
Abstract
Purpose:
Scoliosis is a prevalent condition among individuals with cerebral palsy, characterized by an inability to maintain spinal alignment due to diminished muscle tone. This progressive curvature becomes structural over time, resulting in physical impairment and challenges in daily activities. Consequently, therapeutic intervention is essential. Historically, brace therapy has been extensively utilized, but its efficacy remains uncertain.
Methods:
A systematic review was conducted across four databases to compile all relevant studies and reviews pertaining to brace therapy in cerebral palsy patients. Each article was independently assessed by two researchers and evaluated using the SIGN tool.
Results:
Eight studies were included, comprising six retrospective and two prospective studies, all rated as “acceptable” or “high quality.” Brace therapy demonstrated a temporary positive effect, with improved Cobb angles observed during brace usage, particularly in patients under 15 years of age, due to incomplete spinal maturation. However, this improvement is transient, as Cobb angles tend to increase once the brace is removed, diminishing its effectiveness. In addition, brace therapy positively impacts quality of life by enhancing posture and reducing pain, although these benefits also diminish over time, potentially leading to a decline in quality of life.
Conclusions:
Brace therapy offers temporary relief for physical and daily life challenges associated with cerebral palsy. However, its effects are not sustained, necessitating operative techniques for long-term management. This was a systematic review of Level-II studies or Level-I studies with inconsistent results.
Introduction
Cerebral palsy (CP) is a group of permanent disorders affecting the development of movement and posture, caused by non-progressive disorders occurring in the developing fetal or infant brain. These motor impairments lead to limitations in activity and are frequently associated with disturbances in sensation, perception, cognition, communication, and behavior. In addition, epilepsy and secondary musculoskeletal complications are common comorbidities. 1 With a prevalence of 2–3 per 1000 live births, CP represents the most common physical disability in childhood.
Scoliosis is a frequent orthopedic problem in individuals with CP. It is defined as a Cobb’s angle of ≥10° on a coronal full spine X-ray. The global prevalence of scoliosis is estimated at 1%–2%, which is markedly higher in children with CP. Depending on age, severity of CP, and radiological method, the prevalence of scoliosis in the CP population ranges from 15% to 80%. 2
The severity of scoliosis correlates with the level of the motor disability (classified by the Gross Motor Function Classification System (GMFCS)), the age of onset of scoliosis, and the extent to which the body is affected by CP. A large-scale study involving 2450 CP children reported an incidence of scoliosis of 39.9%, 16.8%, and 7.4% in GMFCS levels V, IV, and III, respectively. 3 Greater motor impairment not only increases the likelihood of scoliosis but also correlates with more severe curvature progression. Early onset of scoliosis is associated with a higher progression of scoliosis during growth. Quadriplegic involvement of CP is another factor associated with more severe spinal deformities. Curves exceeding 40° develop in up to 30% of quadriplegic patients, 10% in those with diplegia, and only 2% in unilateral involved patients. By contrast, curvatures >30° occur in only 0.1%–0.2% of patients with idiopathic scoliosis. 2
In the absence of therapeutic intervention, scoliosis in CP patients tends to progress. The reduced muscle tone and imbalanced trunk musculature hinder their ability to maintain a straight spine, resulting in the development of structural scoliosis. This progression is particularly rapid in young patients due to growth and bone maturation, leading to a swift increase in the severity of scoliosis.4,5
Trunk shift (TS) and pelvic obliquity (PO) are additional conditions observed in CP patients with scoliosis. These occur secondary to contractures of the truncal muscles. The prevalence of PO in CP patients has been reported to be as high as 59.9%. These deformities contribute to a decrease in quality of life (QoL), abnormal posture, and pain. 6
Severe spinal curvatures may lead to difficulties in sitting, which, in turn, negatively affect respiratory function, communication, motor performance, and nutrition. Malpositioning and inability to change position in combination with difficulties in expressing their discomfort and pain increase the risk of developing pressure points on bony structures like the tuber ischiadicum and the major trochanter. 2 Jahnsen et al. studied the occurrence of pain in patients with CP. A questionnaire completed by 406 patients showed that 72% of CP patients experienced pain, most commonly localized to the neck, back, and lower limbs. 7
Respiratory dysfunction is another problem in children with severe CP. It is thought to be caused by weakness of respiratory muscles, abnormal compliance of the chest wall and lungs, and a ventilation-perfusion mismatch. An additional scoliosis and thoracic deformity may further restrict the capacity and compliance of the lungs. 8
Given the substantial impact of scoliosis on the functional capacity and QoL of individuals with CP and their caregivers, adequate prevention and intervention are critical. The underlying etiology of scoliosis in CP differs significantly from idiopathic scoliosis, necessitating tailored management strategies. 9
Non-operative treatment includes observation, usage of seating devices, and/or spinal orthosis. It is considered not to be as effective in CP patients as in patients with idiopathic scoliosis. 10 Surgical options range from growing rods or bipolar fusionless, less invasive techniques to spinal fixation.11,12 The surgical complication risk for spinal surgery in CP patients is well-documented.2,13 Complications are remarkably higher than in patients with idiopathic scoliosis due to medical comorbidities. 9 Therefore, unlike in idiopathic scoliosis, scoliosis surgery in children with CP is sometimes, especially by parents and other non-surgical caregivers, considered a last resort, gaining a place in treatment. 2
This literature review aims to shed light on the outcomes of non-surgical treatment of scoliosis in children with CP, more specifically those classified as GMFCS IV–V, by assessing the impact of bracing therapy on progression of spinal curvature and the impact on QoL.
