedicle screw instrumentation especially occurred in the patients who underwent posterior lumbar fusion. Hounsfield units (HU), as measured on routine CT of the lumbar spine, have shown promise in predicting bone density and various complications in patients with a degenerative lumbar spine.17–19 Bone mineral density measurement by HU as a predictor for cage subsidence should be included in the preoperative planning for spine surgeons to determine whether or not SA OLIF will be performed to treat the patients with ASD. To date, few studies have attempted to assess vertebral BMD and cage subsidence associated with SA OLIF for the treatment of ASD following posterior lumbar fusion. The purpose of this study was to compare SA OLIF as revision for ASD with index surgery for degenerative lumbar diseases, and to assess the effect of vertebral bone mineral density on the cage subsidence.
Material and methods
Patient data
The approval of our institutional review board was obtained. A retrospective study of patients who underwent single-level SA OLIF at our institution between January 2015 and May 2020 were reviewed. Clinical and radiological measurements were collected and analyzed immediately postoperatively and at 3, 12 and last follow-up after surgery. All patients were followed up 13–44 months, with an average of 26.4 ± 8.4 months. Thirty six patients in revision surgery group were enrolled according to the following criteria: (1) patients had a previous PLIF or TLIF surgery; (2) diagnoses included single-level lumbar instability, lumbar disc herniation and spinal stenosis. Forty two patents in index surgery group included grade 1° degenerative spondylolisthesis, lumbar instability or stenosis. The exclusion criteria for the study were as follows: (1) lumbar spondylolysis; (2) lumbar spondylolisthesis grade >1°; (3) spinal tumor pathologies; (4) spinal infection; (5) spinal trauma; (6) diseases involving the L5–S1 vertebrae. The contraindications for SA OLIF were moderate/severe neurological deficits (We defined the patients who appeared to have decreased muscle strength or reduced sensation of legs as moderate/severe neurological deficits), large disc herniation or protrusion (Large disc herniation was defined in patients when their herniated intervertebral disc accounted for 50% or more of the spinal canal), Grade C spinal stenosis or worse (Schizas et al.
20
made a definition for grade C stenosis—no rootlets can be recognized, the dural sac demonstrating a homogeneous gray signal with no cerebrospinal fluid signal visible and there is epidural fat present posteriorly according to magnetic resonance imaging (MRI)), anatomic limitation between psoas and major vessels. All of patients presented low back pain as their predominant complaint, with varying degrees of radiating pain, intermittent claudication, or a combination of these. All patients had to have been treated conservatively for at least 6 weeks without success before consideration for surgical intervention. All patients included had preoperative evaluation with detailed neurologic examination and radiologic imaging, which involved static (anterior–posterior and lateral) and dynamic (flexion and extension) plain lumbar radiographs (Figure 1), magnetic resonance imaging (MRI), and computed tomography (CT) scans. Demographic, surgical data, clinical results, complication, and radiological data were retrospectively collected and assessed. A: X-ray films of a 55-year-old male patient who underwent SA OLIF for rostral adjacent segment disease; A1, A2. Preoperative anteroposterior and lateral views; A3, A4. Preoperative lumbar dynamic position views; A5, A6. No Cage subsidence was found at 6 months after SA OLIF. B: X-ray films of a 67-year-old female patient with L4 spondylolisthesis (Meyerding type Ⅰ) in index group. B1, B2. Preoperative anteroposterior and lateral views; B3, B4. Preoperative lumbar dynamic position views; B5, B6. Cage subsidence was found at 6 months after SA OLIF.
