
Abstract
Study Design
A retrospective study.
Objectives
This study aimed to check how accurately cages were inserted and how they affected the radiological results in oblique lumbar interbody fusion (OLIF) at L2-L5.
Methods
A total of 137 patients diagnosed with lumbar degenerative disease, 184 intervertebral discs were included. We used a new cage deviation classification system on magnetic resonance imaging (MRI) to determine cage insertion accuracy. Cage deviation angles (CDA) were classified into four groups based on the angle formed by the long axis of the cage and the horizontal axis of the vertebral body. Other radiological parameters on plain radiographs and MRI were compared based on this classification.
Results
Among 183 cages, 19 were in zone Ⅰ-Ⅱ (10.32%), 163 were in zone II-III (88.59%), and two were in zone III-IV (1.09%). The median cage deviation was 4.97°. No significant differences (H = 2.479, P = .290 > .05) of CDA were found among different segments. Posterior cage deviation accounted 94.57%. The minimal, mild, moderate, and severe cage deviation was 89 (48.4%), 51 (27.7%), 30 (16.3%), and 14 (7.6%) respectively. No differences in radiological parameter changes were noted among different cage obliquity categories.
Conclusions
Approximately 98.91% of cages were placed in zones I-II and II-III. Most cages deviated posteriorly with CDA ranging minimal to moderate. Minimal to moderate cage deviation did not impact radiological outcomes significantly in OLIF at L2-L5. However, avoiding severe cage deviation is crucial to prevent contralateral traversing nerve root injuries.
Introduction
Oblique lateral interbody fusion (OLIF) have gained popularity for treating spinal conditions like degenerative disc disease, spondylolisthesis, and spinal deformities.1-6 Placement of cage was the key step in OLIF which might have notable effects on radiological parameters. Placing the cage anteriorly can aid in restoring the segmental angle (SA), while posterior placement might facilitate achieving indirect decompression outcomes. 7
Achieving the accurate cage position is crucial for restoring sagittal alignment and prevents injury to contralateral traversing nerve roots. 8 Uribe 9 et al. categorized the lumbar vertebrae into four zones based on their sagittal position by anatomical study and suggested the cage should be placed within zones II and III, which were defined as the anatomical safe zones. How to put the cage in accurate position? Traditionally, direct lateral interbody fusion (DLIF), extreme lateral interbody fusion (XLIF), lateral lumbar interbody fusion (LLIF) have been performed with a direct lateral view, facilitating cage insertion under fluoroscopy. Conversely, the OLIF procedure employs an oblique trajectory.10,11 The orientation of intervertebral disc removal and cage implantation in OLIF needs to be rotated to align perpendicular to the vertebral body in the sagittal plane. This oblique angle can be somewhat disorienting for certain surgeons. 12 Given that the process of OLIF cage insertion can be perplexing for surgeons, navigation techniques have been utilized to mitigate this confusion in certain conditions.12,13
Although the safe zone of lateral retroperitoneal transpsoas approach had been mentioned, there were no reports about the accurate cage position of OLIF until now. Also, whether malposition or deviation of OLIF cage could achieve equivalent operation goals is still not known. In this study, we put forward a new cage deviation classification system to determine cage insertion accuracy in OLIF and focus on investigating the relationship between OLIF cage positioning and early post-operation radiographic changes.
Materials and Methods
Study Design
This study was approved by the Institutional Review Board of the Ethics Committee of Qingdao Municipal Hospital (No. 2023148). The participants provided written informed consent for the study and publication.
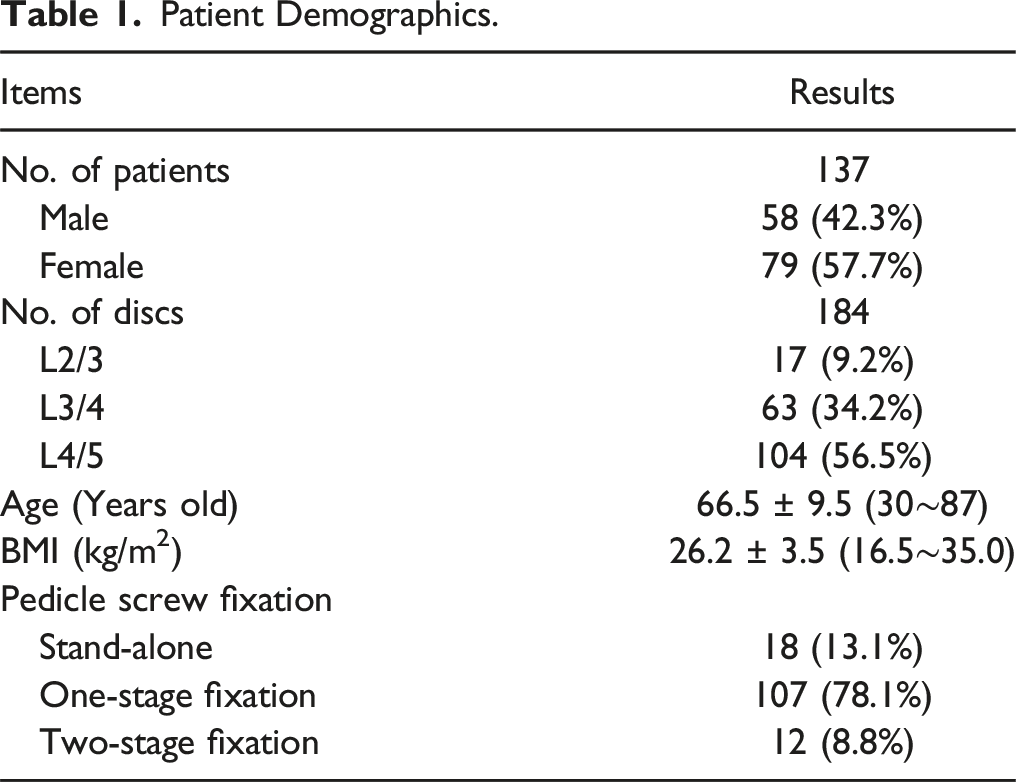
A total of 137 patients, comprising 58 (42.3%) males and 79 (57.7%) females, who underwent OLIF by a single surgeon at Qingdao Municipal Hospital, were enrolled in this study from April 2017 to April 2022. All patients were diagnosed with lumbar spinal stenosis, degenerative spondylolisthesis, or degenerative lumbar scoliosis. Exclusion criteria included: (1) a narrow corridor between the aorta and psoas, (2) history of abdominal surgery, and (3) surgical requirement for L5/S1 abnormalities. Basic demographic data, including gender, age, height, weight, time of chief complaint, and smoking history, were recorded.
