
Abstract
The aim of this study was to assess the prevalence and associated factors of depressive symptoms and perceived stress among people with Type 2 diabetes mellitus (T2DM) in Nepal. Using a cross-sectional design, we collected data from 481 participants with T2DM in Kavrepalanchok and Nuwakot districts of Nepal. Depressive symptoms and perceived stress were assessed using Patient Health Questionnaire (PHQ-9) and Perceived Stress Scale, respectively. Associated independent variables were examined using binary logistic regression analyses. Of 481 participants, 123 (25.8%) had depressive symptoms (PHQ-9 score ≥5) and 156 (32.4%) experienced perceived stress. Low monthly income (<USD 215.52) and low diabetes medication adherence were significantly associated with both depressive symptoms and perceived stress. Mandatory screening and timely treatment for mental health conditions and assessment of medication adherence should be incorporated in the routine primary care of T2DM patients. A person-centred approach to T2DM management, considering the socio-economic determinants of the disease, should be prioritized by the healthcare system. Future studies should identify integrated care for the prevention and management of mental health comorbidities.
What We Already Know
Mental health conditions in people with type 2 diabetes mellitus (T2DM) is a major public health concern.
Studies have reported varying prevalence of depressive symptoms in people with T2DM in Nepal.
Little is known about the prevalence and associated factors of perceived stress in people with T2DM in Nepal.
What This Study Adds
This study adds to the existing body of evidence that there is a high prevalence of depressive symptoms and perceived stress in people with T2DM in Nepal.
Factors significantly associated with depressive symptoms and perceived stress included having a low monthly income and low medication adherence.
Findings of this study suggest mandatory screening and timely treatment of mental health conditions, routine assessment of medication adherence to be incorporated in the routine primary care of T2DM patients and the need for a person-centered approach to T2DM management, considering the socio-economic determinants of the disease.
Introduction
Type 2 diabetes mellitus (T2DM) has emerged as a serious public health threat globally, particularly in low- and middle-income countries (LMICs). Nearly half a billion people are living with T2DM worldwide, 75% of whom reside in LMICs. 1 People with T2DM are two to three times more likely to have depression than those without diabetes. 2 Likewise, people with T2DM are likely to have higher levels of perceived stress, which refers to how they experience and evaluate stress in their lives. 3 A diagnosis of T2DM may bring physical and emotional stress, which may lead to inactivity, poor nutrition, smoking, and alcohol use, ultimately worsening the condition. 4 Although the exact cause of mental health problems in people with T2DM is unclear, the never-ending daily management of T2DM and associated costs are likely to be the contributing factors. 5
There are varying reports on the prevalence of depressive symptoms and stress in people with T2DM worldwide. A review of 42 studies in South Asia showed a prevalence of depressive symptoms ranging from 11.6% to 67.5%. 6 Similarly, 39.3% of people with T2DM reported having high perceived stress in India, 7 and nearly 35% in Iran. 8 However, despite having a strong association with T2DM, mental health conditions often go undiagnosed and undertreated. A study conducted in India suggested that 49% of the people with T2DM had undiagnosed depression. 9 Several factors such as glucose imbalance, physical complications, and limited advice from health care practitioners regarding self-management behaviors for T2DM management have been associated with a high prevalence of undiagnosed mental health comorbidity in T2DM population. 9 Appropriate screening, timely diagnosis and treatment of these mental health conditions in people with T2DM may improve T2DM prognosis whereas, misidentification or delay in diagnosis will only exacerbate the risk of diabetic complications. 10
Studies conducted in Nepal have reported varying prevalence of depressive symptoms in people with T2DM, from 23% 11 to 54%. 12 Furthermore, studies conducted in Nepal so far were either mostly hospital-based or based on community-based studies with small sample sizes. Moreover, no study has been conducted so far to assess the prevalence and predictors of perceived stress in T2DM population of Nepal. Hence, there is a paucity of evidence on what factors influence stress mechanisms in T2DM patients in Nepal. Therefore, this study was undertaken to assess depressive symptoms and perceived stress among people with T2DM in Nepal, as well as to examine the associated socio-demographic and diabetes-related factors.