HU value measure
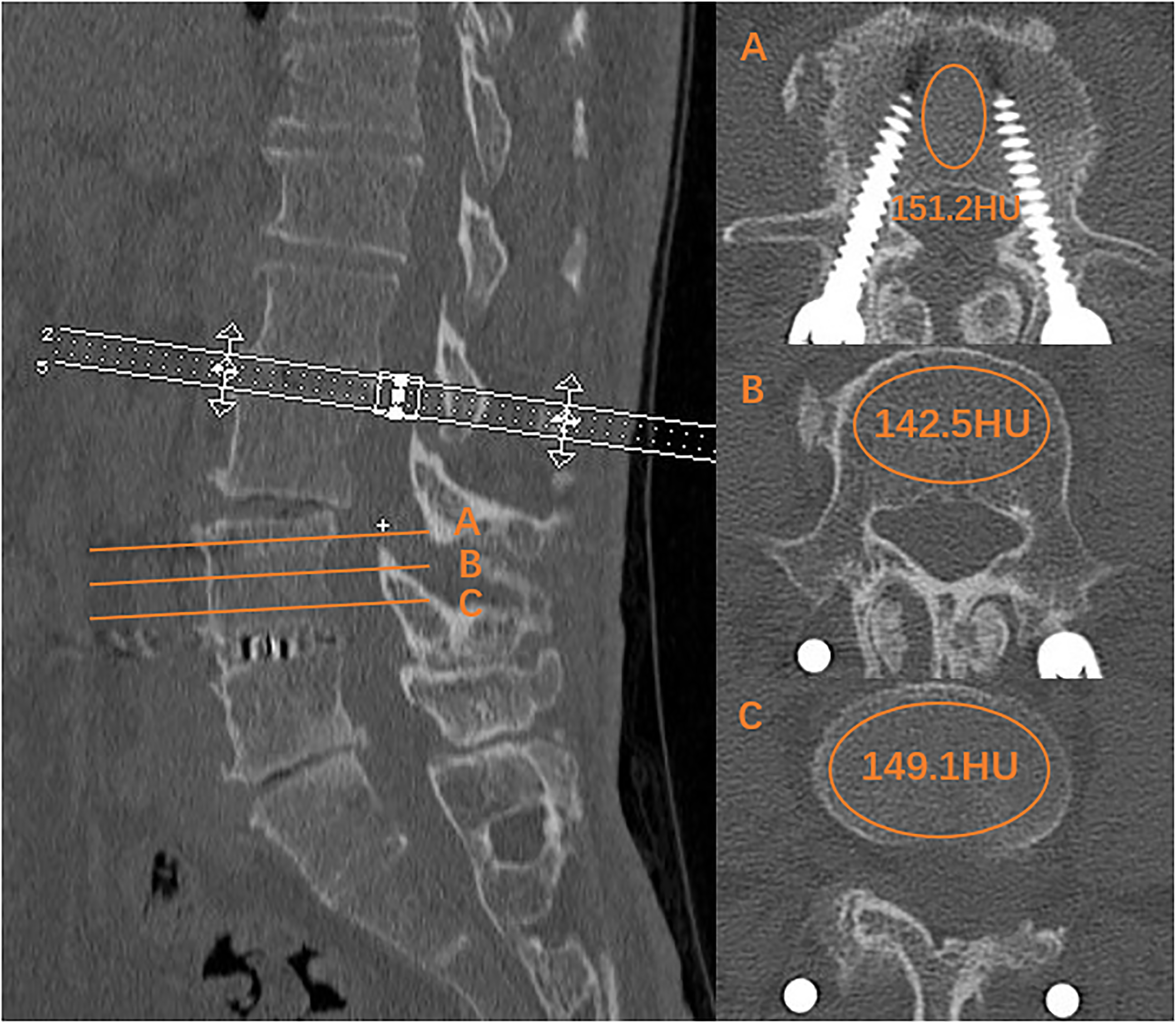
Computed tomography scanner (SOMATOM Definition Flash, Siemens Healthineers, Forchheim, Germany) was utilized for all patients. Computed tomography parameters included a slice thickness of 1.25 mm with a 0.625 mm interval and a tube voltage of 120 kV. The preoperative CT was routinely used to calculate HU values. Vertebral body HU values were measured according to the technique described by Schreiber.
