
Abstract
This study aimed to assess the utilization of health care services and its associated factors among people with type 2 diabetes mellitus (T2DM) in Nepal. Data on the utilization of health care services were assessed in 481 adults aged 30 to 70 years with T2DM in Nepal. Multiple logistic regression analysis was performed to determine the factors associated with the utilization of health care services. Over 6 months, 66.1% of participants visited health care facilities or health service providers, followed by specialist visits (3.5%), hospitalization (2.1%), and emergency department visits (1.9%). Visit to health care facilities was significantly higher among those aged 50 to 59 years old (ORA: 1.64), practicing Hinduism (ORA: 2.4), and earning NRs ≥30 000 (≥USD 226.10) (ORA: 1.82) as compared to those aged ≥60 years old, practicing other religions, and with monthly family income NRs ≤10 000 (≤USD 75.37), respectively. The utilization of health care services among people with T2DM in Nepal was reasonably low. Identifying the underlying causes of low use of health care services is of great importance to bridge the gap in using health care services for management of diabetes.
What We Already Know
Type 2 diabetes mellitus (T2DM) has significantly increased across the world, mostly in low- and middle-income countries in recent decades.
Existing evidence has shown that people with diabetes tend to visit physicians or health care providers, specialists, and emergency rooms more frequently than those without diabetes and are also more likely to be hospitalized.
What This Article Adds
Visit to health care facilities within the last 6 months was 66.1% among the people with T2DM living in rural and urban areas of Nepal. Visit to specialists, emergency departments, and hospital admission was generally low among the study participants.
Identifying the underlying causes of low use of health care services is of great importance to bridge the gap in the use of health care services and the management of diabetes.
Introduction
Diabetes mellitus is a chronic health condition that affects various organs leading to premature deaths and disability. 1 In recent years, the prevalence of diabetes among the adult population (20-79 years) in Nepal has increased from 488 200 in 2011 to 1.1 million in 2021. 1 The effective management of diabetes can delay or prevent life-threatening health complications such as cardiovascular diseases, neuropathy, nephropathy, and foot and eye-related diseases. 1
The utilization of health care services plays a significant role in managing type 2 diabetes mellitus (T2DM) by enhancing the interaction between health care providers and patients, thereby improving diabetes care and control. 2 However, the availability of diabetes-specific services through interprofessional collaboration between the service providers is not organized and uniform in Nepal. 3 The majority of diabetes services in Nepal are delivered by the private sector and are urban-centered. 3 Moreover, a systematic review from Nepal highlighted that the existing knowledge on the burden of diabetes, its treatment, and control is still insufficient in Nepal. 4 Insufficient services and resources for diagnosis, treatment, and prevention of diabetes at the primary health care level are major causes of higher disease burden in Nepal. 3
Understanding the health care service utilization among people with diabetes is an urgent priority to generate evidence-based recommendations to health authorities in countries like Nepal where diabetes services or resources are inadequate. Hence, the aim of this study was to assess the utilization of health care services and its associated factors among people with type 2 diabetes in Nepal.
Methods
Study Design and Participants
This study includes cross-sectional data from a randomized controlled trial (RCT) implemented in rural and urban communities of Nuwakot and Kavrepalanchowk districts of Nepal. The detailed methodology of the RCT has been published elsewhere. 5 In brief, this study uses baseline data, collected between July 2021 and February 2022, from the RCT, which has 481 participants at baseline. Those aged 30 to 70 years who were clinically diagnosed with T2DM were enrolled in the study.
Study Measures
Measure of dependent variable
The utilization of health care services among people with type 2 diabetes was assessed by asking the participants if they had visited (1) a physician or health facility, (2) an emergency department, (3) a specialist visit, and (4) if they were hospitalized due to the complications of type 2 diabetes during the last six months. The answers to all the primary outcome variables were categorized as “No” and “Yes” for the logistic regression analysis; however, all the continuous findings are reported in the descriptive findings in Table 1.
General Characteristics of Study Participants and Health Care Service Use by Gender.