Methods
Search strategy
A comprehensive literature search was conducted in March 2025 using the following databases: PubMed, Embase, Medline, and Cochrane Library. The following terms were used: “cerebral palsy,” “scoliosis,” and “brac*,” connected by the preposition “AND.” Additional relevant articles were identified by screening the reference lists of included articles.
Inclusion criteria
Studies meeting the following criteria were included: (i) study design: systematic and narrative reviews, and controlled trials; (ii) type of intervention: bracing for scoliosis; and (iii) populations: studies must include children diagnosed with CP, GMFCS IV or V, with associated scoliosis. Studies addressing neuromuscular scoliosis were only included if a cutoff of 80% CP population was reached or if a separate analysis for the CP population was conducted.
Exclusion criteria
Studies meeting one of the following criteria were excluded: (i) study design: conference abstracts; (ii) type of intervention: studies solely addressing interventions other than bracing, like surgical treatments, Botox injections, neuromuscular electrical stimulation, selective dorsal rhizotomy, etc. There was no exclusion based on the prior treatments patients had received. (iii) Population: studies involving other diseases than CP, studies involving neuromuscular scoliosis with less than 80% of the population representing CP patients, and studies involving normal developing children (iv) language: studies published in languages other than English or German.
Data abstraction
Two independent raters evaluated the articles. The review process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. At first, the articles were rated by title and abstract, according to the inclusion and exclusion criteria. In the second round, the leftover articles were evaluated on full text, aligned with the inclusion and exclusion criteria. From the remaining articles, the following data were abstracted (Table 1): title, authors, publication date, study design, population, population size, aim, follow-up, intervention, outcome parameters, complications, and results. As outcome parameters, we abstracted Cobb angle, progression of the Cobb angle, trunk shift, pelvic obliquity, and effect on pulmonary function, sitting balance, and pain.
Patient characteristics.
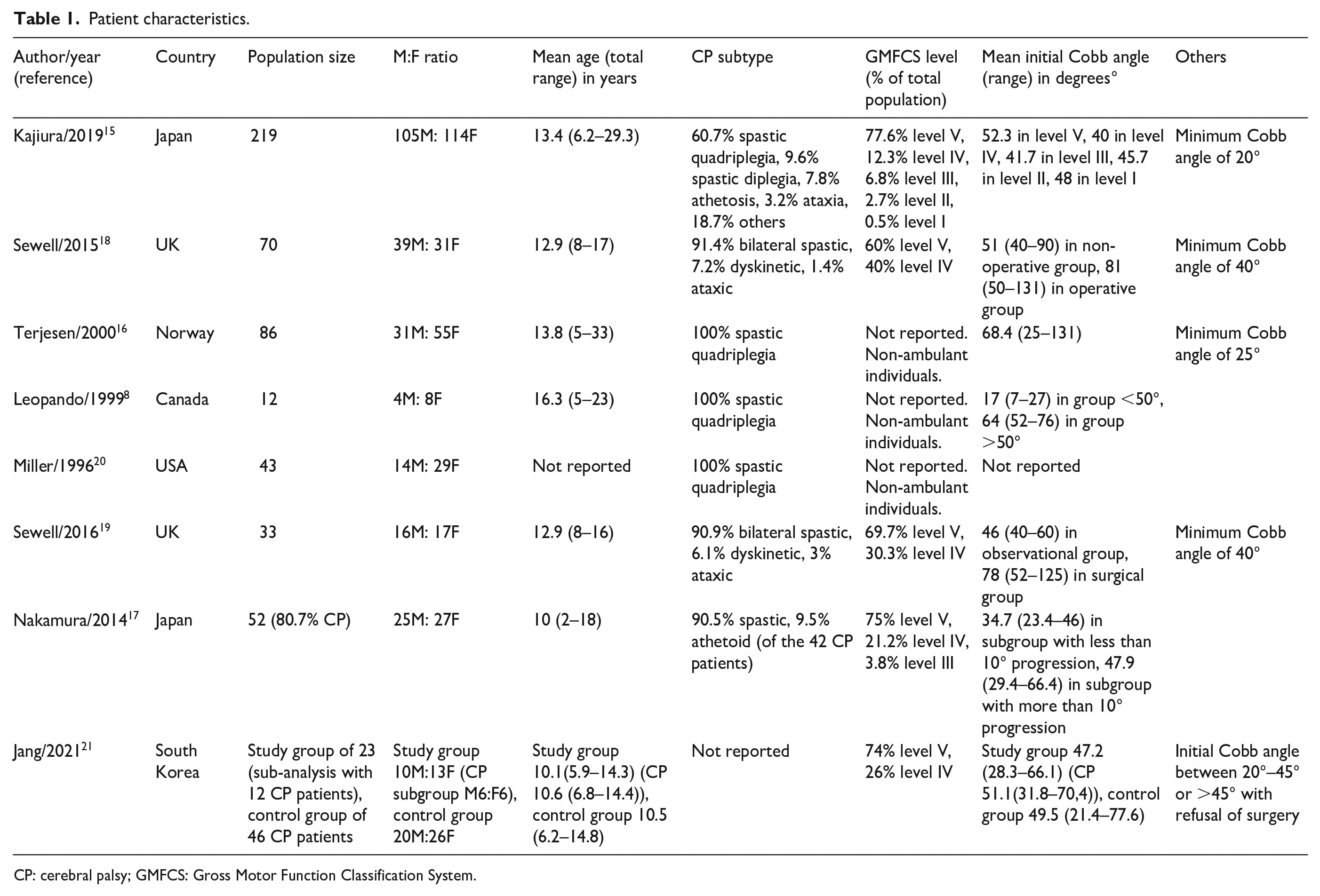
CP: cerebral palsy; GMFCS: Gross Motor Function Classification System.
Outcome parameters
To evaluate the impact of bracing on CP patients with scoliosis, multiple clinical and functional outcomes were considered (Table 2): starting with the severity of scoliosis and its progression, measured by the Cobb angle. Annual progression is used to describe the mean progression of the Cobb angle in a year. TS and PO were assessed as indicators of postural imbalance. Different radiographic methods were used across the studies (e.g., Maloney and O’Brien method). And as a last parameter, evaluation of quality of life was included. The impact of bracing on the QoL of patients with CP was assessed through various scoring systems. Some studies employed their scoring systems, while