Methods
Study Design and Participants
This cross-sectional study used the baseline data of an overarching project, which was a prospective, community-based randomized controlled trial (RCT) of people with T2DM (30 years and above). The RCT examined the effectiveness of a culturally appropriate lifestyle intervention (using combination of community health workers, peer supporters, and regular telephone calls) in improving management and care of people with T2DM over 6 months postcluster randomization. A detailed description of the RCT is provided in its study protocol published elsewhere. 13 Ethical clearance of the overarching project was obtained from Human Research Ethics Committees (HRECs) of Nepal Health Research Council Nepal (#944/2019P), Kathmandu University Nepal, Tokyo Women’s Medical University Japan and Central Queensland University Australia (#CQU RSH/HE 0000022453). People (30 years and above) who were clinically diagnosed with T2DM, that is, with glycated hemoglobin (HbA1c) > 6.5% were eligible to participate in the study based on the American Diabetes Association and the World Health Organization (WHO) criteria for diagnosis and classification of diabetes.14,15
Procedures
Data were collected between September 2021 to February 2022 from a stratified random sample of 20 clusters (health facilities) from Kavrepalanchowk and 10 clusters from Nuwakot districts. Data were collected digitally from study participants and entered into KoboToolbox/Open Data Kit, which is a software used to collect, manage, and analyze data. KoboToolbox was preferred to reduce manual errors associated with paper-based data collection. To identify and recruit people with diagnosed T2DM into the study, available health registries of the randomly selected health centers in the districts were reviewed. Then, letters along with necessary description of the study were sent to those people with T2DM. Furthermore, an open invitation was sent to the health centers and communities, inviting the possible participants who may have had diagnosed or undiagnosed T2DM or felt they were at risk of developing T2DM. Hemoglobin test of people suspected of having T2DM was performed at the health centers. Then, all prospective participants, that is, those with HbA1c ≥ 6.5% completed the baseline assessments, including a survey questionnaire, anthropometric, and metabolic measurements. Hemoglobin of 92 participants recruited from the health registries were <6.5% after the HbA1c test but were included in the study as they already had T2DM diagnosis prior to their participation in the study. Verbal and informed written consent were taken from study participants prior to data collection. The sampling flowchart of the study is presented in Figure 1.
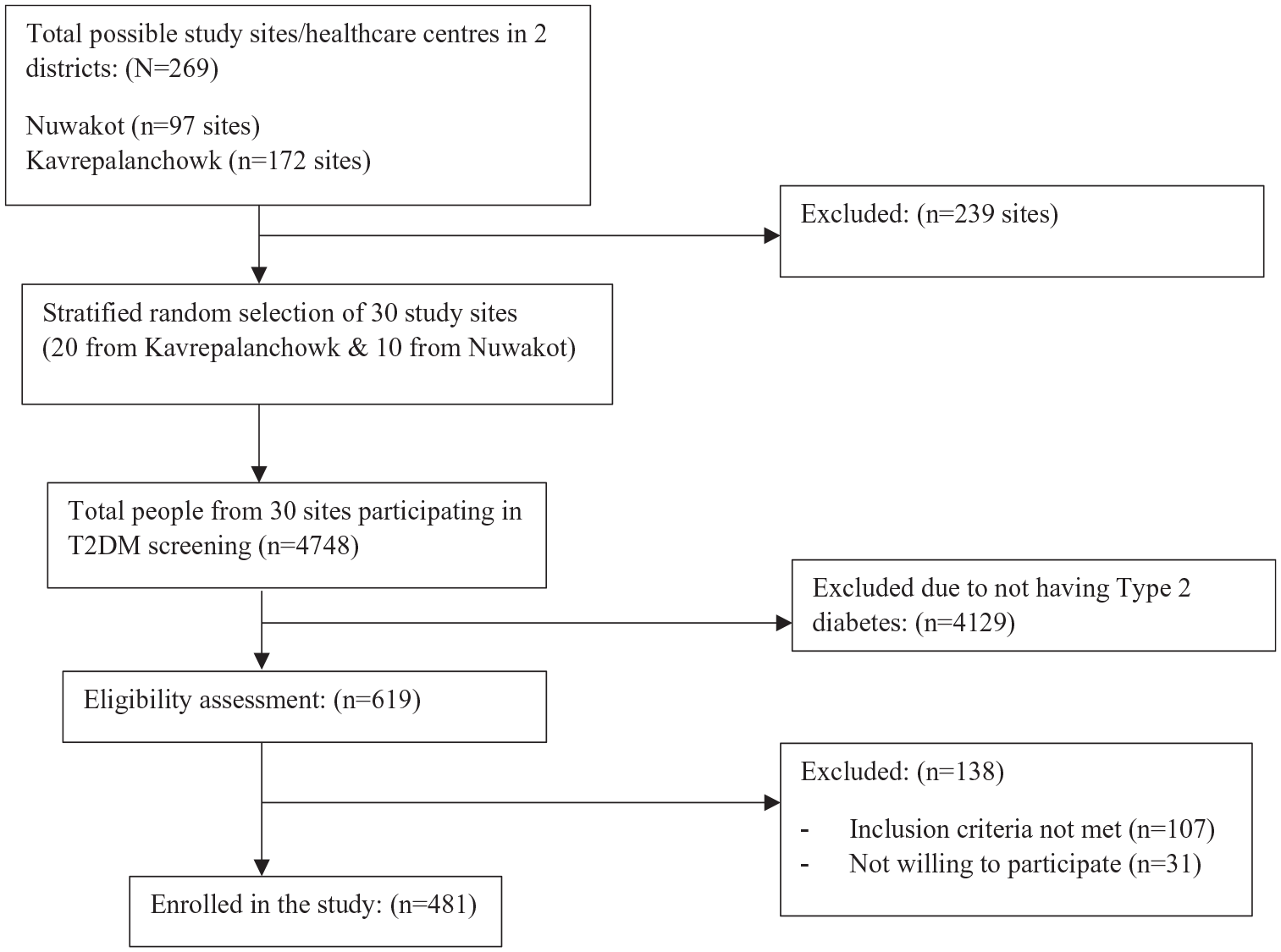
Sampling flowchart of the study.