Surgical Procedure
Preoperative plain radiographs, computerized tomography (CT) and magnetic resonance imaging (MRI) were performed. Particular attention was given to corridor between aorta and psoas, lateral osteophytes, disc space height, and facet joint degeneration level before operation was scheduled.
Patients were positioned in the lateral decubitus position. A skin mark was made at the center of the target intervertebral disc using C-arm fluoroscopy guidance. Access to the psoas was achieved through the retroperitoneal space after incision and dissection of abdominal muscles. Careful retraction of the psoas revealed the intervertebral disc. The intervertebral disc was removed, and endplate preparation was performed after a tubular retractor was placed. Dissection of the annulus fibrosis on the opposite side ensured the cage’s access to the contralateral apophyseal ring. An 18 mm-wide cage filled with allogenic bone was inserted into the intervertebral space, confirmed for proper size using a cage model. Posterior and lateral fluoroscopy were conducted to verify accurate cage placement on the bilateral apophyseal rings. Single-segment cases received posterior pedicle screw instrumentation through a Quadrant retractor, while two or more segment cases employed traditional open access.
Radiological Evaluation
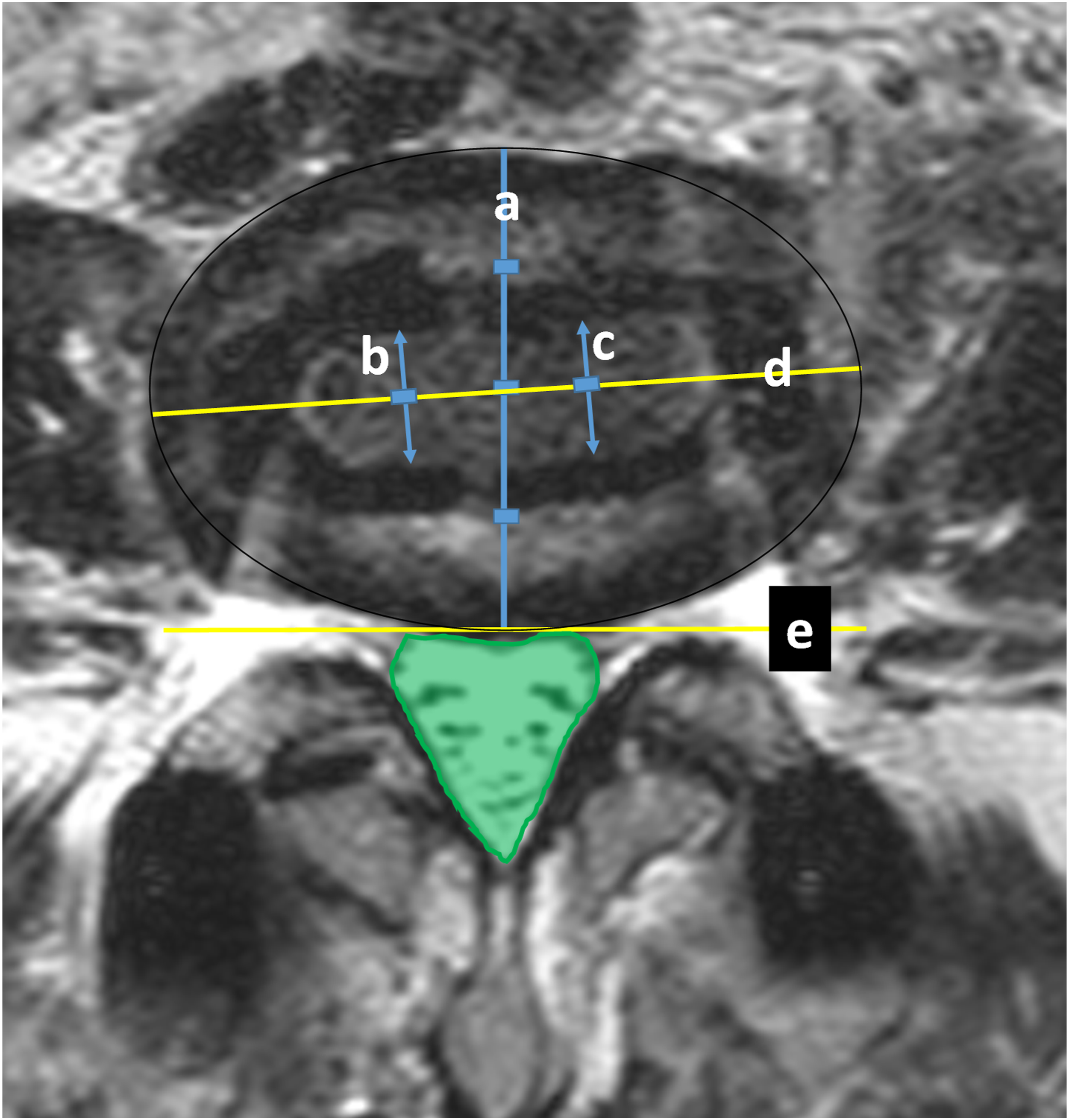
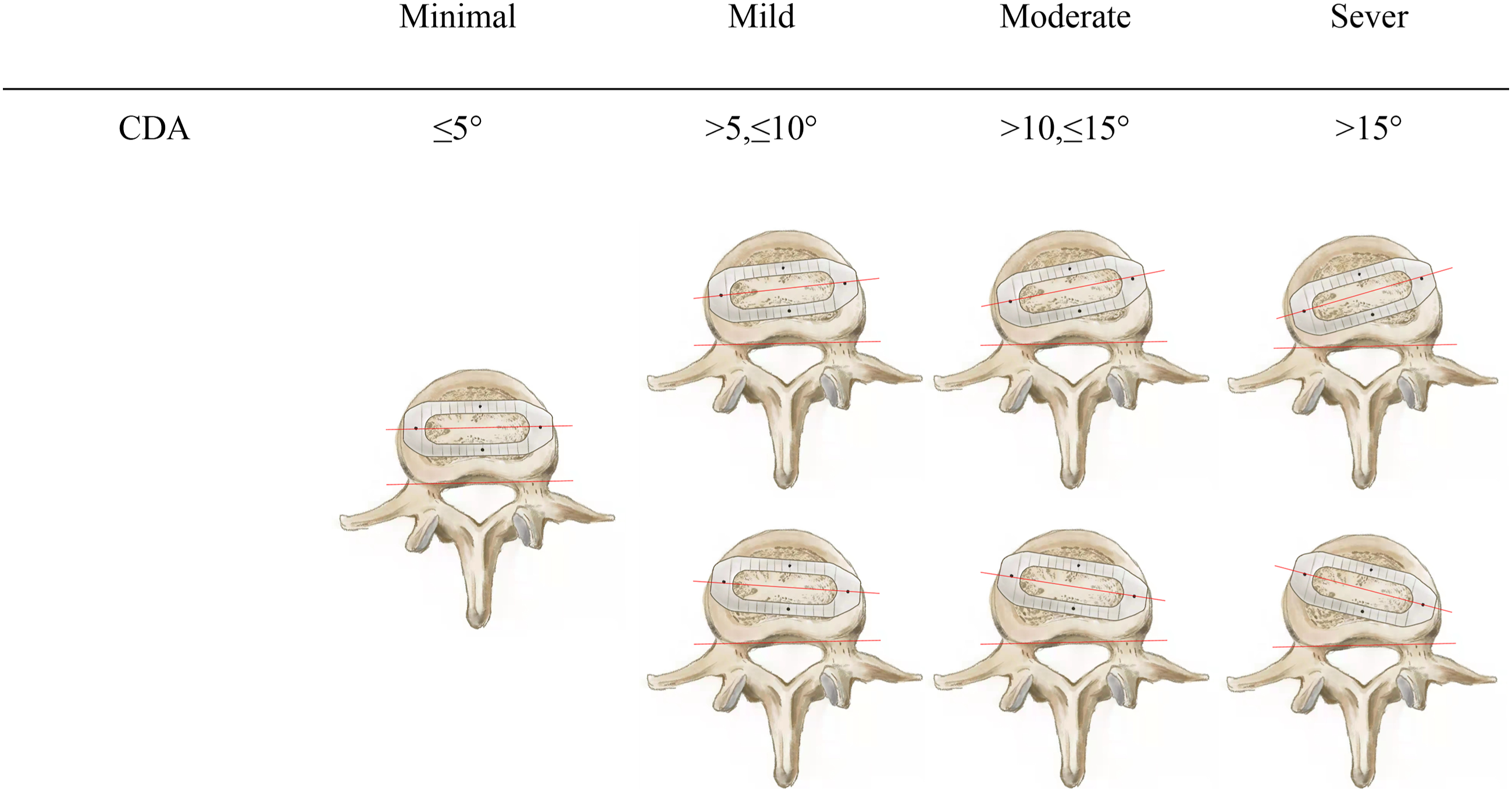