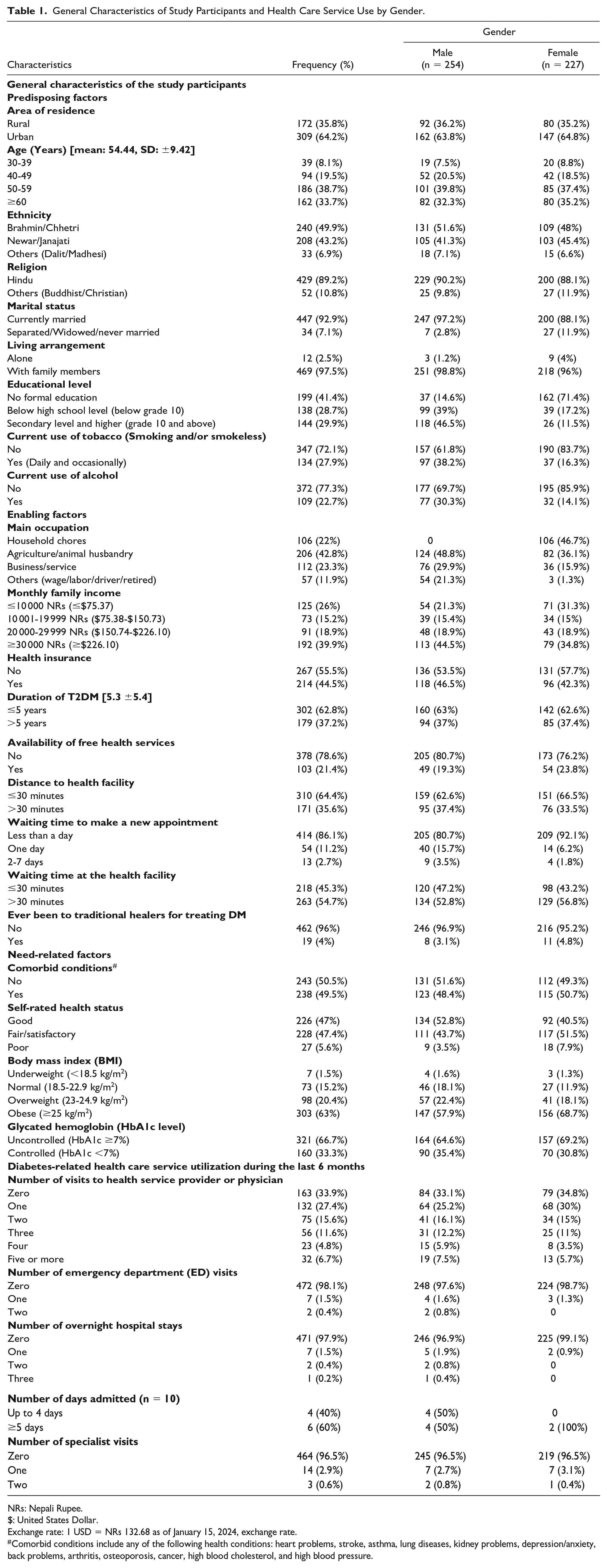
NRs: Nepali Rupee.
$: United States Dollar.
Exchange rate: 1 USD = NRs 132.68 as of January 15, 2024, exchange rate.
Comorbid conditions include any of the following health conditions: heart problems, stroke, asthma, lung diseases, kidney problems, depression/anxiety, back problems, arthritis, osteoporosis, cancer, high blood cholesterol, and high blood pressure.
Measure of independent variable
Several independent variables were identified through a review of the literature and were categorized into predisposing, enabling, and need of care factors adapting the Andersen Behavioral Framework for Health Service Utilization. 6 In the model, predisposing factors refer to the sociodemographic characteristics such as age, gender, ethnicity, religion, marital status, education, and living arrangements; enabling factors refer to services or resources that facilitate the use of the services such as occupation, income, health insurance, availability of free health care services, distance to the health facility, and waiting hours; and need factors refer to physical condition and disease characteristics that motivate service use, which includes comorbid conditions, self-rated health status, body mass index (BMI), and glycated hemoglobin (HbA1c).