Measurements
A structured questionnaire was prepared to collect required data for the study. The status of depressive symptoms was assessed using a validated and Nepali-translated screening and diagnostic tool for depressive symptoms, the Patient Health Questionnaire (PHQ-9). 16 Patient Health Questionnaire-9 has been used previously in Nepalese setting 12 and has shown a high internal consistency (Cronbach’s alpha 0.824) and a good convergent validity as demonstrated by a correlation of 0.75 with Generalized Anxiety Disorder-7 (GAD-7) and of 0.93 with Patient Health Questionnaire Anxiety-Depression Scale (PHQ-ADS) in a similar South Asian country, Bangladesh. 17 Patient Health Questionnaire-9 showed a high internal consistency in this study with a Cronbach’s alpha of 0.810. Depressive symptoms were categorized with PHQ-9 scores of 5, 10, 15, and 20 representing mild, moderate, moderately severe, and severe depressive symptoms, respectively. Participants with scores below 5 were categorized as not having any depressive symptoms, and those with the scores of 5 or above were classified as having some depressive symptoms, including mild symptoms. 16 Depressive symptoms were dichotomized as not having any depressive symptoms (PHQ-9 score <5) and having depressive symptoms (PHQ-9 score ≥5). Similarly, perceived stress was measured using a validated and Nepali-translated 10-item Perceived Stress Scale (PSS-10), which is used to understand the degree to which, one appraises situations in their life as stressful. 3 The tool has shown a good reliability with Cronbach’s alpha 0.715 and construct validity (a significant and strong correlation of 0.58 between the scores of PSS-10 and General Health Questionnaire, GHQ-28) when used in South Asian population. 18 PSS-10 showed an acceptable internal consistency with a Cronbach’s alpha of 0.691 in this study. Each question was scored as 0 = never, 1 = almost never, 2 = sometimes, 3 = fairly often, and 4 = very often, except for questions 4, 5, 7 and 8 for which the scores were reversed. Individual scores on the PSS-10 can range from 0 to 40 with scores ranging from 0 to 13 representing low stress, 14 to 26 moderate stress, and 27 to 40 high perceived stress. 3 Perceived stress was dichotomized combining moderate and high perceived stress to create a single variable.
Adherence to diabetes medication was measured using a reliable and valid eight-item Morisky Medication Adherence Scale (MMAS). Scores of <6, 6 to <8, and 8 represented low, medium and high medication adherence, respectively. 19 Similarly, physical activity level was assessed using the Global physical activity questionnaire (GPAQ). 20 Moderate to vigorous physical activity for 150 minutes per week was considered the cut-off value for meeting the recommendations. 20 Hypertension was established by a health care professional when the blood pressure reading in the sphygmomanometer was 130/80 mm Hg or higher. Hemoglobin was assessed using a sensitive point-of-care testing (POCT) analyzer (SDA1c Care) by a trained lab assistant. An HbA1c of 7% or more was considered uncontrolled HbA1c and lower than 7% was considered controlled HbA1c level. 14 Anthropometric measurements were taken, and body mass index (BMI) was calculated following the WHO BMI criteria for Asian classification. 21 A BMI of <18.5 kg/m2 was classified as “underweight,” 18.5 to 22.9 as “normal weight,” 23 to 24.9 as “overweight” and ≥25 as “obese.” 21 All instruments used to measure the independent variables in this study have been validated in similar settings like Nepal. A detailed information on their psychometric properties is reported in the study protocol. 13 The survey questionnaire was revised to best fit in Nepalese context and translated into Nepali language. Pretesting of survey questionnaire was done prior to collecting baseline data. Upon necessary revision after the pretesting, the questionnaire was then back translated to English by two independent translators.