Our study primarily focuses on postoperative radiological changes. Each patient underwent plain radiographs and MRI within 1 week after the surgery. All measurements were independently collected by three physicians. Average results were used for statistical analysis. If unacceptable differences (>5° for degree, >5 mm for distance and >10 mm2 for area) existed, a fourth physician was involved to ensure reasonable results. Pre- and postoperative lateral plain radiographs were used to measure anterior disc height (ADH), posterior disc height (PDH), foraminal height (FH), foraminal area (FA), surgical segment angle (SSA), disc segment angle (DSA), and lumbar lordosis (LL) using our PACS (picture archiving and communication system) workstation. (See Figure 1) Additionally, the mean cross-sectional area of the thecal sac (CSA) was calculated from three distinct intervertebral levels on T2-weighted MRI, both before and after the operation. Postoperative MRI was employed to assess the position and angulation of the cage. (See Figure 2) The desired cage position was defined as having the main body within zone Ⅱ to Ⅲ. Cage angulation was categorized into four groups based on the angle formed by the long axis of the cage and the horizontal axis of the vertebral body: minimal (0°-5°), mild (>5° ≤ 10°), moderate (>10° ≤ 15°), and severe (>15°). (See Figure 3) Measurements on plain radiographs. Angulation between line a and b was disc segment angle. Line c and d was anterior disc height and posterior disc height. Line e was foraminal height. Angulation between line f and g was surgical segment angle. The green part represents foraminal area. Measurements on postoperative MRI. The outline of the disc was drawn as an oval. Line a was the central line of the oval and been seprated into four equal parts, representing zone Ⅰ ∼ IV, where cage position