
Abstract
Study Design
A single-institution retrospective study of a cohort of patients who underwent internal fixation spine surgery for thoracolumbar burst fracture (TLBF).
Objective
To observe the imaging manifestations of intervertebral disc changes in TLBF, to analyze the relationship between the degree of disc injury and the Cobb angle increase.
Methods
We retrospectively analyzed the data of patients who underwent short-segment pedicle screw instrumentation in the spinal surgery department of a single hospital between January 2014 and December 2017 (n = 90). According to the magnetic resonance imaging characteristics of the superior intervertebral disc tissue of the injured vertebrae before the operation, the intervertebral disc injury was divided into three types, which was used for group allocation: group A, uninjured intervertebral disc group; group B, mild intervertebral disc injury group; and group C, severe intervertebral disc injury group. The main imaging results of the three groups Cobb, IVA, IHI, AHIV, and VAS were compared among groups.
Results
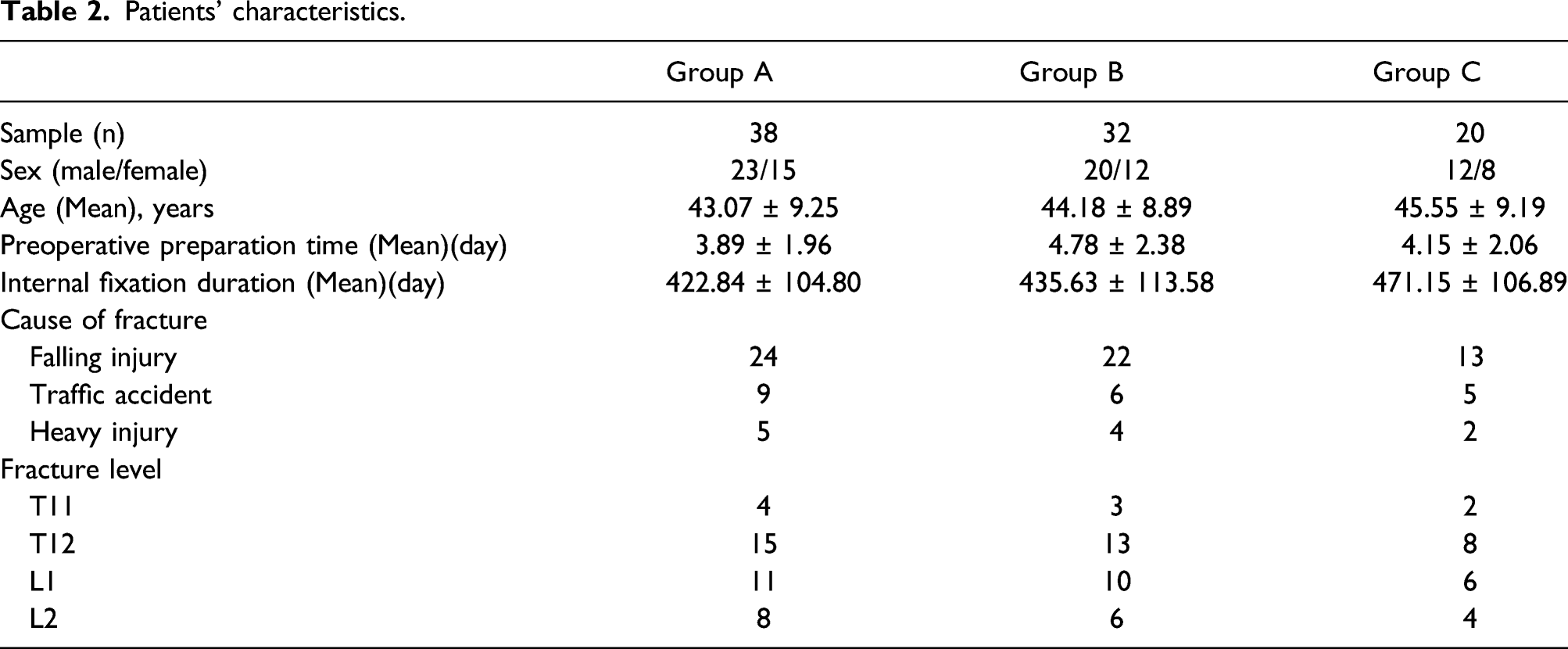
Ninety patients were included in the study (n = 38, 32, and 20, in groups A, B, and C, respectively). There was no statistically significant difference in demographics among the three groups (p > .05). 1-year post-surgery, the Cobb angle in group C differed significantly from that in groups A and B (p < .01). There was a significant difference in Cobb angle between groups A and B after internal fixation was removed for 6 months. At 1-year post-surgery, the IHI group C differed significantly from groups A and B (p < .01), while groups A and B were similar (p = .102); however, at 6 months after the internal fixation was removed, the IHI differed significantly between these two groups, also the AHIV between groups A and B was statistically significant (p < .01). The VAS pain score was similar among the three groups. Pearson’s test showed that the increase in the Cobb angle was moderately correlated with IVA and IHI, and weakly correlated with AHIV.