Sample Size
A sample size calculation was performed considering depressive symptoms as a primary outcome. The sample estimation method was based on effect size (adjusted R-squared value) and was computed using STATA. Assuming the proportion of diabetic people with depressive symptoms in Nepal as 40.3%, and the adjusted R-squared value of the statistical model in the study as 0.40, as reported in a previous study, 22 and considering the 21 independent variables of which we wanted to assess the association with the study outcome, a sample size of at least 432 was estimated. Assuming a nonresponse rate of 10%, at least 480 participants were required in this study.
Data Analyses
Data analyses were performed using STATA version 18.0. The prevalence of depressive symptoms and perceived stress were reported as proportions. Descriptive statistics were presented as frequency, percentage, mean, and median. To identify the socio-demographic and diabetes-related factors independently associated with depressive symptoms and perceived stress, multivariable logistic regression analysis was run accounting for clustering effect after adjusting for the independent variables associated with the outcome variables (with P ≤ .20) in the bivariate analyses. Independent variables were tested for multicollinearity using variance inflation factor (VIF). The highest VIF was 2.2, hence no multicollinearity was detected. Adjusted odds ratios along with 95% CIs were computed. The goodness of fit of the statistical model was assessed by the Hosmer-Lemeshow test.
Results
Characteristics of Study Participants
A total of 481 participants with new or established diagnosis of T2DM were enrolled in the study. Table 1 illustrates the socio-demographic and diabetes-related characteristics of the participants. Just over half (53%) of the participants were female. The mean ± SD age was 54 ± 9.41 years. Most of the participants (59%) had gained formal education. A large proportion of participants (42%) relied on agriculture/animal husbandry as their source of income and 43% had a monthly income of NRs 10 000 to 25 000 (USD 86.2-215.5). Half of the participants (50%) had one or more comorbidities associated with T2DM, the most common of which were hypertension, hypercholesterolemia, and heart problems. Around 65% had no family history of T2DM, and time since diagnosis was 5 years or less for 63% of participants. Most of the