
Abstract
Background
People with type 2 diabetes mellitus (DM) are at risk of experiencing depression, which in turn can affect their selfcare activities. Recent evidence has shown that social support is beneficial in reducing the risk of depression and positively affecting increases in self-care activities. However, the role of social support in the relationship between depressive symptoms and selfcare activities has not been studied. This study aims to determine the mediating effects of social support on the relationship between depressive symptoms and self-care activities of people with type 2 DM.
Design and methods
A cross-sectional consecutive sampling approach was used with 94 respondents with type 2 diabetes in East Jakarta, Indonesia, who were undergoing diabetes treatments during May–June 2020. The instruments used were the Centre for Epidemiologic Studies-Depression Scale, Summary of Diabetes Self Care Activities and Duke-UNC Functional Social Support Questionnaire. All three questionnaires have been tested for validity and reliability. Data analysis was carried out using multiple linear regression, path analysis, and the Sobel test.
Results
The results of multiple linear regression analysis on the variables age, sex, education level, socioeconomic status, duration of type 2 DM, and complications of type 2 DM showed that only complications of type 2 diabetes affected self-care activities (p=0.000; R2=0.515). The results of the path analysis and Sobel test showed that social support significantly mediated the effects of the relationship between depressive symptoms and selfcare activities (z=-0.162 > table 1.96; direct effect = -0.499; indirect effect = -0.0789; total effect = 40.3%).
Conclusions
Screening for depressive symptoms and interventions involving social support are strongly suggested for patients with type 2 DM who are suspected of showing a decline in self-care activities.
Introduction
Diabetes mellitus (DM) is a chronic disease and the main cause of morbidity, disability, and death, with diagnoses steadily increasing every year. 1 The World Health Organization's Global Report on Diabetes of 2013 showed that the prevalence of diabetes mellitus was 382 million people, increasing to 422 million people in 2014. It is estimated that the prevalence will continue to grow to 592 million people by 2035, particularly in developing countries such as Indonesia.2,3 The majority of diabetic patients have type 2 DM, which is also the main cause of macro-vascular and micro-vascular complications for such patients.4–6 Diabetes mellitus type 2 is also the leading cause of death worldwide. 7
Significance for public health
This study suggests that social support mediates the effects of depressive symptoms on self-care activities in patients with type 2 diabetes mellitus (DM). Therefore, depression screening and the assessment of social support for each type 2 DM patient at risk of experiencing decreased self-care activities could be an effective intervention. The present study on the existence of social support as a factor increasing self-care activities in type 2 DM patients with depression symptoms can be used for reference and to provide information to public and educational institutions, including students, lecturers, and researchers.
Self-care efforts contribute significantly to reducing mortality and minimizing complications in diabetics. 1 Self-care activities include patient participation in continuous self-management through diet, foot care, physical exercise, and blood glucose monitoring. 8 However, it is undeniable that self-care activities have an influence on patients’ lifestyle and financial or economic changes. 9 However, diabetic patients have been shown to be prone to depression due to the high financial costs of self-care and ongoing fears of life-threatening risks, such as complications and premature death.
Individuals with diabetes and depressive symptoms have been shown to be two to three times more likely to have lower adherence to self-care activities than those without depressive symptoms. 10 Therefore, the role of social support is in the improvement of self-care for type 2 DM patients. Recent research has discussed the role of social support in self-care activities, showing that a higher level of social support is associated with increased self-care activities in type 2 DM patients, including glycemic control.11,12 Additional research has shown the involvement of social support regarding levels of self-care activities in type 2 DM patients experiencing depression to be highly significant. The results of the regression analysis in the present study showed that low social support was the greatest factor affecting individuals experiencing depression. 13
The prevalence of people with diabetes mellitus increases every year, including in Indonesia. Good diabetes management, including good glycemic control with minimal complications, is expected to improve clinical outcomes. Although several studies have reported poor glycemic control as a significant factor in high complication rates caused by non-adherence to self-care activities, the causes of the decline of self-care activities have rarely been explored. Patients with type 2 DM are also at risk of depression. Type 2 DM patients with depressive symptoms are two to three times more likely to have lower medication adherence and selfcare activities compared to those without depressive symptoms. Research on depressive symptoms has suggested that higher levels of depressive symptoms are significantly associated with lower levels of self-care activities. Furthermore, existing studies have shown that the role of social support can increase self-care activities and reduce the risk of depression. Based on this, depressive symptoms are clearly affected by self-care activities and social support, with a decrease in depressive symptoms closely related to an increase in self-care activities. Therefore, this study aims to determine the mediating effects of social support in the relationship between depressive symptoms and self-care activities in patients with type 2 DM.