Statistical Analysis
Data analysis was performed using the IBM SPSS version 23. Multivariate logistic regression was performed to identify the variables associated with visits to health care facilities or service providers during the last 6 months. Visits to specialists, emergency departments, and hospitalization were very low, and therefore not analyzed using logistic regression, as it may lead to biased estimates and inaccurate inferences.
Results
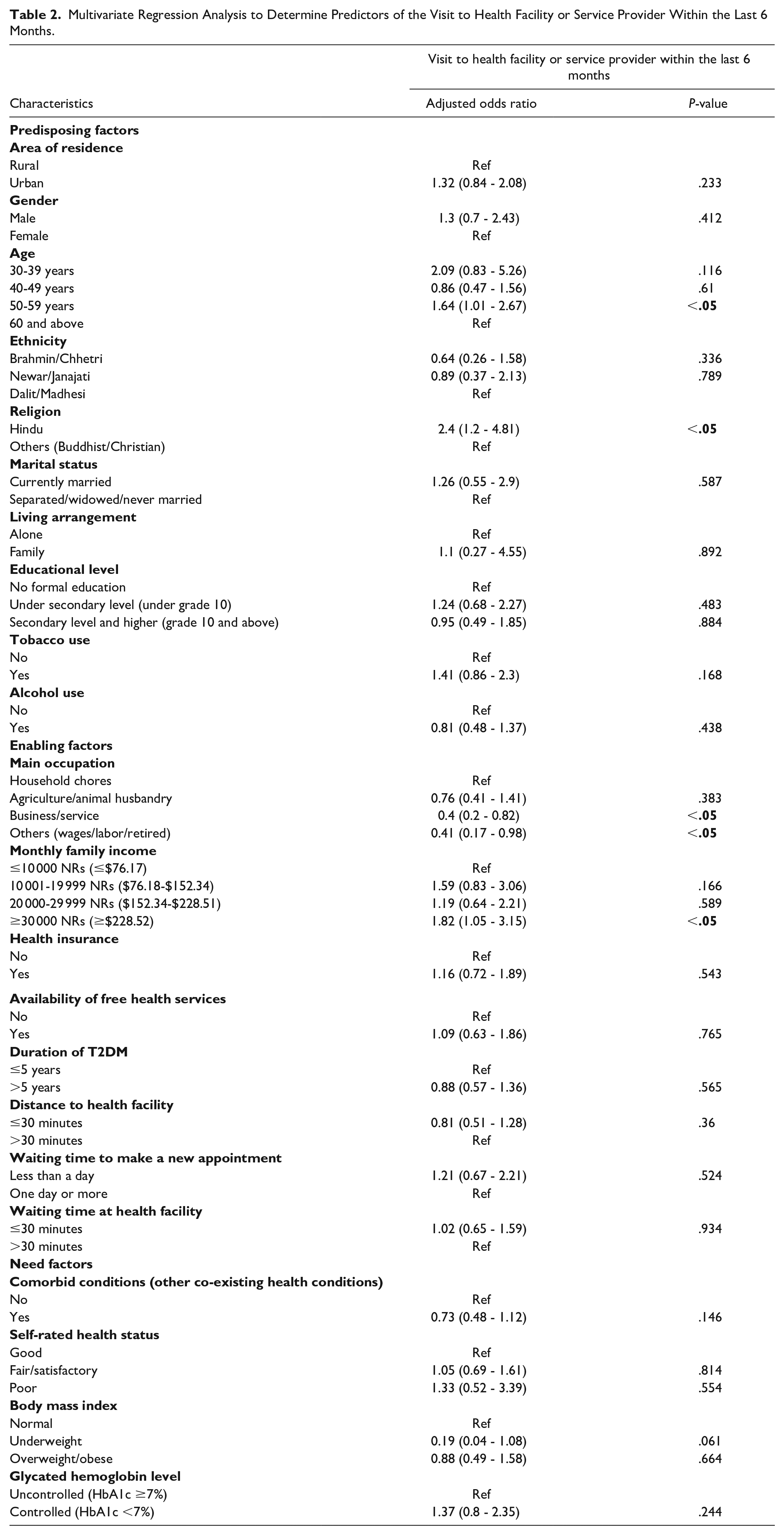
The mean (±SD) age of the study participants was 54.4 (± 9.4) years and 52.8% were males (Table 1). The majority of the study participants (66.1%) visited a health care facility or service provider within the last 6 months preceding the survey (Figure 1). Age, religion, occupation, and monthly family income were significantly associated with visits to health care facility or service provider within the last 6 months (Table 2).