participants (82%) was taking oral hypoglycaemic agents (OHAs) as their mode of treatment and 45% had a high adherence to T2DM medication. In terms of behavioral characteristics, 28% of the participants used tobacco products, 23% consumed alcohol, 80% performed moderate to vigorous physical activity for at least 150 minutes per week, 32% had their HbA1c level checked in the past 6 months, and 2% had their feet examined in the past year. Nearly half (45%) of the participants had hypertension, 67% had uncontrolled HbA1c (≥7), and 83% were either overweight or obese.
Characteristics of the Study Participants.
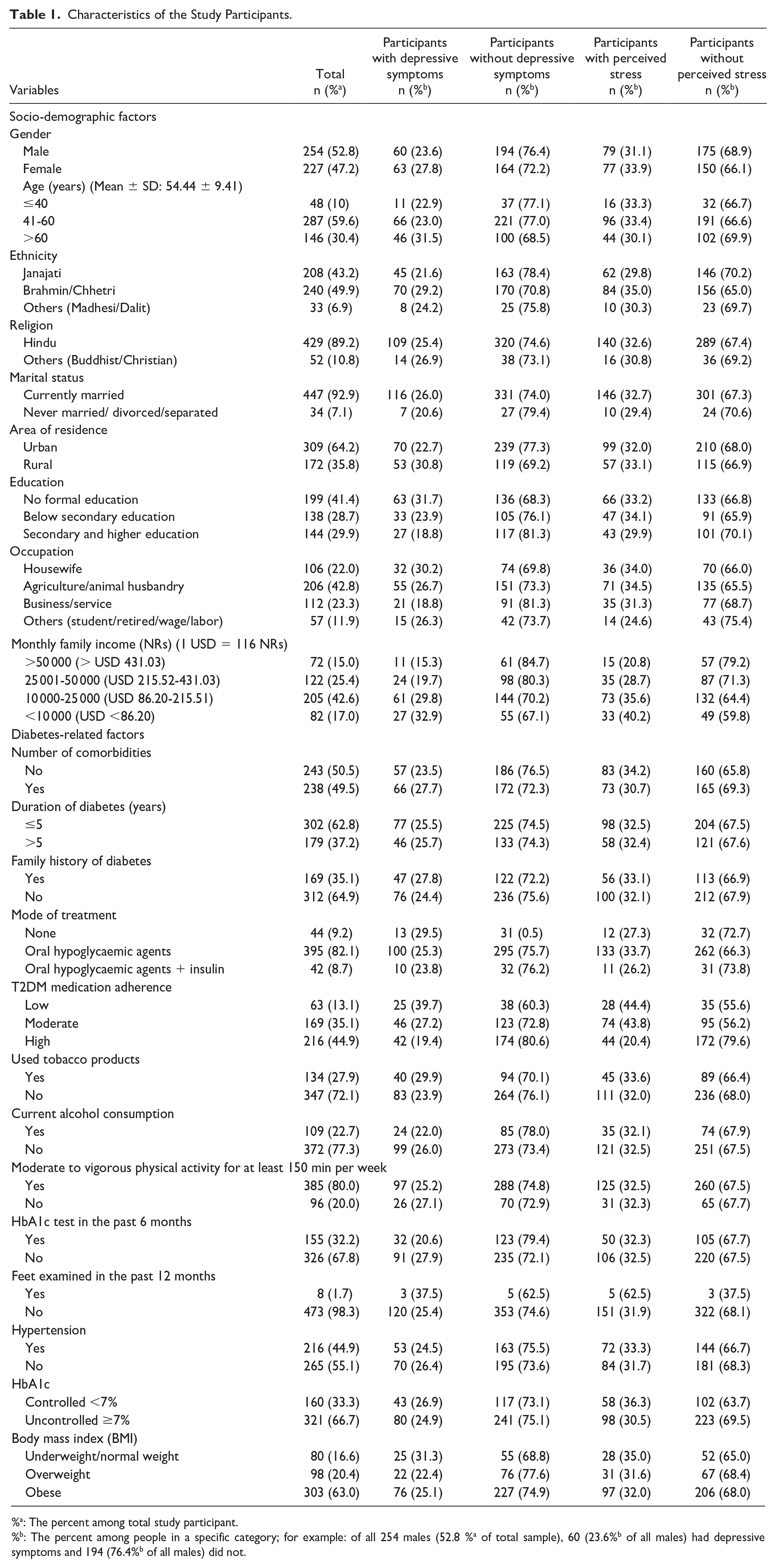
%a: The percent among total study participant.
%b: The percent among people in a specific category; for example: of all 254 males (52.8 %a of total sample), 60 (23.6%b of all males) had depressive symptoms and 194 (76.4%b of all males) did not.
Prevalence and Severity of Depressive Symptoms and Perceived Stress
The mean percentage of participants who had depressive symptoms was 25.8% (PHQ-9 score ≥5) with most of them having mild symptoms. Similarly, 32% of the study participants experienced perceived stress, with most of them experiencing moderate level of stress (see Supplemental Table).
Factors Associated With Depressive Symptoms and Perceived Stress
The adjusted logistic regressions showed that monthly income and T2DM medication adherence of the study participants were significantly associated with both outcome variables, depressive symptoms (Table 2) and perceived stress (Table 3). People having a monthly income of less than NRs 25 000 (<USD 215.52) were almost three times more likely to have depressive symptoms (aOR = 2.58, 95% confidence interval [CI]: 1.36-4.87) and twice more likely to have perceived stress (aOR = 2.34, 95% CI: 1.09-5.07) than those having a monthly income of >NRs 50 000 (>USD 431.03). Similarly, people with low adherence to T2DM medication were three times more likely of having depressive symptoms (aOR = 2.72, 95% CI: 1.33-5.59) and perceived stress (aOR = 3.03, 95% CI: 1.42-6.47) than those with high adherence. Moderate adherence to T2DM medication also increased the odds of having depressive symptoms by two times (aOR = 1.73, 95% CI: 1.04-2.89) and perceived stress by three times (aOR = 3.18, 95% CI: 1.97-5.14) compared to those with high adherence.
Factors Associated With Depressive Symptoms Among Study Participants.