was defined. Line b and c were separated equally, then line d was the central axis of the cage. Angulation between line d and e represented cage obliquity. The green part represented cross-sectional area. Cage deviation angle on MRI was divided into two types: anterior and posterior deviation and four categories: minimal, mild, moderate and severe according to the angulation formed by long axis of cage and horizontal axis of vertebral body (the two red lines).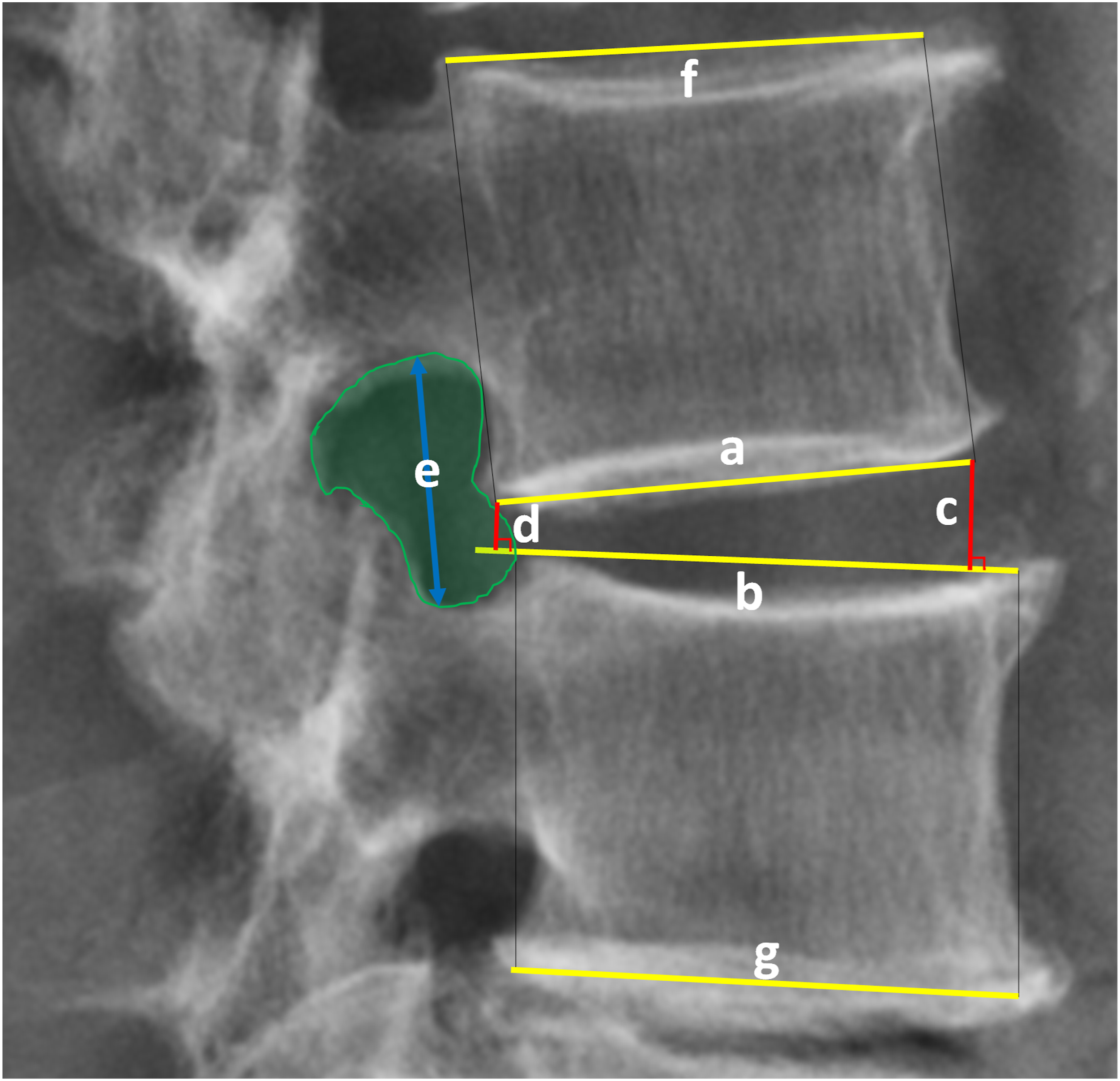
Statistical Analysis
Statistical results were presented as mean ± standard deviation for continuous variables and as frequency and percentage for categorical variables. We utilized paired Student t-tests to compare pre- and postoperative radiological parameters. Similar statistical approaches were used when patients were divided into subgroups based on different operation levels and diagnoses. The chi-squared test (χ2) was employed to compare the percentage of malpositioned cages in different segments. Kruskal-Wallis test and chi-squared test (χ2) were used to compare the degree of cage obliquity across different segments. Analysis of variance (ANOVA) was utilized to compare radiological parameter changes between various cage obliquity categories. Spearman correlation analysis was conducted to investigate the relationship between cage angulation and changes in radiological parameters. A significance level of P < .05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 19.0; IBM SPSS Statistics for Windows, IBM Corp, Armonk, NY).
Results
Patient Demographics.
Radiological Changes
Changes on Plain Radiographs and MRI.