Conclusion
For TLBF with an intervertebral disc injury, the presurgical degree of intervertebral disc injury is the main reason for the post-surgery increase in the Cobb angle. Thus, diagnosis and treatment of this kind of patient require attention to the risk of spinal deformity.
Keywords
Background
With the rapid development of the domestic industry, construction industry, transportation industry, population growth, and increased aging, the number of patients with a spinal fracture is rising annually. Spinal fractures usually occur in the thoracolumbar segment (T11‒L2).1,2 Thoracolumbar burst fractures (TLBF) account for approximately 10–20% of all spinal fractures, 3 with more males than females affected. Mostly young adults are involved, with a high incidence among those aged 40–59 years. In addition, approximately 21–40% of thoracolumbar fractures are accompanied by varying degrees of nervous system damage,4,5 of which TLBFs pose a higher risk of injury.
Reduction and internal fixation with the posterior short-segment pedicle screw instrumentation (SPSI) is one of the treatment options for TLBF. Because screw placement through the injured vertebra can effectively restore the height of the anterior edge of the vertebral body, bone graft reconstruction through the injured vertebral pedicle can effectively maintain the reduction and can reduce the incidence of loss of kyphosis correction and failure of internal fixation.6,7 However, some patients have recurrent low back pain and kyphosis progression after the operation, particularly after the internal fixation device is removed.8,9 TLBF is often associated with different degrees of injury of the intervertebral disc above the injured vertebrae.10-13 However, to date, evaluation of TLBF with an injury of adjacent intervertebral discs has not received much attention, which may be one of the main reasons for the above phenomenon.
Therefore, we analyzed imaging findings of TLBF with an injury of consecutive intervertebral discs and evaluated the relationship between the degree of preoperative intervertebral disc injury and postoperative Cobb angle loss.
Methods
This study was approved by the Ethics Committee of the xxxx. A total of 524 patients with TLBF were selected from the Department of Spinal Surgery at our hospital, between January 2014 and December 2017. The inclusion criteria were as follows: age younger than 60 years; a presence of a fresh single segment TLBF (fresh TLBF was defined as a fracture of no more than 3 weeks) (AO typing: type A3); vertebral fracture mass without encroachment into the spinal canal or less than 30% of the canal, but without symptoms of neurological compression(vertebral fracture mass without encroachment into the spinal canal or less than 30% of the canal, but without symptoms of neurological compression); absence of a surgical history of intervertebral disc disease; availability of complete clinical and imaging data; and segments fixed by SPSI involve the injured vertebrae the superior and inferior adjacent vertebrae. Exclusion criteria were the following: age ≥60 years; pathological fracture, osteoporotic vertebral compression fracture, old fractures, severe spinal deformities, and other spinal diseases; other type AO–A3 fractures; a spinal canal occupying more than 30% of the space; ASIA neurological function grade D or above); incomplete clinical and imaging data; and absence of SPSI. Finally, according to inclusion and exclusion criteria, 90 patients were included in the study.
According to the preoperative magnetic resonance imaging (MRI) characteristics of intervertebral disc tissue, discs were divided into three types, which were used to allocate patients to three groups: type I, no damage to the intervertebral disc and no change in the shape and signal of the intervertebral disc; type II, mild intervertebral disc injury and changes in edema in the intervertebral disc accompanied by a change in intervertebral space height, with no endplate injury and annulus rupture; type III, in addition to all characteristics of type II, severe intervertebral disc injury accompanying endplate injury, with or without rupture of the fibrous annulus and occupation of the spinal canal space.
Parameters measured
The parameters recorded were the Cobb angle(Cobb), intervertebral angle (IVA), intervertebral height index (IHI), a former high rate of injured vertebrae (AHIV), and visual analog scale pain score (VAS) at 1 week, 1 year after surgery, and 6 months after internal fixation removal. Parameters were measured by two experienced spinal surgeons; three measurements were taken at each time-point and the average of both surgeons’ average values was taken for analysis (Figure 1). Classification of the degree of disc injury. A: Uninjured intervertebral disc group; B: Mild intervertebral disc injury group; C: Severe intervertebral disc injury group.
