
Abstract
Histone H2AX undergoes phosphorylation as an answer to DNA double-strand breaks, which in turn are part of the oncogenic procedure. The detection of gamma-H2AX can potentially serve as a biomarker for transformation of normal tissue to premalignant and consequently to malignant tissues. The aim of this study was to evaluate the clinical significance of gamma-H2AX expression in breast cancer. Gamma-H2AX expression in tissues from 110 breast cancer patients was analyzed by immunohistochemistry and correlated with clinicopathological variables. Greater tumor size, higher grade, and the number of affected lymph nodes are significantly associated with greater values of gamma-H2AX. In addition, gamma-H2AX differs significantly among patients’ International Federation of Gynecology and Obstetrics stage. Higher values of estrogen receptor and progesterone receptor are significantly associated with lower gamma-H2AX values. In conclusion, a positive association between gamma-H2AX expression and infaust histopathological parameters was observed.
Introduction
Cancer is the leading cause of death worldwide, with breast cancer being the second most common type of malignancy and the fifth most common cause of cancer death. Among women, breast cancer is the most frequent malignancy type, which is also responsible for the greatest number of cancer-related deaths. According to World Health Organization data, 2.1 million women are diagnosed with breast cancer every year, whereas 627,000 women died from cancer in 2018. The above facts reveal the critical role of early diagnosis. The use of new biomarkers and the new risk assessment tools can play an important role in this direction. Regarding breast cancer, biomarkers specific to the particular patient and cancer type are cornerstones for the individual management planning, contributing to the early diagnosis and good prognosis.
The classical prognostic factors in breast cancer include the tumor size (T), the lymph node status (N), the presence of metastases (M) and lymphovascular invasion (LVI), the proliferation markers (such as Ki-67), the status of estrogen receptor (ER) and progesterone receptor (PgR), the human epidermal growth factor receptor 2 (HER2)/neu status, the histological type, and the patient’s age and ethnicity. 1 During the previous years, molecular tests, investigating a series of relative genes in formalin-fixed paraffin-embedded (FFPE) tissue specimens, have been commercially available, but these are indicated only for subgroups of patients and are associated with high cost.2,3
H2AX is a variant of histone H2A representing 2%–25% of total H2A, and its levels are cell line and tissue dependent. 4 Several events, 5 such as oncogenic stress, ionizing irradiation, treatment with radiomimetic agents, drugs, or even normal physiological processes, with meiosis and class-switch recombination being among them, are responsible for DNA damage.6,7 DNA double-strand breaks (DSBs) in their turn are responsible for the activation of three phosphatidylinositol 3-kinase-like kinases (PIKKs): ataxia telangiectasia mutated (ATM), ataxia telangiectasia and Rad3-related (ATR), and DNA-dependent protein kinase (DNA-PK), which catalyze the H2AX phosphorylation at serine 139 in the C terminus.8,9 The phosphorylated H2AX plays then a functional and structural role in DNA damage repair.
Considering the above mentioned points, it can be concluded that gamma-H2AX (gH2AX) could function as a sensitive marker for DSBs, which in turn signify genomic instability and can potentially contribute to cancer initiation and progression. As a consequence, monitoring the formation of gH2AX could potentially be a sensitive means of early breast cancer detection.
This study aims to reveal the role of gH2AX as a possible prognostic factor in breast cancer and its correlation with classical prognostic factors. The expression of gH2AX in normal breast tissue, and especially premalignancies, such as atypical hyperplasia, has previously been studied.2,3
H2AX is a variant of histone H2A representing 2%–25% of total H2A, and its levels are cell line and tissue dependent. 4 Several events, 5 such as oncogenic stress, ionizing irradiation, treatment with radiomimetic agents, drugs, or even normal physiological processes, with meiosis and class-switch recombination being among them, are responsible for DNA damage.6,7 DNA double-strand breaks (DSBs) in their turn are responsible for the activation of three phosphatidylinositol 3-kinase-like kinases (PIKKs): ataxia telangiectasia mutated (ATM), ataxia telangiectasia and Rad3-related (ATR), and DNA-dependent protein kinase (DNA-PK), which catalyze the H2AX phosphorylation at serine 139 in the C terminus.10,11 The expression of gH2AX in breast cancer tissues was determined, and its association with clinicopathological variables of patients with this malignancy was analyzed. To our knowledge, this is one of the very few studies investigating the detection of gH2AX in paraffin-embedded tissue blocks from breast cancer patients.