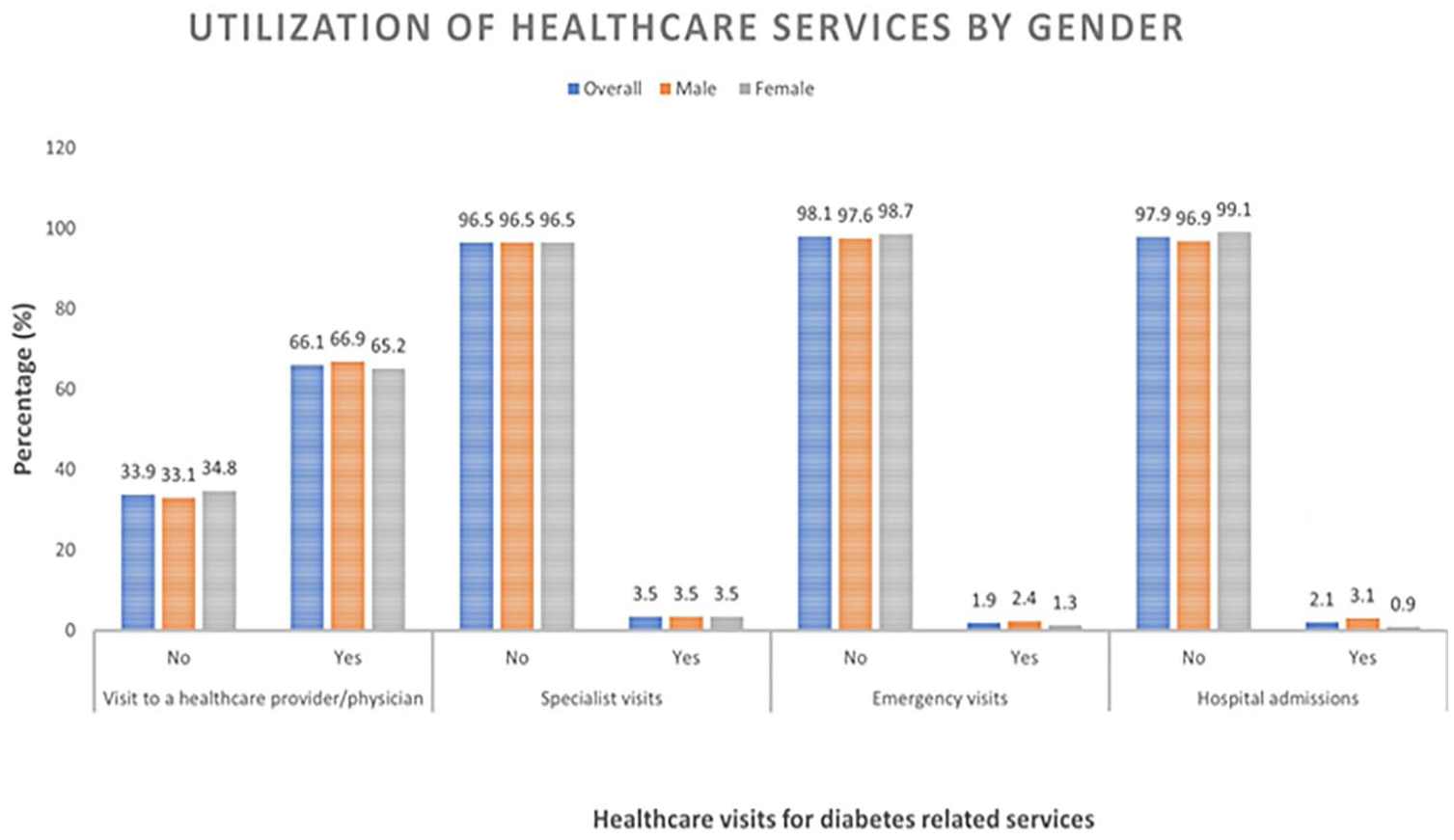
Utilization of health care services to manage type 2 diabetes.