Statistical analysis
All data were processed using SPSS 21.0 (IBM, Armonk, NY). The counting data are represented as (x ± s) and were compared by one-way analysis of variance. Counting data were compared using the chi-squared test. Pearson’s test was used for correlation analysis. p < .05 was considered statistically significant.
Results
The distribution of disc injuries in included patients (n).


Measurement methods for each parameter. A: Cobb angle; B: Intervertebral angle; IHI: Intervertebral height index; C: Intervertebral height index (IHI): IHI = (b + d)/(a + c) × 100%, (a: width of the lower edge of the upper vertebral body of the intervertebral space; b: height of the anterior vertebral space; c: width of the upper edge of the lower vertebral body of the intervertebral space; d: height of the posterior vertebral space); D: anterior high rate (AHIV): AHIV = 2f/(e + g) × 100% (e: anterior border height of the upper vertebra of the injured vertebra, f: anterior border height of the injured vertebra, g: anterior border height of the lower vertebra of the injured vertebra).
Patients’ characteristics.
Parameter measurements at different time points.
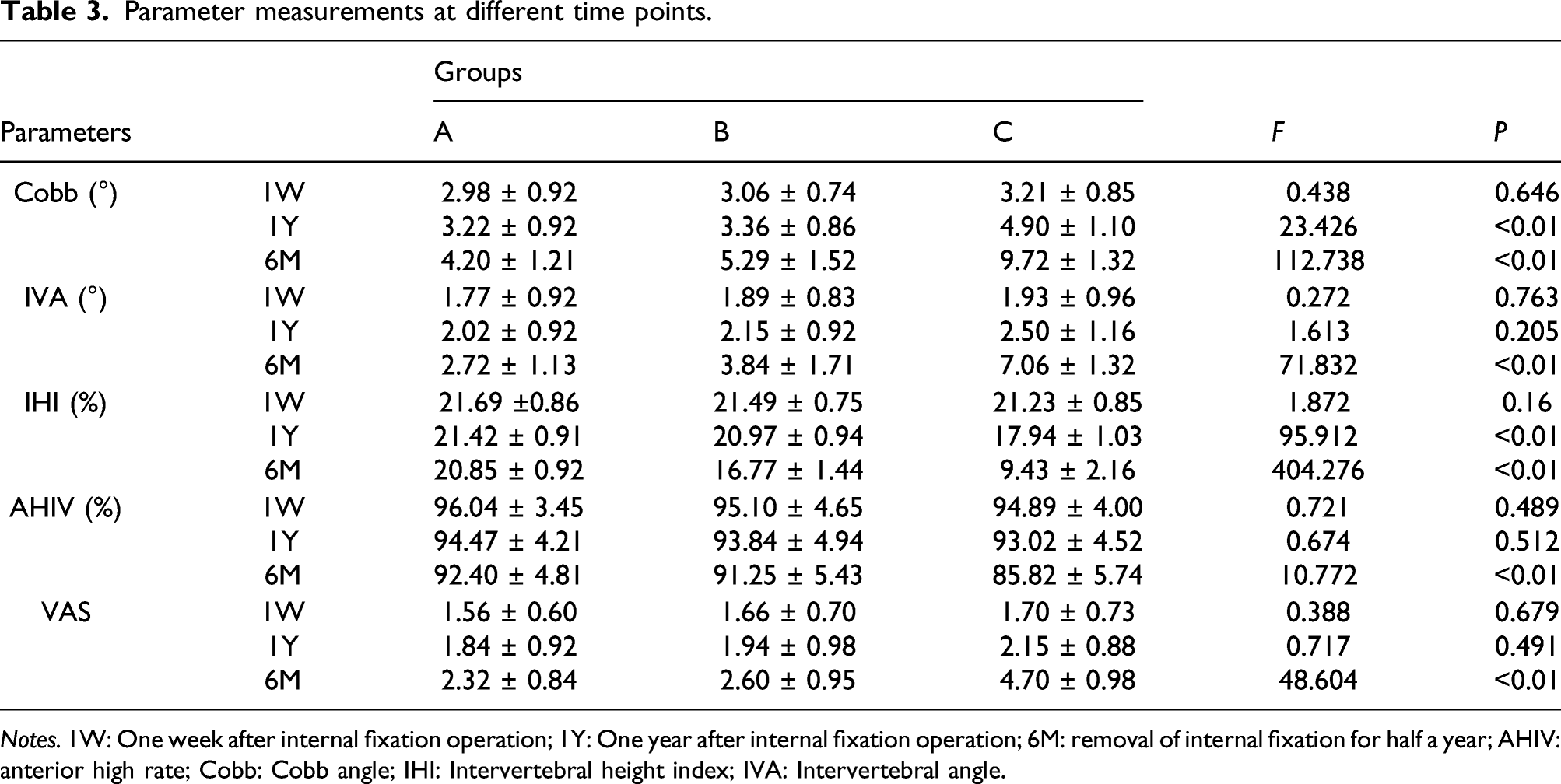
Notes. 1W: One week after internal fixation operation; 1Y: One year after internal fixation operation; 6M: removal of internal fixation for half a year; AHIV: anterior high rate; Cobb: Cobb angle; IHI: Intervertebral height index; IVA: Intervertebral angle.