17
Using standard picture archiving and communication system (PACS) software, an elliptical area of interest (AOI) was drawn on an axial image of lumbar vertebral body including the largest possible cancellous bone and excluding cortical edges, osteophytes, osseous abnormalities, and voids. Special attention was paid not to let the AOI include prior pedicle screw instrumentation on the ASD level. Three measurements were obtained: just superior to the inferior endplate, mid-vertebral body, and just inferior to the superior endplate (Figure 2, Figure 3). The picture system calculates the HU value of the area within the ellipse. The vertebral body BMD was defined as the average HU value of the three AOIs. L1–L4 vertebral body HU, L1 HU, and HU value on fusion segment undergoing SA OLIF were measured and recorded respectively. L1–L4 vertebral HU was defined as the mean value of the four HU values from L1 to L4 vertebra. Fusion segment HU was defined as the mean value of the upper and lower vertebra experiencing SA OLIF. The regions were excluded from the AOI if apparent sclerotic areas which might result in inaccurate measurement of trabecular HU in the vertebral body. One major challenge of endplate CT assessments is the reproducibility of measurements because the methodology is not as standardized compared to routine assessments. So, vertebral body HU values on horizontal plane were measured and assessed in this series. T-values as bone mineral density were measured by dual-energy X-ray absorptiometry on the basis of routine methods. Application of the preoperative CT plus PACS system to measure the HU values of the lumbar spine in index group. Application of the preoperative CT plus PACS system to measure the HU values of the lumbar spine in revision group.
Surgical technique
Stand-alone OLIF
All patients underwent OLIF only through left side approach without neurophysiologic monitoring. The procedure was performed utilizing expandable retractors (OLIF 25 system; Medtronic, Memphis, TN, USA) according to the procedure described previously. 12 Polyetheretherketone (PEEK) intervertebral cages (OLIF25 Clydesdale Spinal System; Medtronic SofamorDanek, Minneapolis, MN, USA), filled with allograft bone, were used to achieve fusion. No direct posterior decompression and instrumentation were done in this series.
Clinical and radiographic measures
The clinical parameters including Operative time, radiation exposure time, Intraoperative blood loss, and length of hospital stay were collected. All intraoperative and postoperative complications, including vertebral endplate fracture, leg sensory disturbance, psoas/quadriceps weakness, sympathetic nerve injury, surgical site infection, dural tear, ureteral injury, vascular injury, peritoneal content injury, hematomas, paralytic ileus, cage subsidence, and cage migration were also recorded and followed up.
Clinical outcome data included visual analogue scores (VAS) for back pain and Oswestry Disability Index (ODI). Back pain was quantified by visual analog scores (VAS) collected from the patients preoperatively and at final follow-up. The sex question (Section 8) is unacceptable in our culture, and most patients are reluctant to answer this section. Therefore, it was omitted from the ODI parameters in this study. The total possible score is 45. After discharge from the hospital, patients were followed up regularly by the corresponding author. Plain lumbar radiographs were ordered to assess interbody fusion. Computed tomography scan and/or MRI examinations were performed only if patient complained of radiculopathy and/or worsen back pain postoperatively or fusion was suspected to be suboptimal. Fusion was assessed by an independent radiologist using static and dynamic plain X-rays in last follow-up. Definitive fusion was identified by formation of continuous trabecular bony bridges along contiguous vertebral bodies at the operated levels, and less than 3° segmental movement (Figure 4). X-ray films of a 49 year-old female patient with SA OLIF at L4/5 at 6 months after operation. C1, C2. Postoperative anteroposterior and lateral views showed that there was formation of continuous trabecular bony bridges along contiguous vertebral bodies at the operated levels; C3, C4. Postoperative lumbar dynamic position views showed that less than 3° segmental movement was found.
Statistical analyses
The values are shown as mean ± SD. Statistical analyses performed using SPSS Version 23.0 (version 23, USA). p < .05 were accepted for significance. Shapiro–Wilk tests were used to verify the normal distribution of continuous variables. The independent sample t-tests were used for variables which followed normal distribution. The Mann–Whitney U-test was used for those not following normal distribution. Paired t-test was used for within-group statistics. Chi-squared test was used for categorical data.
Results
Comparison of demographic and clinical data between both groups.

There were no significant differences in age, sex, BMI, operated level, average of the lowest T-score, and average HU value between both groups (p > .05). In revision group, the fusion segment HU value was significantly higher than L1–L4 HU value (147.4 ± 35.3 vs 126.1 ± 28.4, p = .000) and L1 HU value (147.4 ± 35.3 vs 126.8 ± 26.2, p = .000). No difference was found among L1 (131.9 ± 38.3), L1–L4 HU value (128.6 ± 36.5) and fused segment HU value (129.2 ± 38.4) in index group. The fusion segment HU values in the revision group were significantly higher than that in the index group (147.4 ± 35.3 vs 129.2 ± 38.4 p = .033). The lower vertebrae of operated level in revision group has significantly higher HU value comparing to that in index group, meanwhile, no significant difference of HU value in upper vertebrae of operated level was found between both groups.