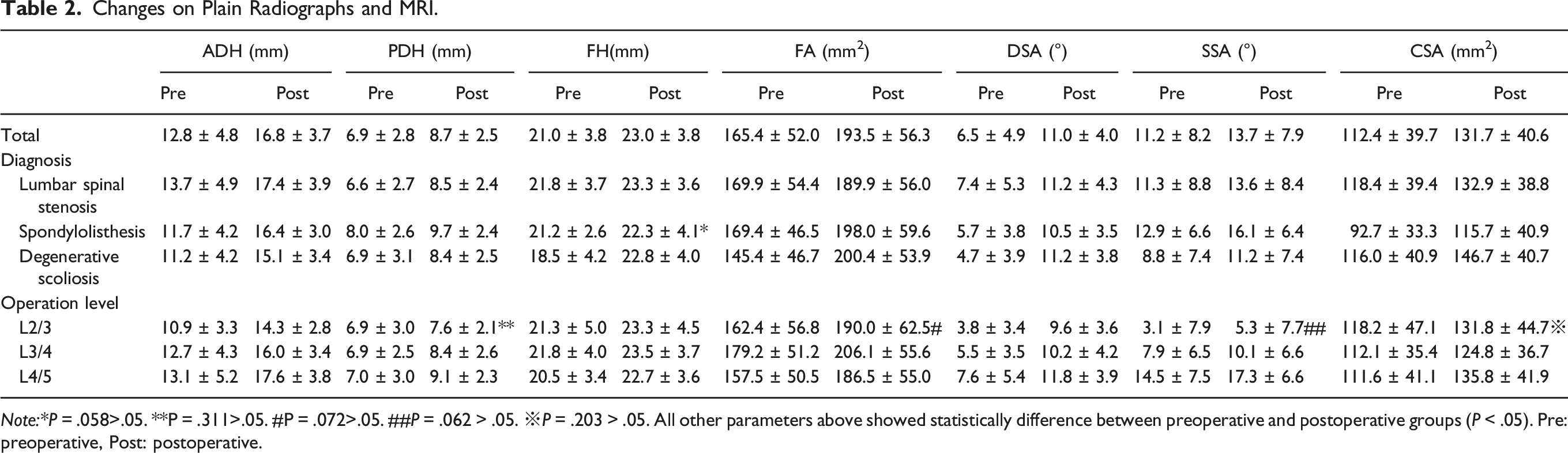
Note:*P = .058>.05. **P = .311>.05. #P = .072>.05. ##P = .062 > .05. ※P = .203 > .05. All other parameters above showed statistically difference between preoperative and postoperative groups (P < .05). Pre: preoperative, Post: postoperative.
LL Change in Different Operation Levels on Plain Radiographs.
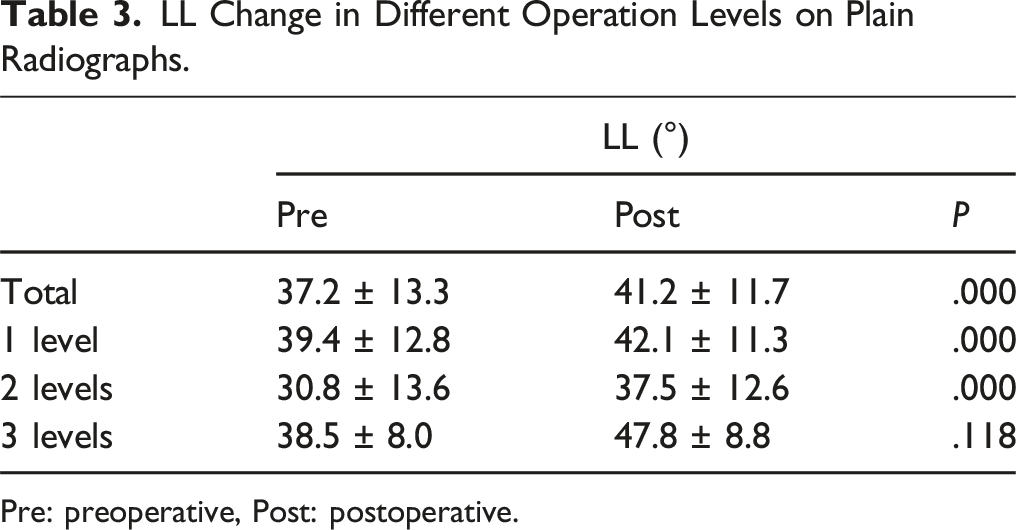
Pre: preoperative, Post: postoperative.