Design and Methods
The design of the study was cross-sectional, including a consecutive sampling technique involving 94 respondents in East Jakarta, Indonesia, who had a medical diagnosis of type 2 DM and who were still undergoing treatment during May–June 2020. The research data was collected through an online questionnaire during that same period. The questionnaires used were the Center for Epidemiologic Studies-Depression Scale (CES-D), Summary of Diabetes Self Care Activities (SDSCA), and Duke-UNC Functional Social Support Questionnaire (DUFSSQ), which have proven validity and reliability.
The Center for Epidemiological Studies-Depression Scale (CES-D) instrument developed by Lewinshon has been standardized and is recognized as being applicable for health research worldwide. 14 The results of the validity and reliability test in 1233 obtained a value of 0.90. 14 The Indonesian version of the Center for Epidemiological Studies-Depression Scale (CES-D) instrument has also been tested for validity and reliability by Kusuma. 15 The results of research conducted by Kusuma found that all questionnaire questions from the Center for Epidemiological Studies- Depression Scale (CES-D) had a score above the r table value (0.169). The results of the reliability test using Cronbach's alpha obtained an alpha value of 0.986. The results of the retest test in this study using the Spearman's rank correlation obtained a correlation coefficient value of r = 0.358-0.828. 15
The instrument Summary of Diabetes Self-Care Activities (SDSCA) is a questionnaire developed by Toobert. 16 The results of the study on the SDSCA instrument showed that majority of participants diagnosed with type 2 diabetes mellitus with an age range of 45 – 67 years. The SDSCA instrument is capable of measuring diabetes self-management in multiple dimensions (7 dimensions) with adequate internal reliability result and test-retest reliability and has evidence of validity and sensitivity to change. The results of validity test on correlation between item score and total score of Toobert research showed the value of r=0.47 and Cronbach's alpha 0.618. The test-retest in this study using the Spearman's rank correlation obtained a correlation coefficient value of r=0.469-0.709. The Cronbach's alpha value in this study was 0.980.
The Duke-UNC Functional Social Support Questionnaire (DUFSSQ) is an instrument used to measure the amount and type of received emotional social support. 17 The results of the psychometric properties of internal consistency reliability test using Cronbach's alpha on the DUFSSQ questionnaire obtained an alpha value of 0.80, the test-retest using Spearman's rank correlation obtained a correlation coefficient of r=0.50-0.77. 18 The Bahasa version of the DUFSSQ questionnaire was yet to exist so that researchers will carry out the process of translating (translate – back translate), testing validity, and reliability in accordance with the test rules that have been set. The test-retest in this study using the Spearman's rank correlation obtained a correlation coefficient value of r = 0.629-0.771. The Cronbach's alpha value in this study was 0.834.
Univariate, bivariate, multivariate, and path analyses were conducted using SPSS version 21. The univariate analysis aimed to analyze demographic characteristics (gender, education, occupation, economic status, complications, age, and duration of type 2 DM illness), categories of depressive symptoms, social supports, and self-care activities. Bivariate analysis was used to determine the relationship between demographic characteristics and self-care activities. Path analysis was used to analyze the cause-effect relationship on two types of variables – direct effect (of depressive symptoms on self-care activities) and indirect effect (of depressive symptoms on self-care activities through social support.
Demographic characteristics of respondents (n=94).