Multivariate Regression Analysis to Determine Predictors of the Visit to Health Facility or Service Provider Within the Last 6 Months.
The prevalence of visits to the emergency department (1.9%), visits to specialists (3.5%), and hospital stays (2.1%) was very low.
Discussion
In this study, 66% of participants visited health care facilities, which is much lower than a previously conducted study in Nepal (93.7%). 7 The findings of this study show that the utilization of health care services among people with T2DM in Nepal is reasonably low, which requires immediate attention to prevent the progression of early diabetic complications such as kidney disease, artery diseases, neuropathy, eye problems, and foot ulceration.
Similarly, despite a low level of health care service use in our study, a lower proportion of participants visited the emergency department and were hospitalized compared with previously conducted study in Nepal. 7 This might be because people in Nepal tend to seek medical services unless they are severely sick and some often terminate the treatment of their chronic condition due to unaffordability of the health care services (high cost of medication and inaccessible health care services). 8
In this study, age, religion, family income, and occupation are the only factors associated with visiting a health care facility, and this is comparable to findings of other studies.9,10 However, none of the need factors were associated with the health care use in our study. These discrepancies might be because higher proportion (94.4%) of study participants in our study self-rated their health as good or satisfactory and more than half (50.5%) were without comorbid conditions which might have resulted in a lower visit to the health facility.
This study is limited by its reliance on self-reported survey data, which may lead to recall bias and a causal relationship between the variables could not be established due to the cross-sectional nature of the survey. Despite these limitations, this is the first community-based study to assess the utilization of health care services and its associated factors among people with T2DM from rural and urban population of Nepal. We conclude that the utilization of health care services among people with T2DM in Nepal was reasonably low. Identifying the underlying causes of low use of health care services is of great importance to bridge the gap in health care service use and management of diabetes.
Footnotes
Acknowledgements
The authors would like to thank all the study participants who agreed to be part of this study. The authors are grateful to the CoLID study group members for their support and input in this study. This research was supported by an Australian Government Research Training Program Scholarship.
Correction (December 2024):
Article has been updated to replace the first line of the Ethical Statement “This article presents the results of a baseline data analysis of a Randomized Control Trial (main study)” with “This is a sub-study of a 2-arm cluster randomised control trial, registered in the Australia and New Zealand Clinical Trial Registry (ACTRN12621000531819).
Authors’ Contribution
GP, LBR, and CV developed the study concept and protocol. GP was responsible for field data collection and contributed to the first draft. GP and PKD performed data analysis. GP and PKD interpreted the data and reviewed the manuscript. LBR and CV provided overall supervision and final comments. All authors have read the final manuscript and agreed for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main study from where the data were provided was funded by AMED Japan (Grant Number JP21JK0110020) under the Global Alliance for Chronic Disease (GACD) Call. However, the authors declare that no funding or specific grant was provided for the publication of this study.
Ethical Approval
This is a sub-study of a 2-arm cluster randomised control trial, registered in the Australia and New Zealand Clinical Trial Registry (ACTRN12621000531819). Ethical approval for the main study was obtained from the Nepal Health Research Council, the National Ethical Body of Nepal (Approval number: 944/2019P), and the Central Queensland University, Australia (CQU RSH/HE 0000022453).
Data Availability
The data of this study if required will be available on request from the corresponding author.