Measurements of the mean cross-sectional area of the thecal sac (CSA) on MRI indicated a statistically significant increase from 112.4 ± 39.7 mm2 to 131.7 ± 40.6 mm2 (P = .000 < .05), confirming that OLIF effectively enlarged the lumbar spinal canal. This effect remained consistent across different diagnostic subgroups (P < .05), demonstrating that it was not influenced by diagnosis. This trend was also observed in L3/4 and L4/5 lumbar levels, with statistical significance (P = .000 < .05). However, for L2/3, the change from 118.2 ± 47.1 mm2 to 131.8 ± 44.7 mm2 was not statistically significant (P = .203 > .05). (See Table 2)
Accuracy of the Cage Placement
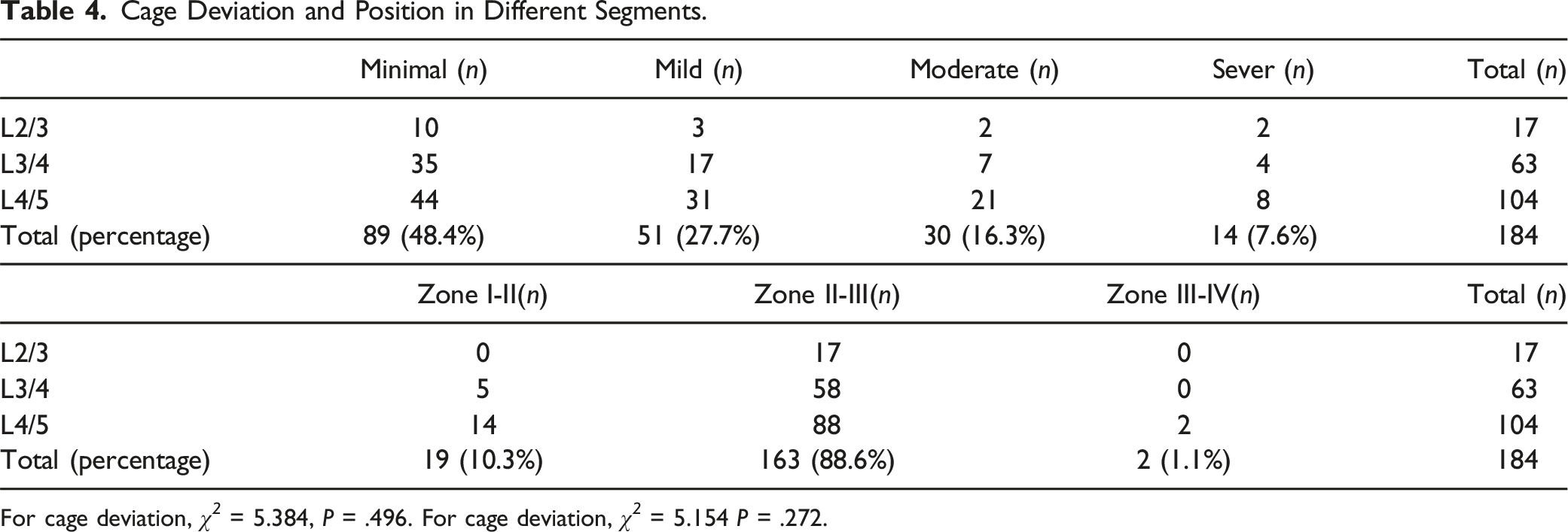
In terms of cage placement on postoperative MRI, out of the 184 cages, 19 were positioned in zoneI-II, two were in zone III-IV; the remaining 163 cages were situated in zone II-Ⅲ. (See Figure 4) No statistically significant differences in cage malposition were found across different diagnoses (χ2 = 2.753, P = .600 > .05) or different levels (χ2 = 5.154, P = .272 > .05). The median degree of cage deviation was 4.97°. Cage deviation indicated no statistically significant differences (H = 2.479, p = .290 > .05) among different segments. When cage obliquity was categorized into four degrees, no statistically significant differences were found between different segments (χ2 = 5.384, P = .496 > .05). (See Table 4) (a) The A-P X-ray view shows the three lines of the oblique lumbar interbody fusion cage. (b) The lateral view also shows three lines of the OLIF cage. (c) Axil view of MRI shows the cage was in II-III zone, cage deviation angle 0°. Cage Deviation and Position in Different Segments. For cage deviation, χ
2
= 5.384, P = .496. For cage deviation, χ
2
= 5.154 P = .272.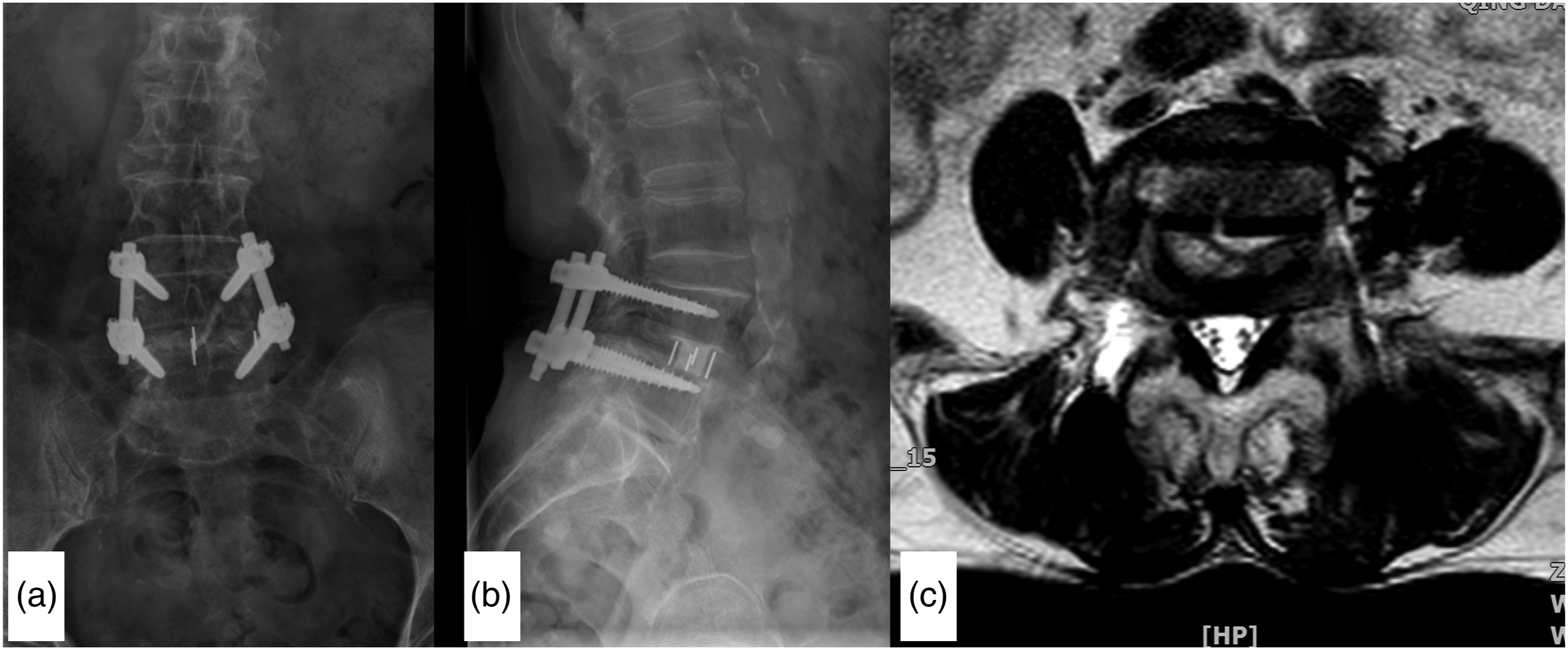
Effects of Cage Placement on Radiological Outcome
No statistically significant correlations were observed between cage angulation and changes in other radiological parameters, either in the overall population or in different segment and diagnosis subgroups. Additionally, no differences in radiological parameter changes were noted among different cage obliquity categories.