Materials and methods
Study subjects
The patients were treated in a university surgical clinic from January 2016 to September 2018. One hundred ten consecutive patients with newly diagnosed breast cancer were enrolled in this study.
The inclusion criteria were the following: newly diagnosed breast cancer and indication for surgical excision, according to the guidelines and after presentation of the case to the multidisciplinary oncological care team. History of malignancy at any site and previous antineoplastic therapy were the exclusion criteria.
The first contact with the patients was in the breast care unit ambulance. The patients completed a questionnaire that aimed at obtaining a more detailed medical history. The patients were explicitly informed on the conduct of the research and signed the informed consent form. As approved by the institutional review board and according to national law, coded tumor tissues were used.
Immunohistochemistry
The tissue specimens were formalin fixed and embedded in fresh paraffin. The subsequent steps performed were as follows: deparaffinization of the tissue on the slides, heat-induced epitope retrieval (antigen unmasking) with citrate unmasking solution (EnVision™ FLEX Target Retrieval Solution, Low pH 6, PTLink) for 10 min at a subboiling temperature (96°C), blocking each section with 150 µL of blocking solution (FLEX hyperoxidase blocking solution) for 1 h at room temperature, and incubation with gH2AX phospho-histone (Ser 139) rabbit monoclonal, clone 20E3 (CELL SIGNALING), at a dilution of 1:300 overnight at 4°C. EnVision™ FLEX/HRP was used as detection reagent. Hematoxylin counterstaining for 5 min followed by mounting of the slides and examination by light microscopy were the last steps of the tissue processing for the evaluation of gH2AX expression levels. In addition, antibodies against the following proteins were obtained from the indicated suppliers: estrogen receptor α (ERα) rabbit monoclonal, clone EP1 (DAKO), at a dilution of 1:50; progesterone receptor (PgR) mouse monoclonal, clone PGR636 (DAKO), at a dilution of 1:200; and c-erbB2/HER2/neu mouse monoclonal, clone CB11 (CELL MARQUE), at a dilution of 1:200. Stained sections were viewed for gH2AX at a magnification up to 400× and semiquantitatively scored by at least two independent pathologists (Figure 1). Regarding the evaluation of immunohistochemical staining, a percentage of positive nuclear staining was assessed for ERα, PgR, and gH2AX, and cell membrane staining was evaluated for HER2/neu (scoring of 0, 1+, 2+, and 3+ was applied), and in cases of HER2/neu score of 2+, a chromogenic in situ hybridization (CISH) was conducted and evaluated according to the guidelines of the College of American Pathologists and the American Society of Clinical Oncology. 12

(a) High expression of gH2AX with heterogeneous intensity (200× magnification). (b) High expression of gH2AX (200× magnification). (c) Low expression of gH2AX (200× magnification). (d) Very low expression of gH2AX (200× magnification).
Statistical analysis
Normal distributed variables are expressed as mean (standard deviation (SD)), while variables with skewed distribution are expressed as median (interquartile range (IQR)). Qualitative variables were expressed as absolute and relative frequencies. The Mann–Whitney test was used for the comparison of gH2AX between two groups, and the Kruskal-Wallis test, for the comparison of means among more than two groups. The Bonferroni correction was used in case of multiple testing, to control the probability of type I error. Spearman’s correlation coefficients were used to explore the association between two continuous variables. Correlation coefficients between 0.1 and 0.3 were considered low, between 0.31 and 0.5 were considered moderate, and those over 0.5 were considered high. Multiple linear regression analysis was used with the values of gH2AX being the dependent variable, using the stepwise method (p for entry 0.05, p for removal 0.10) and logarithmic transformations due to non-normal distribution of the dependent variable. Adjusted regression coefficients (β) with standard errors (SEs) were computed from the results of the linear regression analysis. All reported p values are two tailed. Statistical significance was set at p < 0.05, and analyses were conducted using SPSS statistical software (version 22.0).