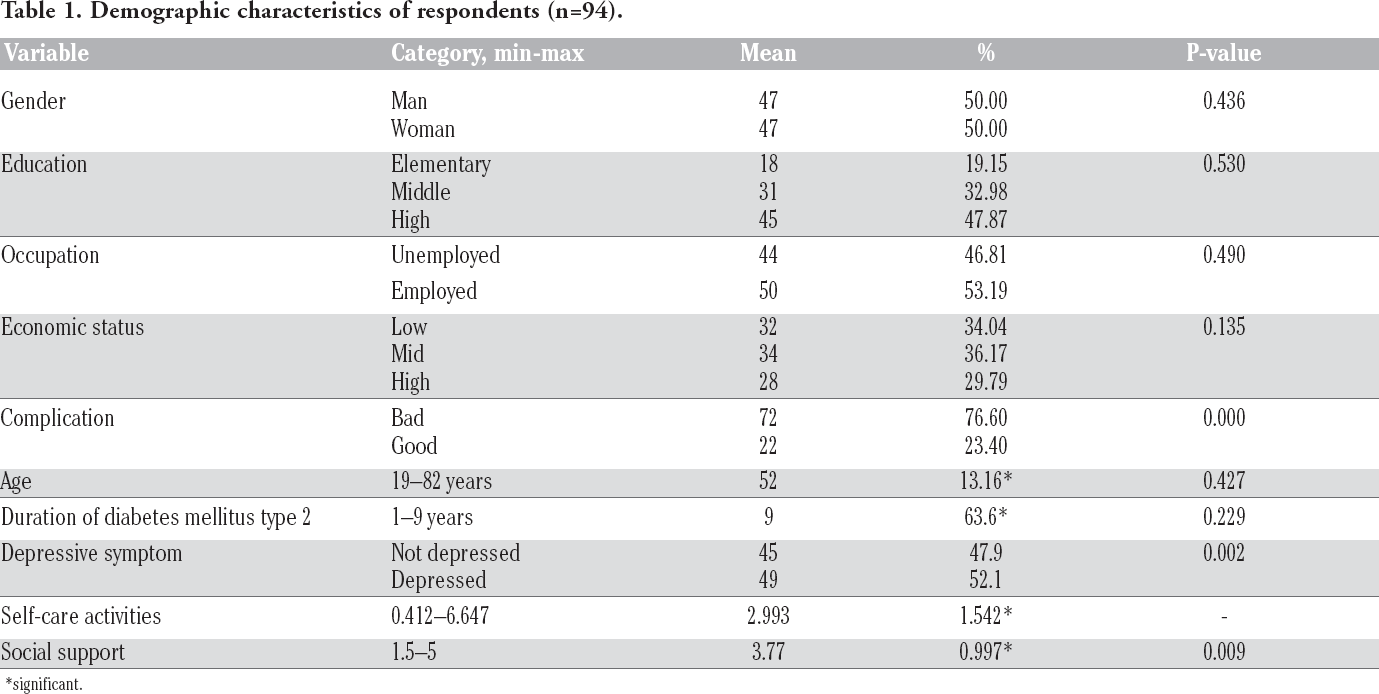
significant.
Results
The proportions of sexes of the respondents were comparable, with 50% male participants and 50% female participants. Most respondents (47.87%) had high levels of education, 53.19% were employed, and 76.60% suffered serious complications. Most of the respondents’ economic status (36%) was within the medium category. The average age of the respondents and the length of illness were 52 years and 9 years, respectively. Most of the respondents (52.1%) indicated having depressive symptoms, while the mean level of self-care activity was 2.993 (SD 1.542), and the mean level of social support was 3.77 (0.997) (Table 1).