others chose to use standardized questionnaires, such as the performance version of the Activities Scale for Kids (ASKp), the Assessment of Caregiver Experience with Neuromuscular Disease (ACEND), or the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD). Questionnaires were filled in by patients and/or their caregivers. Patients can suffer from difficulties as a consequence of the disease but also of the therapy (i.e., sitting balance, pain, breathing, etc.).
Outcome parameters.
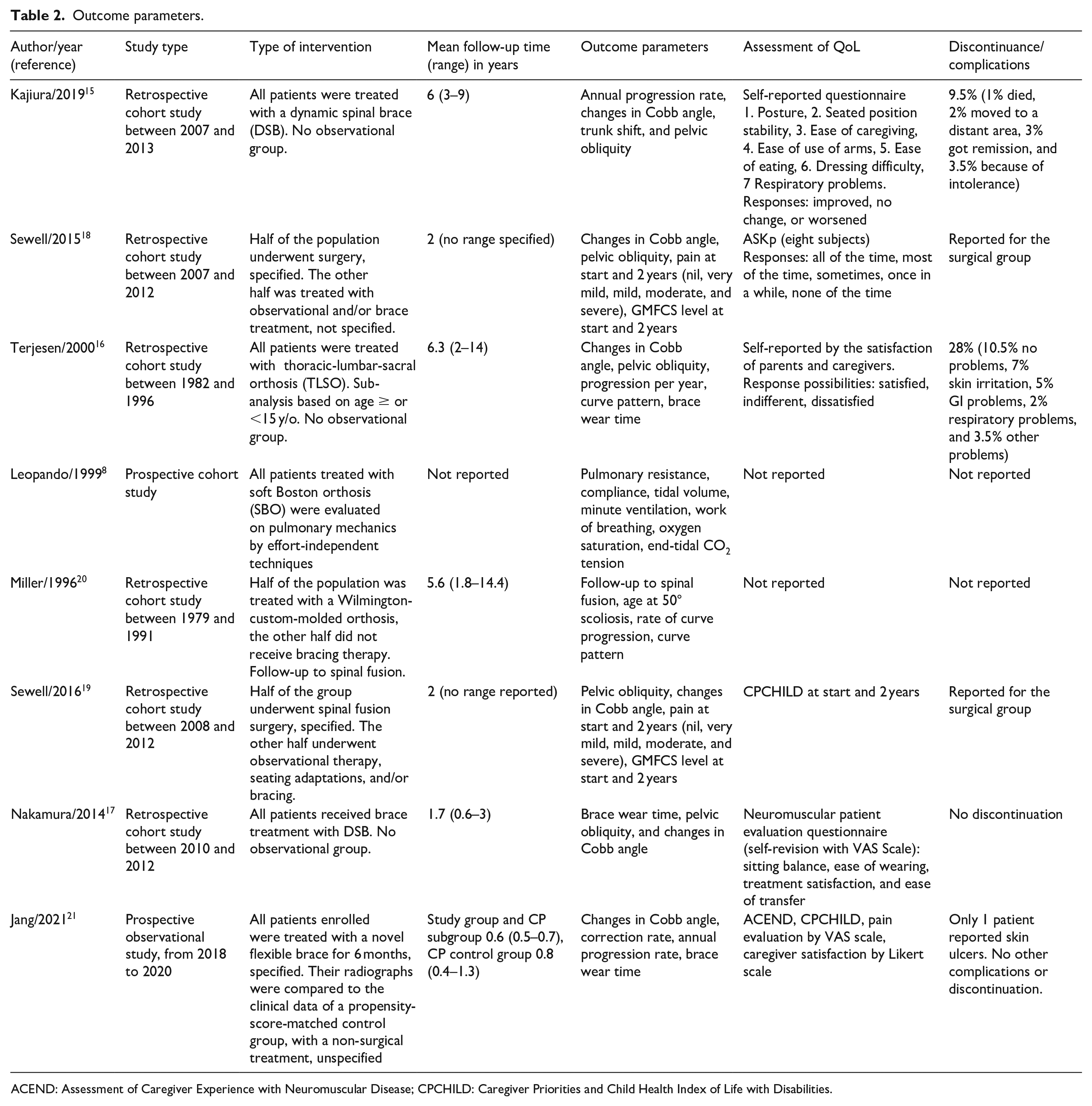
ACEND: Assessment of Caregiver Experience with Neuromuscular Disease; CPCHILD: Caregiver Priorities and Child Health Index of Life with Disabilities.
Results
A total of 183 records were identified through the database search, with 20 articles meeting inclusion criteria (Figure 1). Of these, eight were studies (six retrospective and two prospective studies) and 12 were narrative reviews. No systematic reviews were identified.
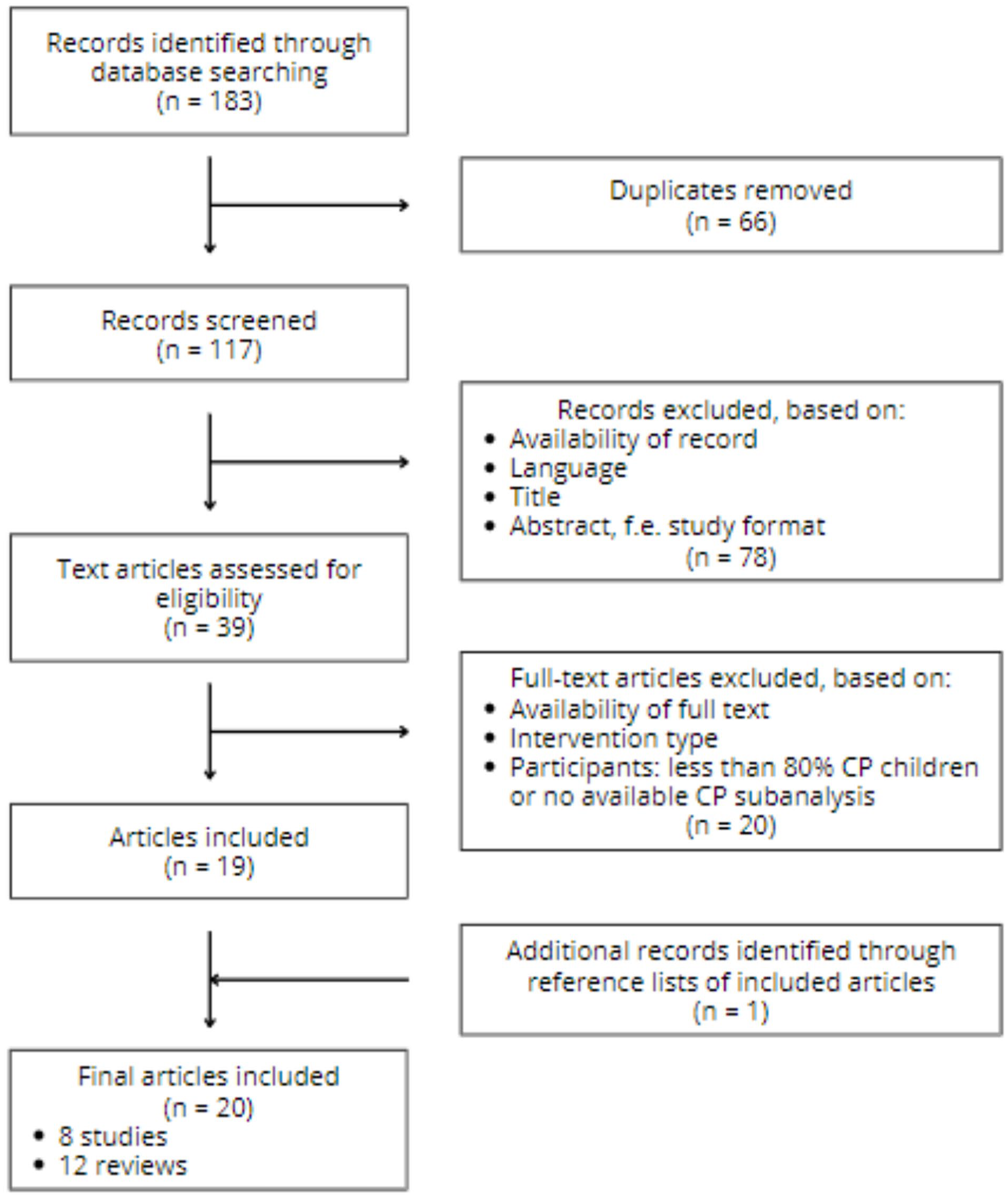
Flowchart of search strategy.
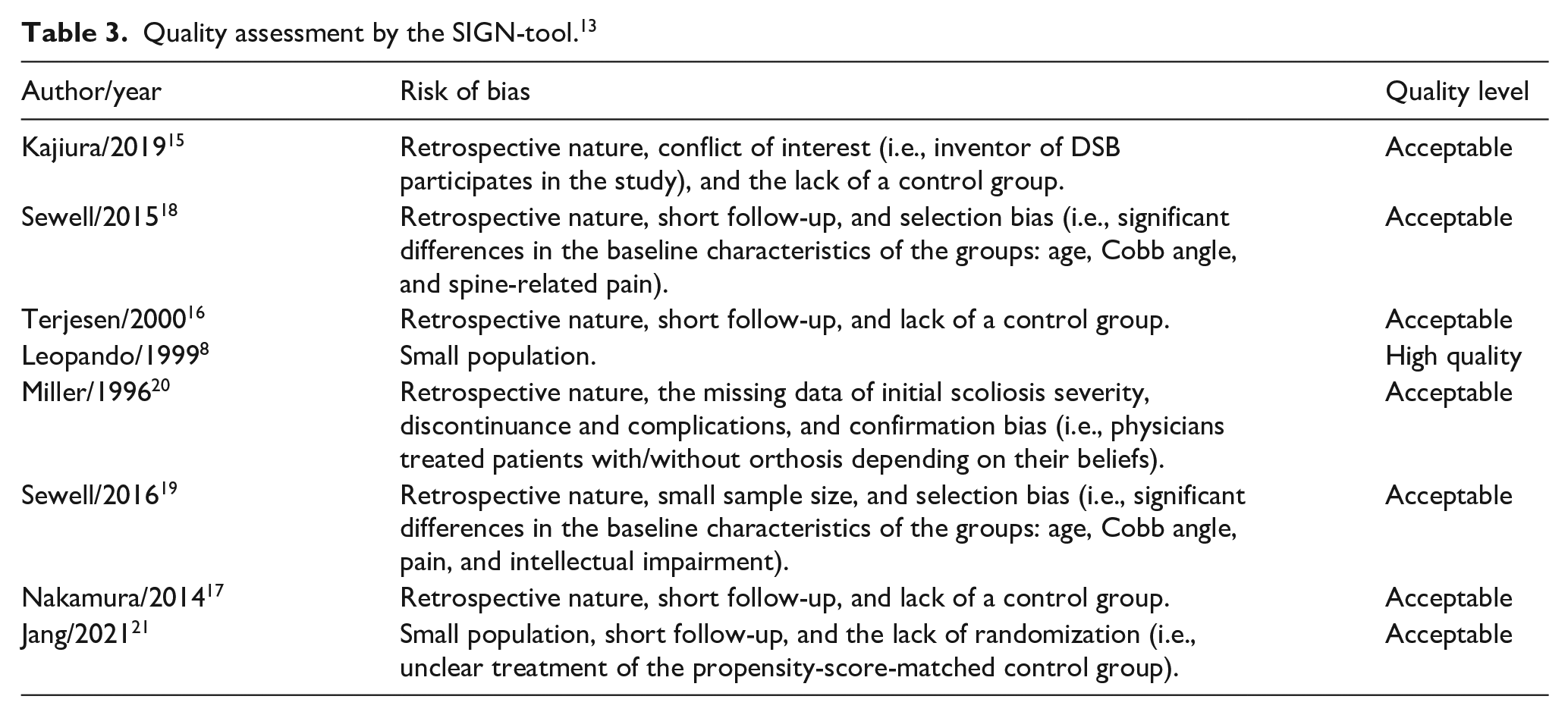
An analysis of the quality of evidence and risk of bias for the included studies was conducted, using the SIGN-tool designed for cohort studies, 14 categorizing the studies with an ordinal scale: “high quality,” “acceptable quality,” or “unacceptable quality.” Due to the retrospective design of six out of the eight articles, only acceptable levels of quality could be reached. All included articles had relatively short follow-up times, with a mean follow-up time ranging from 6 months in one of the