Results
The study included tumors from 110 patients (male/female = 1/109) with mean age 61.4 years (SD = 13.9 years). A total of 57.3% of the patients presented with cancer in the right breast and 41.8% in the left one. The majority of patients were at stage T1 or T2 (47.3% and 45.5%, respectively), whereas 6.4% were at stage T3 and 0.9% at stage T4. The mean tumor size was 2.5 cm (SD = 1.7 cm), while 40.9% had a grade 3 tumor. The median number of examined lymph nodes was 8.5 (IQR = 3–15), and the median number of affected lymph nodes was 1 (IQR = 0–4). Histological stage II (43.6%) was found in the majority of the patients, followed by histological stage I (40%) and III (22%). Regarding the prognostic stage, stage I was found in most of the patients (68.2%), followed by stage III (19%) and stage II (16%). Most patients (70.9%) had undergone mastectomy, either for oncological indications or for their preference. Quadrantectomy was conducted in 18% and lumpectomy in 14% of the study population. Patients’ clinicopathologic characteristics, hormone receptor, HER2/neu, and gH2AX expression and Ki-67 labeling index are presented in Table 1. Regarding hormone receptor status, 71.9% of the patients were ER positive and 40.8% of them were PgR positive. A total of 41% of the patients were HER2/neu negative. An HER2/neu score of 2 was observed in 48.2% of the patients, while 24.5% of them had a positive CISH. Patients’ median expressions of gH2AX and Ki67 were 45% (IQR = 20–70) and 35% (IQR = 30–60), respectively. Regarding the intrinsic subtypes, the majority of the patients had a luminal B tumor (45.4%), whereas the minority had a triple-negative tumor (9.1%).
Patients’ clinicopathologic characteristics, hormone receptors status, and proliferation index markers.
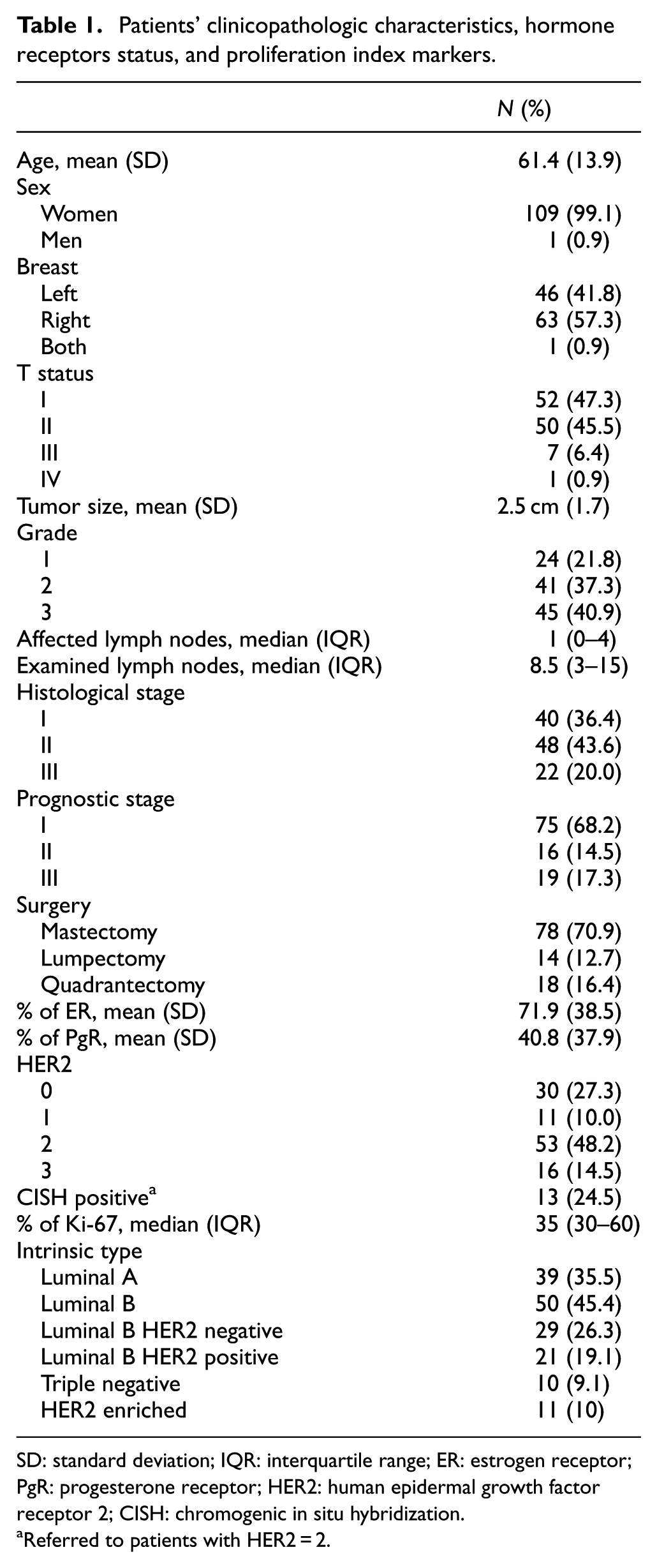
SD: standard deviation; IQR: interquartile range; ER: estrogen receptor; PgR: progesterone receptor; HER2: human epidermal growth factor receptor 2; CISH: chromogenic in situ hybridization.
Referred to patients with HER2 = 2.
Correlation of gH2AX and immunohistochemical profile of tumors