Correlation of Cobb angle with IVA, IHI, and AHIV at 6 months after removal of internal fixation.

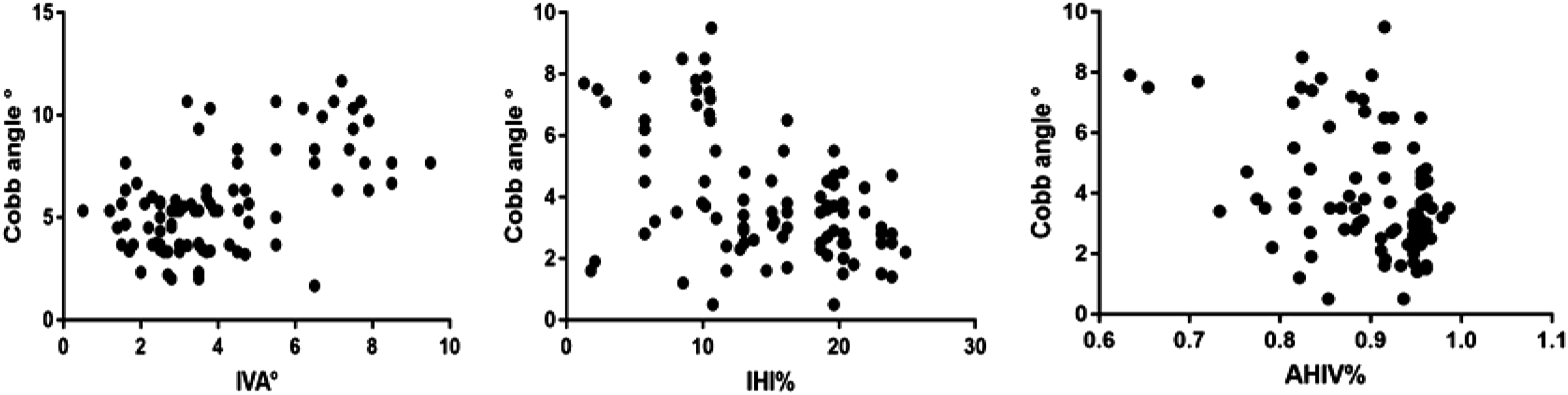
Scatter plots of Cobb Angle versus intervertebral angle (IVA), intervertebral height index (IHI), and the anterior high rate (AHIV) at 6 months after removal of the internal fixation.
Discussion
In this study, we investigated imaging manifestations of intervertebral disc changes in TLBF and analyzed the relationship between the degree of disc injury and the postoperative Cobb angle increase, to provide insights into TLBF treatment. We found that after using SPSI for TLBF with an intervertebral disc injury, more severe intervertebral disc injuries were more prone to postoperative complications such as loss of correction. Moreover, the change in the intervertebral disc shape is one of the main reasons for the progress in the kyphosis angle and the loss of the correction angle after surgery.
The degree of intervertebral disc injury increased with the increase in fracture degree and positively correlated with the AO fracture type.10,14 In our study, we also found that the degree of injury to the superior intervertebral disc was closely related to the severity of vertebral injury in TLBF. The intervertebral disc is a type of cartilage complex that is vulnerable to tension and shear force and can suffer traumatic injury under great compression force. Among the 90 patients included in this study, 52 patients had varying degrees of intervertebral disc injury, which demonstrates the vulnerability of the intervertebral disc during TLBF, and also reminds spinal surgeons that they should pay attention to injury of the intervertebral discs when treating patients with TLBF.