included studies to 2–6 years in most other studies. Population sizes were overall small, and frequently, no control group was used.15 –17 Potential biases included conflict of interest, 15 selection bias,18,19 confirmation bias, 20 and the lack of information and/or randomization.20,21
Severity of scoliosis measured by Cobb angle
Several studies report a correction of the Cobb angle in CP patients while wearing spinal braces.15,16,19 Kajiura et al. 15 report an initial correction of 34.3% in a study with 219 patients with a Cobb angle of ≥20°. The Cobb angle is corrected from 49.9° to 32.8° when wearing a brace. A study by Terjesen et al. 16 found a correction of 38.1% (68.4° to 43.9°). The study included 86 patients with baseline Cobb angles ranging from 25° to 131°. Kajiura et al. 15 also observed age-dependent differences in correction, with patients younger than 15 years achieving a 37% correction, compared to a 28.9% correction in patients aged 15 years and older. These findings were contradicted by Terjesen et al., 16 who reported no significant differences in correction rate across these age categories.
Despite initial correction of Cobb angles, the effectiveness of bracing declines over time. After a 3-year follow-up, Kajiura et al. 15 observed a reduction in correction from 34.3% at the start of the treatment to 19.3% after the follow-up period. These results were confirmed by Terjesen et al., 16 who reported a reduction from 38.1% to 22.6%. In a study by Nakamura et al., 17 a study with 52 patients, only a significant correction in half sitting position was observed, unlike when the patient was in supine position. They also reported a decreased correction by increasing age and stated a higher correction in patients where more vertebrae were involved.
Progression of the Cobb angle, despite bracing, was noted across studies.15 –20 Terjesen et al. 16 concluded a progression of the Cobb angle from 68.4° initially to 93.1° at final follow-up, both measured without the orthosis. The annual progression rate was 4.2°. In the age category of <15 years, the annual progression was significantly higher. Kajiura et al. 15 confirmed these results with a progression of Cobb angle from 49.9° at the initial presentation to 76.1° at the final presentation, both measured without orthosis. They reported a mean annual progression rate of 4.5°. They also reported a difference in age categories, with an annual progression of 5.8° in patients younger than 15 years, compared to only 1° for patients aged 15 years and older. This can be explained by the maturation of the skeleton. Miller et al. 20 compared a braced group of 21 patients with a non-braced group of 22 patients. Cobb angles of 50° were reached at an age of 12.5 years and 14 years, respectively. However, they reported no statistically significant effect from the use of orthosis on curve magnitude or curve progression rate. Jang et al. 21 report no significant difference in Cobb angle after final follow-up. This can be explained because of the short follow-up time of only 6 months. This period will be too short to evaluate changes in the Cobb angle.