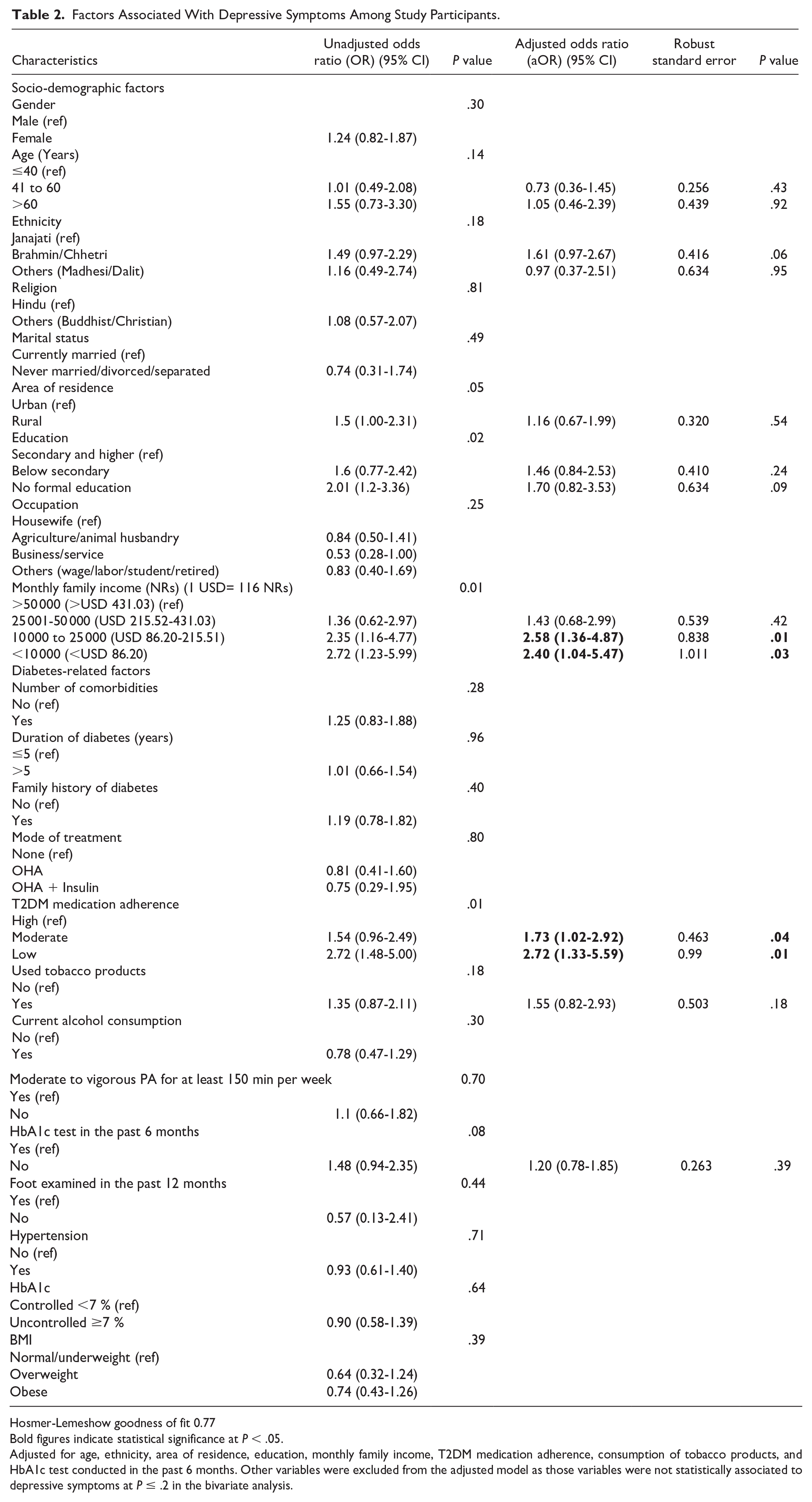
Hosmer-Lemeshow goodness of fit 0.77
Bold figures indicate statistical significance at P < .05.
Adjusted for age, ethnicity, area of residence, education, monthly family income, T2DM medication adherence, consumption of tobacco products, and HbA1c test conducted in the past 6 months. Other variables were excluded from the adjusted model as those variables were not statistically associated to depressive symptoms at P ≤ .2 in the bivariate analysis.
Factors Associated With Perceived Stress Among Study Participants.