Adverse Outcomes
Among 14 severe cage deviation cases, one case experienced transient injury to the contralateral traversing nerve root due to severe cage deviation in L4-5 level, where the cage was positioned in zone III-IV. (See Figure 5) (a) The A-P X-ray view show the four lines of the oblique lumbar interbody fusion cage and the distance between the middle two lines was too large. (b) The lateral view also shows four lines and the distance between the middle two lines was also large, the posterior line was near to the posterior border of the vertebra. (c) Axil view of MRI shows the cage was in III-IV zone, cage deviation angle 30°.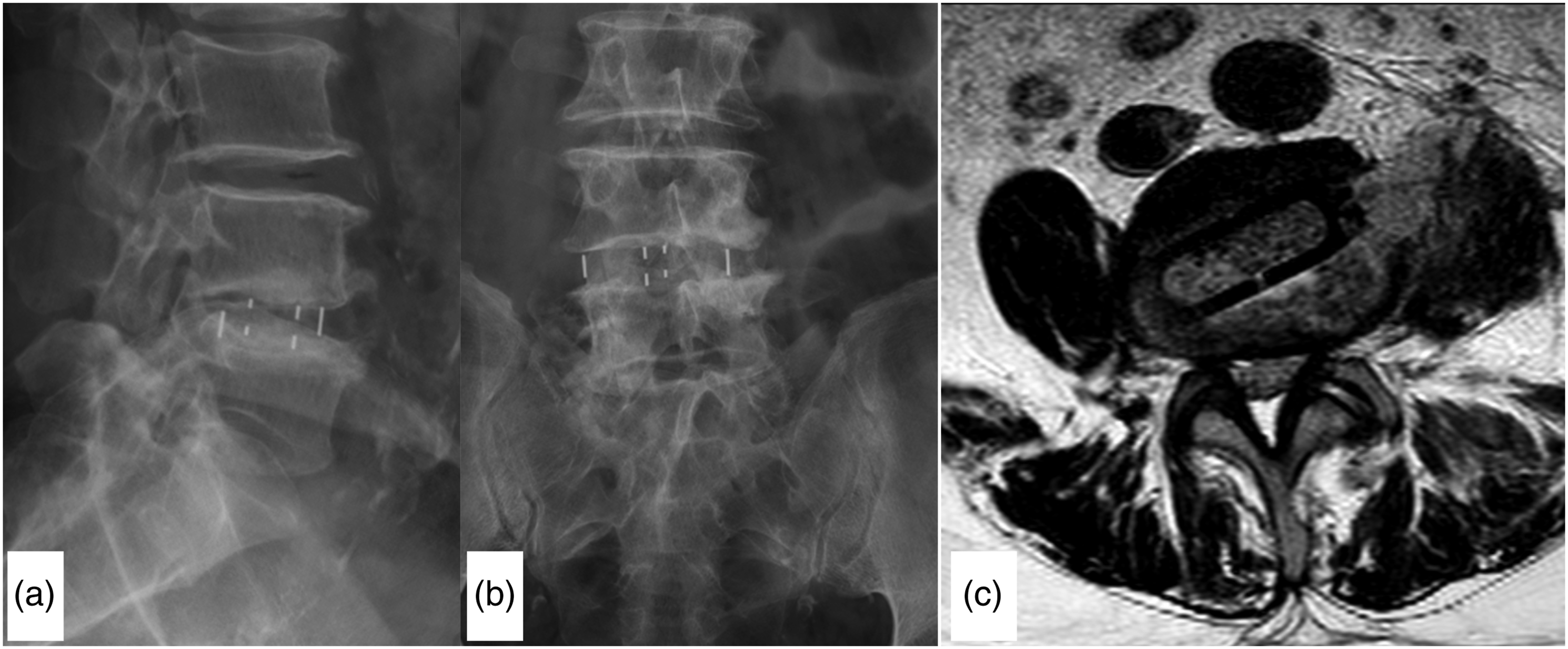
Discussion
Usually, correct insertion of cage is thought to be one of the most important target for OLIF surgeons, which is crucial to achieve indirect decompression. In our study, most cages (98.91%) were inserted zone Ⅰ-Ⅲ with median deviation of 4.97°, minimal to moderate deviating cages accounting 92.4%. Radiological parameters including ADH, PDH, FH, DSA, LL, SSA and CSA were enlarged significantly in most conditions, revealing effective indirect decompression of OLIF. However, it seemed that minimal to moderate cage deviation had no significant relations with indirect decompression efficacy according to our analysis.
The OLIF technique, short for oblique extroversion (OLIF) technology, primarily involves a specific anatomical approach and trajectory direction.10-12 Initially, a cage is introduced into the disc space via an oblique trajectory. Subsequently, it is rotated to attain a true lateral direction perpendicular to the vertebral body within the sagittal plane. Finally, optimal placement of the cage is achieved within zones Ⅱ and Ⅲ, spanning bilateral epiphyseal rings. Standard anterior-posterior and lateral C-arm fluoroscopy reveals three lines embedded within the cage.