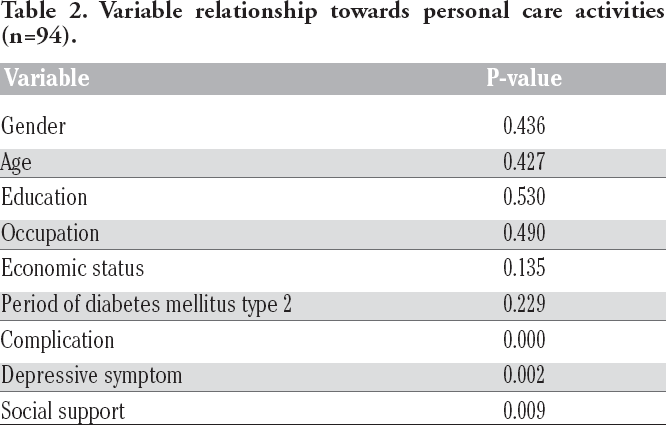
The results of the bivariate analysis (Table 2) showed that there was no association between confounding variables (gender, age, education level, socioeconomic status, and duration of illness) and self-care activities, except regarding complications of type 2 diabetes (p=0.000; 95% CI). Additionally, there was a relationship between self-care activities and both depressive symptoms (p=0.002; 95% CI) and social support (p=0.009; 95% CI).
The results of the multivariate modeling test showed that experiencing type 2 DM complications was the confounding variable that most significantly influenced the risk of declining self-care activities in type 2 DM patients. This was proven through the coef B value of -2.722, which indicated that each unit increase in the complications’ variable reduced a participant's ability to carry out self-care activities by 22.722. The p-value of 0.000 and R 2 of 0.515 indicated that the level of the relationship between complications and self-care activities was highly significant, with complications of type 2 DM influencing self-care activities by 51.5%.
Figure 1 shows the relationship between the following variables: depressive symptoms, social support, and self-care activities. The correlation coefficient between depressive symptoms and social support was -0.288, indicating that an increase in social support would further reduce depression symptoms, and vice versa. The correlation coefficient between social support and self-care activities was valued at 0.418, indicating that improved social support positively affects self-care activities, and vice versa. The correlation coefficient between depressive symptoms and self-care activities was -0.578, indicating that an increase in depressive symptoms will lead to a decrease in self-care activities, and vice versa.
Table 3 describes the results of sub-structure-1with the following coefficient equation of the effect of depressive symptoms on social support:

The equation can be interpreted as follows: the path coefficient of the effect of depression symptoms on social support was 0.288 or 8.3% with a significant negative effect (p=0.005).
Table 4 describes the results of the sub-structure-2 with the coefficient of depressive symptoms and social support for self-care activities equation as follows:

The equation can be interpreted that the effect of depressive symptoms on self-care activities is 0.499 or 24.9% with a significant negative effect (p=0.000), while the effect of social support on self-care activities is 0.274 or 7.5% with a significant positive effect (p=0.002).
The results shown in Figure 2 and Table 5 indicate that depression symptoms and social support have a significant effect on selfcare activities with a total value of 0.403 or 40.30%.

Correlation coefficient between variables (n=94). X = depressive symptoms; Y = social support; Z = self-care activities.
Variable relationship towards personal care activities (n=94).
Sub-structure-1 path coefficient of depression symptoms on social support (n=94).

a. Dependent variable: social support (Y).
The Sobel test in this mediation model showed the significant mediating effect of social support on the relationship between depressive symptoms and self-care activities (z=-0.162 >t table 1.96).
Discussion
Based on the result of the study, the relationship between gender and self-care activities are not significant and this is aligned with previous research which states that men and women have a tendency to perform adequate self-care hence they are indifferent. 19 The result also shows a significant relationship between gender and dietary practice where men have 0.328 times worse practice of type 2 DM diet than women taking into account age, education, occupation, and self-efficacy variables. 20
The proportion in this study is similar with previous studies which showed that people from age group >50 years have an increase of 5-10 mg/dL per year. 21 Statistics show no relationship between age and self-care activities. The results of this study are in line with previous research which described that age is not related to the ability to perform self-care activities. 22 However, there are also other research that showed different results wherein the variables of self-care and age have a significant inverse relationship – the higher the age, the lower the ability to perform self-care activities. 12
Researchers believe that the reason for no relationship found between age and self-care activities in this study was because more than 50% of respondents who participated had experienced complications of type 2 diabetes. This is in accordance with previous theory where older DM patients are at risk for complications or comorbidities which cause declining physical function to a point where self-care activities cannot reach optimal levels. 23 On the other hand, younger respondents may still spend most of their focus on their job so that diabetes self-care activities cannot be carried out optimally. The results of the study also showed that age difference was not a significant factor in performing self-care activities as older DM patients already possess the experience of self-care activities and have perceived bigger benefits so that they always strive to carry out the activities. 24 Meanwhile younger DM patients find it easier to explore information about the disease based on up-to-date information so they have good knowledge about diabetes self-care and try to apply it in their daily lives.