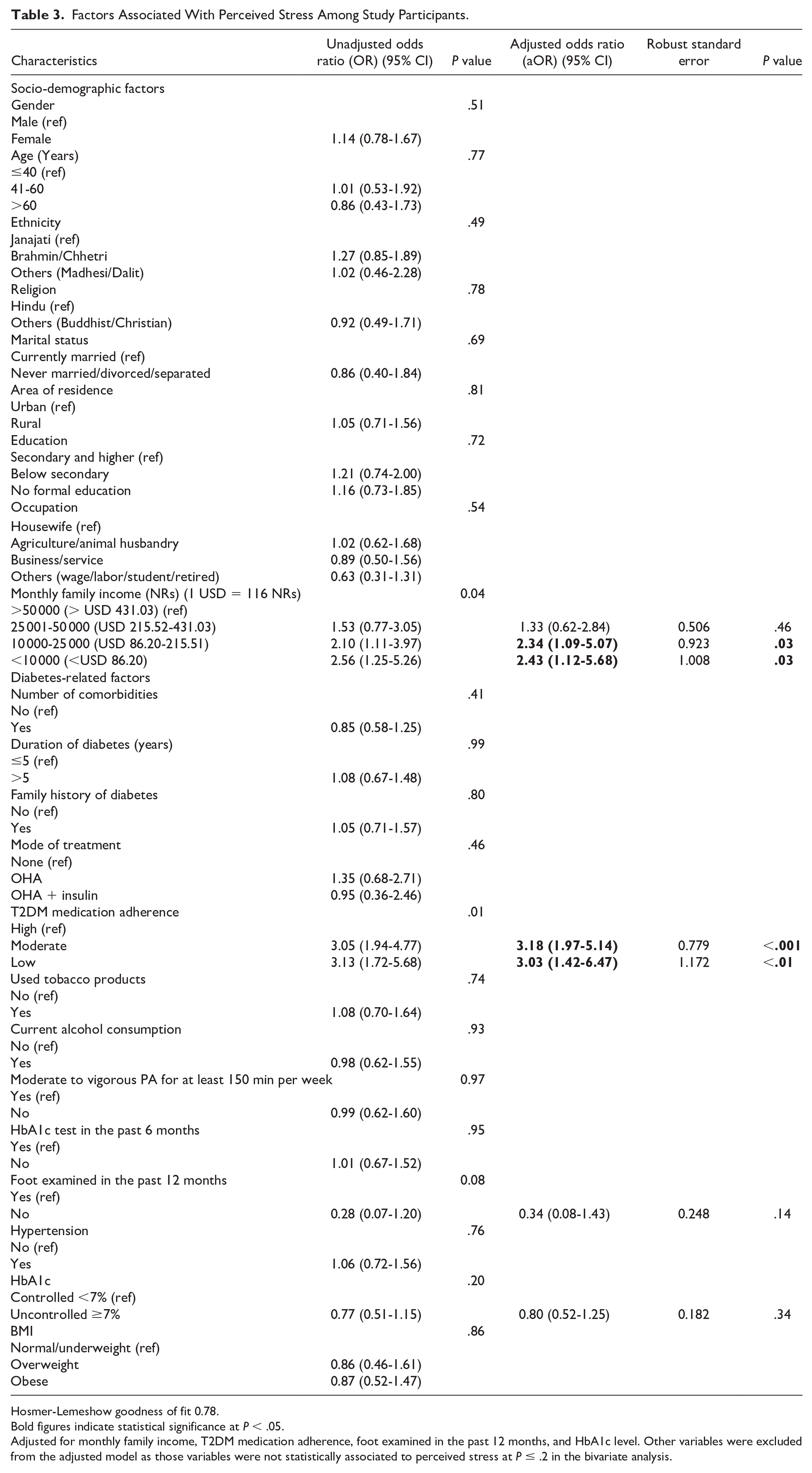
Hosmer-Lemeshow goodness of fit 0.78.
Bold figures indicate statistical significance at P < .05.
Adjusted for monthly family income, T2DM medication adherence, foot examined in the past 12 months, and HbA1c level. Other variables were excluded from the adjusted model as those variables were not statistically associated to perceived stress at P ≤ .2 in the bivariate analysis.
Discussion
The study findings revealed that more than a quarter of the study participants had depressive symptoms, and nearly one-third had perceived stress, mostly of mild to moderate severity. The results are consistent with a previous review that found a pooled prevalence of 27.7% of depressive symptoms among people with T2DM in Southeast Asia 23 and another study conducted in South India that found perceived stress in 39% of people with T2DM. 7 However, our study reported a lower prevalence of depressive symptoms in people with T2DM in Nepal compared to a study by Mishra et al 12 (54%) conducted in Nepal and by Aschner et al 24 (36.6%) conducted in 21 developing countries. The study also reported a higher level of depressive symptoms compared to a study by Sunny et al 11 (22.7%). These differences in prevalence of depressive symptoms may be attributed to varying study settings within Nepal and the use of different instruments such as Beck Depression Inventory 11 for measuring depression/depressive symptoms. To our knowledge, this is the first study to examine the prevalence and associated socio-demographic factors of perceived stress among people with T2DM in Nepal.