Surgical parameters and clinical outcomes between both groups.

Complications in 78 patients.

HU values between the patients with subsidence and non-subsidence.

Discussion
The treatment of ASD has typically been decompression and stabilization, or extension of the existing construct. In the setting of ASD with radiographic evidence of dynamic instability, spondylolisthesis, and/or stenosis, several studies report significant improvement in pain and quality of life after revision surgery. Traditional posterior revised surgery for ASD including TLIF, PLIF, and MIS TLIF consisted of aggressive decompression involving extensive removal of the medial facets and foraminotomies followed by extension of the previous fusion. The surgical treatment for ASD via conventional surgery often follows the previous approach. Additional posterior instrumentation has been suspected to result in more extensive dissection and blood loss, longer duration of operation, higher risk of surgical site infection and durotomy, and greater medical costs.
Oblique lumbar interbody fusion approach achieves indirect decompression and sagittal and coronal restoration via the insertion of larger interbody cage supporting bilateral epiphyseal rings. Compared with TLIF/PLIF, it may significantly reduce tissue trauma and blood loss, decrease the operating time, and preserve the posterior longitudinal ligament complex. In comparison to LLIF, this technique may also reduce risk related to the transpsoas approach, such as injuries to the psoas muscle, lateral femoral cutaneous nerve, genitofemoral nerve, and lumbosacral plexus. To date, few studies have investigated the clinical outcomes of SA OLIF for ASD, although OLIF has achieved popularity over the treatment of lumbar degenerative diseases. Compared with posterior reoperation, SA OLIF for ASD obtains good clinical and radiographic outcomes with decreased operative time and hospital stay, lesser blood loss, and lower risk of dural injury.13,14 There is no consensus regarding the efficacy of treatment with SA OLIF, although it seems to be advantageous in the setting of ASD. Considering indirect decompression of SA OLIF, it is very important to correctively determine indication for ASD. Lumbar instability in 21 cases, spinal stenosis in 11 cases, and disc herniation in 4 cases had been chosen as indication in our series. It is stressed that lumbar stenosis with soft compression is mild or moderate. No prolapse and massive herniation are chosen as indication for SA OLIF. There was no significantly difference between the two groups in operative time, intraoperative blood loss, and X-ray exposure since all of the patients underwent the similar procedure. Functional scores including ODI and VAS for back pain significantly improved after surgery, which demonstrated early clinical results in 78 cases. SA OLIF may provide good short-term outcomes for the patients with ASD.
The leg sensory disturbance was observed in seven cases followed by psoas/quadriceps weakness in three cases, all of which disappeared within 2 month after conservative therapy. The reason for transient sensory disturbance and weakness was considered to be associated with psoas muscle isthmic condition and nerve irritation. Endplate fracture occurred in one case in revision group and 3 cases in index group respectively during procedure. Cage subsidence was observed in 2 cases in revision group and 9 cases in index group, which resulted in interbody fusion in final follow-up. Cage subsidence is one of the most common complications that can be seen with OLIF, which may be correlated with intraoperative endplate damage, endplate strength, osteoporosis and so on. The patients with cage subsidence may suffer from axial pain and recurrent neurological symptoms, although SA OLIF may be as effective as OLIF aided by different fixation devices with less blood loss, shorter operative time, and lower operative cost for implants. Lower BMD have been previously tied to higher rates of postoperative interbody cage subsidence in patients undergoing OLIF. Osteoporosis may play more important role in occurrence of cage subsidence during SA OLIF while comparing with cage size. For the reason, accurate preoperative assessment of a patient’s underlying bone quality is paramount for OLIF, especially SA OLIF.