The distribution of people with type 2 diabetes mellitus by education level is different with data from Infodatin which stated that people with type 2 diabetes tend to be in groups of lower education level. 25 Statistics show no relationship between education level and self-care activities. These results are not in line with previous research which described low education level has significant correlation to poor self-care. 26
Sub-structure-2 path coefficient of depressive symptoms and social support on self-care activities (n=94).

a. Dependent variable: self-care activities.
Direct and indirect effects of variable X on variable Y.

Total effect of X and Y towards Z.

Combining sub-structure-1 and sub-structure-2 models.
The education level determined in this study was formal education achieved by individuals which could not precisely describe participants’ level of knowledge on type 2 DM management. Meanwhile research by Kassahun et al. used a questionnaire approach to measure respondents’ level of knowledge on type 2 DM management as the definition of the education level variable. 26 Formal education level is often loosely associated with level of knowledge. Although formal educations aimed to improve one's knowledge, it does not necessarily mean that individuals with low formal education level have limited knowledge as well.
The socio-economy status of most respondents belonged to the middle socioeconomic category. This is in accordance with past research where middle-income groups tends to be more susceptible to type 2 diabetes. 27 Analysis on the significance test between socio-economic status and self-care activities concluded that there was no relationship between self-care activities and socio-economic and employment status. This finding is not in line with results of previous research which described that there was a strong relationship between income levels and self-care on people with type 2 diabetes where individuals with high income have the ability to perform better self-care and vice versa. 28
The absence of a relationship between socioeconomic status and self-care activities in this study occurs because each type 2 DM patient actually has the ability to perform self-care and achieve a better quality of life in different ways. In the case of managing type 2 DM, patients with low income can take advantage of the health insurance provided by the government to gain access to health facilities for free. Meanwhile, individuals with higher income have more options to obtain health services they needed, either independently at home or in health care facilities.
Further statistical analysis showed no relationship between duration of having type 2 diabetes and self-care activities. This is not in line with previous studies which explained that type 2 diabetes patients with illness duration of more than 14.29 years are associated with higher levels of self-care. 28 Results from other study also showed that illness duration of type 2 diabetes is associated with increased self-care abilities. 29 The accumulated experience of various aspects of diabetic care coupled with frequent exposure to self-care education may be responsible for this finding. 30
Most of type 2 diabetes patients were known to possess macrovascular and/or microvascular complications. This condition is in line with the results of this study where most respondents have bad complications. The results also showed a relationship between complications of type 2 diabetes mellitus illness with self-care activities. Continuous self-care activities can delay or minimize the development of diabetes complications. 31 However, diabetic patients with complications often experience difficulties in carrying out their self-care activities due to physical and metabolic dysfunction.