Trunk shift and pelvic obliquity
Similar to the Cobb angle, TS and PO show initial improvement with bracing.15,19 Kajiura et al. 15 documented a significant reduction of TS and PO while wearing spinal orthosis, at the beginning and after therapy. Another study by Nakamura et al. 17 reported only an improvement after treatment, in a half-sitting position.
However, during follow-up, several studies reported a significant progression of TS and PO despite continued use of orthosis.15,16,19 Kajiura et al. 15 found that this progression was significant, although not for TS by patients of 15 years or older. Terjesen et al. 16 observed a significant increase in mean PO from 22° to 29°.
Quality of life
Seating balance and posture
The ability of “balanced sitting” or “posture” is said to be a significant predictor of satisfaction. 17 Orthosis can have a beneficial effect by permitting a better posture, head-neck control, and seating balance.15,16 This was reported by Sewell et al., 18 after comparing a brace-treated group, with a group treated with surgery. However, this improvement was only temporary. In the brace-treated group, seating balance declined and pain levels increased over a 2-year timespan, leading to a decline in ASKp scoring (i.e., a decline in QoL). By contrast, the operatively treated group, with higher initial pain scores, had increasing ASKp scores over time, due to decreased pain levels and a better seating balance.
The perception or experience of pain
Further investigating the impact of different factors on the QoL, Sewell et al. 19 found a moderate, although not significant, correlation between pain levels and QoL. CPCHILD questionnaires were all completed by the caregivers, and the perception of pain was evaluated using VAS scales. The brace-treated group had a significant decline in CPCHILD scores (i.e., a decline in QoL). The changes in the CPCHILD score were attributed to a change in the experience of pain and seating balance.
Jang et al. 21 aimed to compare a more flexible type of brace with a historical, propensity-score-matched control group. Not only were the specific characteristics of this control group lacking, but they also did not conduct a comparison of the QoL between both groups. In the treatment group, no significant improvement in the CPCHILD scores was found between baseline and 6 months after initiation of the novel flexible brace. Jang et al. 21 attribute the caregivers’ perception of ineffectiveness to the history of treatments the patient had already received: those who had experienced rigid bracing scored a decline in pain with the flexible brace, and those who were new to bracing techniques scored an increase in pain intensity.
Dermatological complications
Brace treatment can impact QoL by causing skin irritations, pressure points, or even hyperthermia. These complications were not found to be the cause of discontinuation of bracing16,17,21 and remained limited in occurrence. Nakamura et al. 17 observed that 3 of 53 patients experienced skin irritation and 2 of them developed mild hyperthermia. Jang et al. 21 reported 1 case of a skin ulcer in 23 patients.
Pulmonary function
Leopando et al. 8 investigated the impact of bracing on pulmonary function in children with CP (i.e., Soft Boston Orthosis). Their outcome parameters for the pulmonary mechanics and gas exchange were as follows: pulmonary resistance, pulmonary compliance, tidal volumes, ventilation per minute, oxygen saturation, the work of breathing, and CO2 end-tidal tension. A comparison of the results with and without orthosis was conducted per patient, in the seated and supine positions. No significant differences were found. The work of breathing increased when patients took off their brace in a seated position; however, this reached no statistical significance.
Feeding, convulsions, and others
To complete the research of QoL, no significant difference could be found in the feeding type or gastrointestinal problems between a bracing and a surgical intervention nor on communication level, intellect, or prevalence of seizures.17,18
Discussion
This review aims to evaluate the outcomes of spinal bracing as a treatment of scoliosis in children with CP, with a specific focus on two key domains: first, the influence on the severity and progression of scoliosis and second, the influence on QoL. A critical limitation across the included studies is the absence of a standardized assessment for both scoliosis severity and QoL, which are measured, respectively, in different positions and by different tools. This limits the comparability of outcomes.
Following a comprehensive literature search across multiple databases, 12 narrative reviews and eight original studies (six retrospective and two prospective) met the inclusion criteria. The reviews were all of a narrative nature. The most recent one dates from 2020. 4 To our knowledge, no critical appraisal had been conducted before. To fulfill this need, this systematic review includes a quality of evidence analysis on the eight included studies, using the SIGN tool (Table 3). 14 Across studies, the methodological quality was generally limited, with a considerable bias arising from retrospective designs, small sample sizes, and short follow-up durations. Additional sources of bias included confirmation bias—linked to conflicts of interest, lack of randomization, and absence of control groups—and selection bias, often due to restrictive inclusion criteria (e.g., minimum Cobb angle thresholds) and heterogeneity in baseline characteristics between comparison groups.