Dual-energy X-ray absorptiometry (DXA) is current “gold method” to assess BMD and is widely used clinically to diagnosis osteopenia or osteoporosis. However, a growing body of research literature has suggested that in vivo assessments of BMD using DXA are inaccurate and imperfect. Alternative means of preoperative bone quality assessment have been investigated for patients being considered for spinal fusion.21,22 Since 2011, the vertebral Hounsfield units (HU) value derived from clinical computed tomography (CT) has been regarded as a useful tool to determine BMD and osteoporosis. 17 It is less affected by lumbar degenerative conditions than DXA by avoiding cortical bone, vascular calcification, and degenerative structures. Considering lumbar CT is a routine preoperative examination for patients requiring lumbar fusion, the HU value can be measured on preexisting CT images at no additional cost and radiation. One advantage of a CT-based technique over the DXA is that CT-based techniques can selectively measure detailed site-specific bone density, such as the pedicles and endplates. 23 DXA scans and associated t-scores have a suboptimal predictive value for osteoporotic related complications following elective spine surgery. While both lower t-scores and average HU were associated with osteoporosis related complications, only HU was an independent predictor of osteoporosis related complications. 24 HU, as measured on routine CT of the lumbar spine, have shown promise in predicting various complications in patients with a degenerative lumbar spine. 25
To the best of our knowledge, few studies have assessed the specific relationship between the vertebral body HU and interbody graft failure during SA OLIF for ASD. It is worth evaluating the influence of BMD in ASD level on the risk of cage subsidence, since no additional instrumentation may obviously increase the risk of cage subsidence and migration during SA OLIF procedure. Unfortunately, unlike DXA t-scores, which have universally recognized scoring stratification, accepted standard cut-off values for HU have not yet been determined. Some authors have suggested cut-offs between HU < 110–160 as predictive of clinically significant diminished bone density in the lumbar spine. Using 110 HU as the lower limit of normal provides 52–60% sensitivity for distinguishing osteoporosis from osteopenia and normal BMD in the lumbar region.26,27
To date, few literatures reported the study on cage subsidence after SA OLIF. According to a systematic review, of those studies that specified subsidence rate, the pooled patient populated equaled 1362 patients, 141 of whom incurred cage settling after LLIF. Therefore, the estimated incidence of subsidence reached 10.3%. 28 The present study demonstrates that there was a relatively low rate of cage subsidence (14.1%) in 78 patients, as compared to that (18.7%) reported by Abe et al. 29 The cage subsidence rate was 5.6% in revision group, which was significantly lower than subsidence rate of 21.4% in index group. The average HU values of fusion segment and lower vertebra in the revision group was significantly higher than those in the index group, which was reason why lower incidence of cage subsidence was observed in revision group. There were statistically significant lower vertebral body HU values in 11 patients with subsidence while comparing to 67 patients without subsidence (Table 4). Our findings suggest that a significant association exists between lower HU values of lumbar vertebral body and the likelihood of cage subsidence after SA OLIF for ASD. Therefore, we recommend routinely measuring the HU value on preoperative CT scans when planning SA OLIF for ASD. Vertebral osteoporosis should been considered as contraindication for SA OLIF as primary or revision surgery.
No significant difference was found among L1, L1–L4 and fusion level HU values in index group. Nevertheless, vertebral HU value on fusion level was significantly higher than those on L1 HU value (147.4 ± 35.3 vs 126.8 ± 26.2, p = .000) and L1–L4 HU value (147.4 ± 35.3 vs 126.1 ± 28.4, p = .000) in revision group. It is speculated that additional stress over adjacent segment following lumbar arthrodesis may result in degenerative diseases and increased bone mineral density. The higher BMD is in favour of preventing cage subsidence following SA OLIF for ASD, although the true etiology of increased bone mineral density remains unknown.
The patient population was relatively heterogeneous with regard to surgical indication, which included lumbar spondylolisthesis, instability, stenosis, and disc herniation. Stand-alone oblique lumbar interbody fusion was performed as index and revision procedures. There were other limitations such as relatively small sample size, short time follow-up, and the retrospective nature of this study. Cage subsidence was measured with postoperative lateral lumbar radiographs but CT scans. Additionally, we were not able to assess the relationship between cage subsidence and vertebral BMD, since the number of patients with cage subsidence was too small.
Conclusion
In conclusion, SA OLIF provides good clinical outcomes in the management of ASD and primary lumbar degenerative diseases at short-term follow-up. The HU values of fusion segment were significantly higher than those including L1–L4 and L1 in the patients with ASD, although the true etiology of increased bone mineral density remains unknown. Stand-alone OLIF has advantages that make it attractive comparing to the traditional posterior procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The clinical study proposal was approved by the medical ethical committee of the authors’ institution. The written informed consents were obtained from all patients at study entry.