Short-term impact of complications can trigger anxiety and depression as elevated blood glucose levels are linked to fatigue, sleep disturbances, and the risk of infection. Continuous exposure to this short-term impact can lead to long-term complications, such as limited body functions. Eventually the patient found it difficult to carry out daily activities optimally including self-care management of type 2 diabetes. 31
Most of respondents in this study are classified having depressive symptoms and this is in line with other research which stated diabetic patients are prone to experiencing depression that is about twice as higher as other individuals. 32 The results of the analysis indicated that there is a relationship between depressive symptoms and self-care activities and this is also in line with findings from previous studies which explain that depression has negative effect to the management of diabetes mellitus illness, such as medication adherence and self-care activities (diet, physical activity). 10
Statistics showed a significant relationship between social support and self-care activities. This was in line with existing research on the role of social support in self-care activities that shows how a higher level of social support is associated with increased selfcare activities and glycemic control in type 2 DM patients.11,12 However, other research has also stated that the effect of social support on self-care is moderate and considerably varied, depending on the type of diabetes, the majority of ethnicity in the sample, and the type of social support measures obtained by each individual. 31
There are several important ways relatives and families can support type 2 DM patients, including increasing patient awareness in recognizing their illness as uncurable. This can help patients gain greater awareness regarding managing their own disease, including undergoing routine treatment. 33
Multivariate test results showed that complications of type 2 DM were the most significant confounding variables influencing the risk of decreased self-care activities for type 2 diabetes mellitus patients. This was in line with existing studies that used multiple logistic regression design, wherein complications were statistically the most influential factors on self-care activities. 34 Results of previous studies have also suggested that patients with diabetic microvascular complications had more difficulties carrying out self-care activities, even though they realized the importance of controlling their diabetes. 35
The results of the path analysis indicated that social support as felt by type 2 diabetes patients had an important mediating role in reducing the negative effects of depressive symptoms on self-care activities. These results were corroborated by the results of a study by Salinero et al. which aimed to determine the prevalence of T2 DM, as well as to identify factors related to depression, such as socio-demographic, clinical, and psychological factors, with a large prospective cohort design for one year. 35 Some of the variables that were inversely associated with increased risk of depression included employment (OR 0.595; 95% CI), low self-care activities (OR 0.552; 95% CI), systolic blood pressure (OR 0.982; 95% CI), and social support (OR 0.978; 95% CI). On the other hand, variables that were in line with increasing depression were the presence of a history of depression (OR 0.648; 95% CI), neuropathy (OR 1.951; 95% CI), oral antidiabetic medication and insulin, gender, and cholesterol. It can thus be concluded that the level of depression could be reduced by increasing self-care activities and social support.
T2 DM is a disease that cannot be cured. Individuals diagnosed with this chronic disease are only able to control the progression of the disease so that they are prevented from experiencing fatal complications. Additionally, adjusting to the lifestyle necessary to manage type 2 diabetes is not easy and must be done continuously. This ultimately becomes the catalyst for the emergence of psychological problems, which can initially begin with anxiety and move to depression. Individuals with diabetes and depressive symptoms have been shown to be two to three times more likely to have lower adherence to medication and self-care activities than those without depressive symptoms.10,36
Based on this, social support plays an important role in diabetic patients’ management of their disease, especially their mental health. The results of the present study explain that the role of social support can increase self-care activities by 2.86 times or approximately 74%. 22 In addition, the results of the current research also showed that there was an inverse relationship between social support and coping, suggesting that increased social support is associated with decreased emotional distress. 37
Social support is a means of coping that can influence negative conditions such that it can change the emotional response of T2 DM patients with depression to the condition of their disease. Social support can come from individuals who are close to the patient, such as spouses, family members, friends, healthcare workers, and support groups within the community. Aspects of social support include providing motivation to patients to carry out treatments, providing support and information about the most recent developments in type 2 diabetes management, providing assistance when patients are sick, and providing positive reinforcement.
One of the instruments, namely the DUFSSQ, has not been translated into Bahasa and has never been used in domestic research. The present researcher tried to translate this tool into Bahasa, testing the validity and reliability, but did not perform back translation of the questionnaire. This opens up the possibility for different interpretations of each item in the questionnaire.
Conclusions
This study suggests that social support mediates the effects of depressive symptoms on self-care activities in patients with T2 DM. Therefore, depression screening and the assessment of social support for each type 2 diabetes mellitus patient at risk of experiencing decreased self-care activities could be an effective intervention. The present study on the existence of social support as a factor increasing self-care activities in type 2 diabetes mellitus patients with depression symptoms can be used for reference and to provide information to public and educational institutions, including students, lecturers, and researchers.
Footnotes
The authors declare no potential conflict of interest.