On the other hand, the special anatomical structure and composition of intervertebral discs determine its specific role in forming the spine and protecting the spinal cord, which also makes it extremely difficult to recover after intervertebral disc injury,15-20 with consequent secondary intervertebral disc degeneration, 21 fusion, 22 etc. TLBF is often complicated by an intervertebral disc injury, which can be reliably assessed by MRI.12,13,23 Of the TLBF patients, 67.2% were complicated with upper or inferior intervertebral disc injuries, of which the upper intervertebral disc injury accounted for 63.4% . 23 On the side hand, the nucleus pulposus is in a relatively closed environment and has an immune exemption. When the annulus fibrosus is ruptured, the herniated nucleus pulpous causes an immune response and pain, producing inflammatory factors (for example, IL-4 and TNF), which also accelerate intervertebral disc degeneration and inhibit its repair.24,25 A study reported that intervertebral disc injury caused by TLF can lead to increased apoptosis of intervertebral disc tissue. 26
While reducing the vertebral body, SPSI can indirectly reset the damaged endplate of the injured vertebra by using traction reduction of the upper and lower adjacent vertebral endplates and the restraint of the anterior and posterior longitudinal ligament and fibrous annulus, to achieve a good reduction effect. However, many centers have reported postoperative complications, such as loss of correction angle, progressive aggravation of kyphosis, and failure of internal fixation in TLF patients with an intervertebral disc injury, and it is suspected that intervertebral disc injury may be one of the main causes of these phenomena .2,21,27,28
The increase in Cobb angle is the most important parameter of postoperative correction loss; it can be used for objective evaluation of kyphosis in the sagittal position. 29 IVA is an important index for evaluating the morphological changes in intervertebral discs. 30 IHI can objectively reflect the height of the intervertebral disc. 31 AHIV reflects the height recovery and recompression ratio of the injured vertebrae. IVA, 30 IHI,21,31,32, and AHIV 33 can reflect changes in the Cobb angle, and it has been reported that changes in intervertebral disc morphology may be one of the main reasons for the change in this angle. 30 Our study also concluded that there was a significant positive correlation between the postoperative increase in the Cobb angle and IVA and IHI. There was also a certain correlation between AHIV and the change in the Cobb angle; thus, we infer that the change in the angle is mainly caused by incomplete reduction of the vertebral body and poor fracture healing after reduction or secondary compression of the vertebral body.
In this study, there was no significant loss of Cobb angle in groups A and B before and after the operation; however, for group C, we observed that intraoperative reduction of the fracture was intact and that all parameters were better at the last follow up than before the operation. However, changes in IHI, VAS score, and Cobb angle were observed at one postoperative year and 6 months after internal fixation removal. This was mainly due to the loss of effective support of the injured vertebrae and the weakening of the buffering effect after intervertebral disc injury. Vertebral reduction loss and intervertebral instability occur easily, as do IHI, IVA, and AHIV loss, which is then manifested as an increased Cobb angle. In addition, this can lead to the narrowing of the intervertebral foramen and the Modic changes that affect the sinus vertebral nerve and vertebral endplate, causing a gradual increase in the VAS pain score in these patients.34–37 Consequently, after using SPSI for TLBF combined with an intervertebral disc injury, postoperative complications, such as loss of correction, are more likely to occur in cases with more severe intervertebral disc injury. The change in intervertebral disc shape is one of the main reasons for the progression of the kyphosis angle and the loss of correction angle after surgery.
This study has some limitations. First, the study included a limited number of patients. Second, the type of disc injury was not classified in detail. Third, there is a lack of longer follow-up in patients who have had internal fixation removed. In future studies, the discectomy and fusion group should be targeted, compared with the posterior short-stage pedicle screw fixation group. And adding the type of disc injury to the grouping system.
Conclusions
In TLBF complicated with intervertebral disc injury, the degree of intervertebral disc injury before surgery appears to be the main reason for the increased Cobb angle after surgery. The more marked the increase in IVA and IHI, the greater was the increase in the Cobb angle in our study. In clinical practice, this implies that more attention should be paid to the diagnosis and treatment of these patients, to avoid the occurrence of late complications.
Supplemental Material
Supplemental Material - Intervertebral disc injury is the mainspring for the postoperative increase in Cobb Angle after thoracolumbar burst fracture
Supplemental Material for Intervertebral disc injury is the mainspring for the postoperative increase in Cobb Angle after thoracolumbar burst fracture by Zhi Peng, Zhongfeng Cui, Xiaolin Kuang, Chen Yu, Yushan Ruan, Chuan Li, Shaobo Li and Sheng Lu in Journal of Orthopaedic Surgery.
Footnotes
Acknowledgements
We would like to thank all the people who helped us with this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s note
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by theScientific Research Foundation project of the Education Department of Yunnan Province (2019FH001(-015)) and The "Ten Thousand People Plan" of Yunnan province - Medical Experts project (2019).
Supplemental material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.