People with a low family income were more likely to develop depressive symptoms and have high perceived stress. This finding corroborates studies conducted in India, 7 Nepal, 11 and Nigeria. 25 The diagnosis of T2DM is burdensome, especially to people with low earning power as it requires them to face the twin burdens of meeting the everyday need of their family and paying for T2DM treatment costs. 25 The increased burden of the disease and the never-ending daily management associated with it can cause psychological pressure among people with T2DM, more so if they belong to a low-income group. Type 2 diabetes mellitus is associated with “catastrophic health expenditure” in Nepal, as a result, high treatment and management costs coupled with limited knowledge and awareness of self-management could take a psychological toll, especially on low-income people. 26 Furthermore, comorbid depressive symptoms could result in increased financial burden of treatment costs, further triggering psychological stress. 27
Poor T2DM medication adherence was significantly associated with having depressive symptoms and perceived stress in our study participants. Our findings are supported by previous studies examining medication adherence in people with T2DM conducted in similar low-income setting such as Ethiopia 28 and Palestine. 29 Type 2 diabetes mellitus patients with depressive symptoms are likely to pay lesser effort on daily self-care behaviors including medication adherence than those without depressive symptoms. 29 However, it is unclear whether poor medication adherence in itself could drive the development of depressive symptoms or stress in people with T2DM. Medication adherence is critical to the effectiveness of T2DM management and to stop the progression of the condition. When people with T2DM fail to adhere to their medication regimen, it might deteriorate their glucose metabolism, upsurge health care expenditure and the possibility of hospitalization due to requiring further treatment, and consequently trigger fear, psychological stress, and depressive symptoms. 30 Lack of patient awareness on importance of medication adherence and limited professional support from health care personnel during hospital/diabetes clinic visits may be predictors of medication nonadherence among people with T2DM. 28 Hence, strengthening health education and support systems is crucial to encourage people with T2DM to adhere to their prescribed medications for optimum management of their comorbid situation.
This study has several strengths. First, this study has a relatively larger sample size compared to other studies conducted in Nepal (e.g., n = 278, 11 n = 157 12 ). Second, this is the first study to assess the prevalence and socio-demographic factors associated with perceived stress in people with T2DM in Nepal. Third, we have used validated and reliable tools such as PHQ-9, PSS-10, MMAS, and GPAQ in this study. However, there are also limitations to this study. First, the findings from this study might not be generalizable among wider population groups across the country, as the sample was not representative of people with T2DM in all of Nepal. Second, no causal inferences could be derived from the study due to a cross-sectional nature of the study. Third, the responses from participants might be subject to social desirability bias due to the use of self-reported questionnaires. Participants with both new and established diagnosis of T2DM were included in the study. The mental health of those living with T2DM for years may vary greatly from those diagnosed recently. This heterogenous inclusion of participants warrants cautious interpretation of our study findings. Last, since the study was conducted during the time when Nepal was still going through COVID-19, the observed prevalence of depressive symptoms and/or perceived stress might have been influenced by the effect of the pandemic.
Conclusion
This study revealed that a quarter of participants with T2DM had depressive symptoms and a third experienced perceived stress of varying severity in Nepal. Low monthly income and poor diabetes medication adherence were significantly associated with both mental health outcomes among the study participants. Routine primary care of T2DM patients should encompass mental health screening and treatment to prevent further complications. Likewise, efforts to improve medication adherence should be incorporated in the routine clinical practice. Moreover, person-centered care addressing the socio-economic situation of people living with T2DM should be prioritized by health care providers and the health care system as a whole. Further studies with larger sample sizes are recommended to investigate the associated socio-demographic and diabetes-related factors of depressive symptoms and perceived stress among larger population groups with T2DM in Nepal. More detailed research is required to gain a deeper understanding on the association between income and T2DM comorbid with mental health problems. Understanding this association could inform the delivery of a person-centered T2DM management strategy, especially targeting the low-income population groups of the country, and would be key to the success of prevention efforts. Longitudinal research is needed to better understand the risk factors for these mental health conditions among people with T2DM. Qualitative studies are recommended as they can help obtain valuable perspectives for designing and implementing effective multidisciplinary and integrated strategies to the management of T2DM and mental health comorbidity. The findings from this study can be used to inform the design and implementation of low-cost, community-based, culturally appropriate, and locally tailored intervention approaches to address mental-health-related needs of people with T2DM in Nepal at different tiers of health care.
Supplemental Material
sj-docx-1-aph-10.1177_10105395241277892 – Supplemental material for Depressive Symptoms, Perceived Stress, and Associated Socio-Demographic and Diabetes-Related Factors in People With Type 2 Diabetes in Nepal
Supplemental material, sj-docx-1-aph-10.1177_10105395241277892 for Depressive Symptoms, Perceived Stress, and Associated Socio-Demographic and Diabetes-Related Factors in People With Type 2 Diabetes in Nepal by Ashmita Karki, Corneel Vandelanotte and Lal B. Rawal in Asia Pacific Journal of Public Health
Footnotes
Author Contributions
AK conceptualized the study under the supervision of LR and CV. The project research assistants collected the data. AK conducted data cleaning and analysis. AK drafted the manuscript. LR and CV reviewed the manuscript and provided substantial feedback. AK, LR, and CV refined the manuscript, and AK prepared the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian Government Research Training Program (RTP) Scholarship.
Data Availability
The data that support the findings of this study are available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.