Greater tumor size, higher grade, and the number of affected lymph nodes are significantly associated with greater values of gH2AX (Table 2). In addition, gH2AX differs significantly among patients’ International Federation of Gynecology and Obstetrics stage. After Bonferroni correction, it was found that patients of stage I had significantly lower values compared to those of stage II and III (p = 0.001 and p = 0.003, respectively). Similarly, patients of prognostic stage I had significantly lower values compared to those of prognostic stage II and III (p < 0.001 and p = 0.001, respectively). Moreover, patients who had undergone mastectomy had significantly higher gH2AX values compared to those who had undergone lumpectomy (p = 0.014). This may be explained through the operative indication, where mastectomy was mostly indicated for more advanced tumor stages. More specifically, all the patients with T2–T4 tumors and 20 of the patients with T1 tumors underwent mastectomy. This means that patients undergoing mastectomy for an oncological indication because of the severity of the disease have also higher expression levels of gH2AX.
Percentage of gH2AX association with sample’s characteristics.

CISH: chromogenic in situ hybridization; IQR: interquartile range; ER: estrogen receptor; PgR: progesterone receptor; HER2: human epidermal growth factor receptor 2.
Spearman’s correlation coefficient.
Kruskal–Wallis test.
Mann–Whitney test.
When gH2AX was associated with hormone receptor expression, it was found that higher values of ER and PgR are significantly associated with lower gH2AX values (Table 2), indicating that the hormone receptor positivity, already established as a favorable prognostic factor, is related to low gH2AX expression. On the contrary, HER2/neu and Ki-67 were positively associated with gH2AX. Patients with HER2/neu +2, who had positive CISH, had significantly higher gH2AX values compared to patients with HER2/neu +2, who had negative CISH. Table 3 presents the average value and standard deviation of percentage of gH2AX Ser 139 expression in association with sample’s characteristics. More specifically, the average value of gH2AX expression was higher in histological and prognostic stage II and in patients undergoing quadrantectomy.
Average value and standard deviation of percentage of gH2AX Ser 139 expression in association with sample’s characteristics.

CISH: chromogenic in situ hybridization.
When multiple linear regression analysis was applied, it was found that the type of surgery, PgR, HER2/neu, and grade were significantly associated with gH2AX, in a way similar to the univariate analysis (Table 4).