In our study, cage positioning was assessed using MRI due to its superior clarity compared to CT scans. This approach significantly reduces patient exposure to extended radiation, as seen in CT scans.
Correct positioning of the OLIF cage within appropriate zones is vital to: (1) prevent disruption of the anterior longitudinal ligament, (2) avoid encroachment upon the spinal canal, sympathetic chain, and contralateral traversing nerve roots, (3) induce SA and lumbar lordosis based on the OLIF cage angle, and (4) restore disc height to indirectly decompress the spinal canal and prevent cage sedimentation.
The definition of “accurate cage position” in OLIF has evolved historically. Initially, “safe” working zones for transpsoas surgeries like XILF, DLIF, and LLIF were determined based on the lumbar plexus location. In a cadaveric study, Uribe 9 et al. demonstrated that for L1-2 to L3-4, zone Ⅲ was the safest, while the midpoint between zones Ⅱ and Ⅲ was safest for L4-5. However, in the ventral prepsoas approach of OLIF, the involvement of the lumbar plexus is minimal. Zone Ⅳ, being close to the canal, was previously deemed inaccurate.9,14,15 Thus, in 2020, Zhuo et al. redefined accurate cage positioning of OLIF within zones Ⅰ to III. 16
In our study, among 184 levels, 19 cages were in zone Ⅰ-Ⅱ (10.32%), 163 were in zone Ⅱ-Ⅲ (88.59%), and two were in zone III-IV (1.09%). Despite the use of C-arm biplanar fluoroscopy during surgery, the OLIF cage position exhibited quite high accuracy rates.
For lateral and anterior techniques like XLIF, LLIF, OLIF, and ALIF, maintaining navigation accuracy during procedures is challenging due to variations in lordosis/kyphosis and disc heights during cage placement.17,18 Until now, no reports detailed the type and extent of OLIF cage deviations. We introduced a classification system for cage deviations based on the angle between the cage’s long axis and the vertebral body’s horizontal axis. This system categorizes deviations by type and degree, with four levels: minimal, mild, moderate, and severe, with a 5° standard.
Accurate cage placement is crucial for restoring disc height, achieving indirect decompression, aligning sagittal and coronal profiles, and preventing cage settling. We defined the accuracy of cage positioning using the angle formed by the cage’s long axis and the vertebral body’s horizontal axis. This offers a valuable supplement to Uribe’s anatomical study for defining safe working zones.
In our study, minimal, mild, moderate, and severe cage deviations occurred in 89 (48.4%), 51 (27.7%), 30 (16.3%), and 14 (7.6%) cases, respectively. Severe cage deviations were seen in 7.6% of the total 184 levels, and among these, one case experienced transient injury to the contralateral traversing nerve root due to severe cage deviation in the L4,5 level, where the cage was positioned in zone Ⅲ-Ⅳ. (See Figure 5)
Mainly, cage deviations occurred posteriorly, primarily because cages weren’t rotated to the true lateral direction during insertion. Anterior cage deviations occurred in only 10 discs (5.43%), indicating over-rotation of the cage.
A critical concern arises when the cage is severely deviated within zone III-IV. Contralateral traversing nerve root injuries have been frequently reported.19,20 This is primarily attributed to the oblique angle required for OLIF, causing initial insertion of the interbody in the contralateral posterior direction toward the neuroforamen. Another contributing factor is incomplete disc resection. In L4,5 OLIF cases, encountering a high iliac crest can obstruct proper rotation of the cage to the true lateral direction. The cage should be inserted from the crack of blades which formed the “V” with the corridor.
Lumbar spinal stenosis was identified as one of the most suitable indications for OLIF. The spinal canal appeared to enlarge after intervertebral space distraction and thinning of the ligamentum flavum, although this change was sometimes difficult to discern on MRI. The study observed increased ADH, PDH, FH, FA and DSA in conditions like lumbar spinal stenosis, degenerative spondylolisthesis, and lumbar degenerative scoliosis. At the L2/3 level, PDH, FA and CSA did not significantly change postoperatively. LL and SSA changed after surgery, and CSA exhibited significant enlargement.
No statistical differences in radiological outcomes were noted between the 19 levels located in zone Ⅰ-Ⅱ and the 163 levels in zone Ⅱ-Ⅲ. Similarly, no significant differences in cage malposition were observed across lumbar spinal stenosis, degenerative spondylolisthesis, and lumbar degenerative scoliosis, as well as different levels.
While minimal, mild, and moderate cage deviations do not appear to impact radiological outcomes, it remains crucial to ensure the orthogonal insertion of the OLIF cage, preventing severe cage deviations that could lead to contralateral traversing nerve root injuries.
The strength of this study included a novel classification system of cage angulation on postoperative MRI, which might contribute to define safe working zones of OLIF. Also, we answered whether an “imperfect” cage insertion with deviation was acceptable. This study had several limitations. In our study, only radiological outcomes of OLIF was focused, ignoring the clinical manifestations of cage deviation and malplacement assessed by functional scores and follow-up, which might be more meaningful. Also, limited cases with different operation levels and diagnosis might draw certain biases to the results, which reduced reliability of this study. Therefore, further studies including more cases, clinical assessment and follow-up are needed.
Conclusions
Using C-arm biplanar fluoroscopy during surgery, approximately 98.91% of cages were placed in zones Ⅰ-II and II-III. Most cages deviated posteriorly with CDA ranging minimal to moderate. The minimal to moderate cage deviation did not impact radiological outcomes significantly in OLIF. However, avoiding severe cage deviation is crucial to prevent contralateral traversing nerve root injuries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.