Quality assessment by the SIGN-tool. 13
The findings suggest that spinal bracing in children with CP has a limited impact on the scoliosis. The efficacy of brace treatment in improving Cobb angle, TS, and PO is limited to periods of active brace wear and was more effective in patients with flexible curves (i.e., in earlier developmental stages prior to skeletal maturation). In line with Brunner et al., no proof was found for brace therapy to be able to prevent curve progression in the long term.4,22 As the efficacy of a treatment correlates with its adequate use, publications should consequently report the hours of brace wear and ensure longer follow-up times. Terjesen et al. 17 advised daytime brace wear and not at night. Over 50% of the patients contributing wore the brace >10 h a day. Other studies reported average wear times of 10.2 ± 8.0 17 and 7.6 ± 5.5 21 hours a day. Unfortunately, many studies failed to report the duration of brace wear.
In addition to curve management, brace therapy is often justified by its potential to improve seated posture, reduce pain, and thereby enhance overall QoL.2,22 According to Weigl et al., 22 enhanced trunk support facilitates better head, neck, and upper extremity control, potentially enabling greater environmental interaction. The value of bracing should therefore be found in optimizing the QoL of CP patients, rather than trying to optimize the curve. This is in contrast with the intention of treatment in idiopathic scoliosis. 22
Nevertheless, while temporary improvements in posture and pain relief have been reported, these benefits often diminish over time, with some studies even showing a progressive decline in QoL among brace users.18,19 Importantly, it should be noted that none of the reviewed studies compared the seating balance and pain experience of a braced group with a true observational group.
In terms of complications, the incidence of adverse events related to pulmonary, dermatological, gastrointestinal, and neurological systems remained low in brace-treated groups. However, due to a lack of comparative data, particularly with untreated controls, no definitive conclusions can be drawn. Furthermore, when compared to a surgical group, bracing showed no significant differences in QoL based on these complications. 19
Another limitation of brace use is the occurrence of fractures secondary to seizures. Seizures are common in patients with CP and can lead to significant musculoskeletal trauma because of the accompanied low bone mineral density. The most common are rib and vertebral fractures. 23
Other options in non-surgical treatment include seating modifications. Literature indicates that children with cerebral palsy experience significant improvements in postural control and upper extremity function with the use of adaptive seating devices. These can be considered a viable alternative to rigid bracing. The decision between seating modifications and bracing should be individualized, taking into account the specific needs, functional abilities, and overall goals for each child. 24
Surgical intervention remains the treatment of choice in cases of progressive scoliosis that compromises the sitting posture. Unfortunately, this is associated with a high number of complications. Vandendriessche et al. 25 reported higher rates of postoperative respiratory and cardiovascular complications, wound infections, and decubitus ulcers in children with CP relative to those with idiopathic scoliosis. “Postoperative pneumonia was the most frequent complication in both patient groups (43% and 18% in CP and IS, respectively).”
Emerging approaches such as fusionless spinal surgery using minimally invasive bipolar techniques are gaining acceptance, particularly in younger CP patients with rapidly progressive deformities, as they appear to reduce the risk of severe complications.26,27
Howard et al. 28 studied the effect of surgery on Cobb angle and QoL in a 5-year follow-up study. After surgery, they reported a significant correction of the scoliosis and PO. Following a follow-up period of 5 years, no changes were found compared to directly postoperative. They also stated a positive effect on personal care, mobility, and comfort, leading to an improvement in QoL.
This review is subject to several limitations. First, small number of studies is available on this topic. Due to the variability in interventions and population characteristics, no meta-analysis could be conducted. Second, this review did not include an analysis of the curve pattern. Lastly, only one study compared a brace-treated group with a pure observational treatment without bracing. The remainder studies lacked control groups or utilized alternative interventions.
Based on current evidence, bracing therapy for scoliosis in CP patients offers only a temporary benefit in terms of Cobb angle correction and QoL. These benefits are most pronounced during the early stages of treatment and active brace wear. Bracing does not appear to prevent further deterioration of the curve and further decrease in QoL. In a later stage, bracing is unlikely to provide further benefit, and surgical options should be considered.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251361320 – Supplemental material for Bracing for scoliosis in children with cerebral palsy—a systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521251361320 for Bracing for scoliosis in children with cerebral palsy—a systematic review by Niels Merkelbach, Alix De Pauw and Anja Van Campenhout in Journal of Children's Orthopaedics
Footnotes
Author contributions
AVC conceived of the presented idea. NM and ADP conducted the literature search and drafted the manuscript. AVC supervised this work. All authors discussed the results. In the end, NM and AVC contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
There was no need for ethical approval because this was a clear literature-based systematic review.
Data availability statement
The data underlying this study are available in the main article and its supplementary material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.