Multiple linear regression analysis results, with percentage of gH2AX as a dependent variable and sample and clinical characteristics as independent ones.

SE: standard error; PgR: progesterone receptor; HER2: human epidermal growth factor receptor 2.
Regression coefficient.
Regarding the intrinsic subtypes, gH2AX was found to differ significantly among them. After Bonferroni correction, it was found that significantly lower values were found in luminal A and luminal B HER2-negative compared to luminal B HER2-positive (p < 0.001 for both comparisons), triple-negative (p < 0.001 for both comparisons), and HER2-enriched (p < 0.001 for both comparisons) subtypes. Also, significantly lower values were found in luminal B HER2 positive compared to triple negative (p = 0.003) (Table 5).
Average and median values of percentage of gH2AX Ser 139 expression in association with intrinsic subtypes.

SD: standard deviation; Kruskal–Wallis test; HER2: human epidermal growth factor receptor 2.
Discussion
Breast cancer is a major health problem, and the need for early diagnosis and personalized therapy is mandatory. The use of biomarkers may be in this regard very helpful. gH2AX is a novel biomarker of double-strand DNA damage. Our results showed that gH2AX levels may reflect endogenous genomic instability in breast cancerous tissues. Increasing staining of gH2AX was associated with unfavorable prognostic factors, including tumor stage, grading, hormone receptor negativity, and Ki-67. Higher gH2AX expression levels may be indicative of a more aggressively proliferating tumor phenotype, as a result of DNA double-strand defects. These findings are of great importance, since they imply that gH2AX could serve as a new tumor biomarker for cancer diagnosis and surveillance. To our knowledge, this is the first prospective research study with such a number of studying subjects, investigating the relationship between gH2AX and TNM anatomic and prognostic stage and other established breast cancer prognostic parameters, which is of great significance in the daily decision-making practice.
Similar results were found by Yang et al. 13 who showed that gH2AX expression is significantly associated with poor clinicopathologic features. Nagelkerke et al. 14 came to the conclusion that, in a multivariate analysis with tumor size, grade, and triple negativity, only the interaction between triple negativity and gH2AX remained significant. Sedelnikova et al. 15 proposed that detection of gH2AX could benefit for the early cancer screening, with breast cancer included. As gH2AX detection provides a considerably more sensitive, efficient, and reproducible measurement of the amount of DNA damage, compared to other techniques, such as pulsed field gel electrophoresis and comet assays, it is suggested that it could be used for early cancer screening. 16
It should be noted that our study has several limitations. First, the sample size in this study is relatively small, although bigger in comparison to similar studies. Second, our study was conducted in a single center, and this may lead to limited external validity, implausible effect size, and unequal allocation of resources of the study. Further validation with larger cohort and/or multicenter studies is needed.
In conclusion, using a cohort of 110 patients suffering from breast cancer, we observed a positive association between gH2AX expression and infaust histopathological parameters. Further investigations are required to explore the detailed mechanisms by which the gH2AX signaling pathway is involved in tumorigenesis in breast tissues and to establish new diagnostic and eventually therapeutic strategies using gH2AX as a target. It is important to include gH2AX in new cancer biomarkers studies for validation and proper investigation of its impact on cancer diagnosis and follow-up.
Footnotes
Acknowledgements
The authors thank Petraki Maria for technical support.
Authors’ contribution
V.V.P. conceived the presented idea, developed the theory and performed the computations, searched literature, wrote the manuscript, verified the analytical methods, and supervised the findings of this work. G.K. searched literature and wrote the manuscript. C.V. helped in sample collection, pathological diagnoses, performing immunohistochemistry and in situ hybridization, data acquisition, and evaluation of pathological, immunohistochemical, and in situ hybridization data. G.S. helped in sample collection, pathological diagnoses, and data acquisition. O.T. and H.T. helped in sample collection and pathological diagnoses. P.P., D.D., and D.P. helped in data acquisition and supervision of the work
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the institutional review board of Atticon Hospital, Greece.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.