
Abstract
The study was to evaluate the prevalence of mismatch repair gene defect among Thai patients with endometrial cancer and its association with clinico-pathological features and survivals. The formalin fixed paraffin-embedded blocks of EMC tissue from hysterectomy specimens of patients having surgery in our institution between 1 Jan 1995 and 31 December 2016 were assessed for the immunohistochemical expression of 4 mismatch repair proteins (MLH1, PMS, MSH2, MSH 6). Mismatch repair gene defect was determined by a negative expression of at least 1 protein. Among 385 EMC patients included in the study, mean age was 57.3 ± 10.8 years with 62.3% aged ⩽ 60 years. The most frequent mismatch repair gene defect was MSH6 (38.7%), followed by PMS2 (34.3%), MLH1 (33.2%), and MSH2 (16.4%). Overall, 55.1% showed negative expression of at least one protein. We found significantly higher mismatch repair gene defect in patients aged ⩽ 60 years, with early stage disease, and negative lymph node status than the other comparative groups: 59.2% vs 48.3% for age (p = 0.037), 58.2% vs 45.2% (p = 0.027) for stage, and 58.1% vs 44.6% (p = 0.048) for nodal status. The 5-year progression-free survival, overall survival, and endometrial cancer-specific survival of patients with mismatch repair gene defect was higher than those without gene defect. The differences were statistically significant for only progression-free survival and endometrial cancer-specific survival: 87.7% (95% confidence interval = 83.0%–92.4%) vs 81.5% (95% confidence interval = 75.4%–87.6%) (p = 0.049) for progression-free survival and 91.0% (95% confidence interval = 86.9%–95.1%) vs 85.5% (95% confidence interval = 80.0%–91.0%) (p = 0.044) for endometrial cancer-specific survival, respectively. In conclusion, more than half of Thai endometrial cancer patients had mismatch repair gene defect. The patients with mismatch repair gene defect had significantly younger age (⩽ 60 years) and better prognosis in terms of early stage, negative nodal status, and longer survivals.
Introduction
The majority of endometrial cancers (EMC) occur sporadically, with only 2%–3% related to familial risk. 1 Lynch syndrome is the most common genetic risk factor of EMC as well as colorectal cancer (CRC). Women with Lynch syndrome had an increased lifetime risk for EMC and CRC compared to the general population: 16%–61% and 18%–61% versus 2%–3%, respectively.2,3 Either EMC or CRC can precede one another. One study found that 50% of affected women with Lynch syndrome developed EMC prior to CRC. 4 Another study reported that affected women who had a history of CRC had a six-fold risk of EMC, 25% of whom was discovered within 10 years. 5 Other cancers related to Lynch syndrome, aside from EMC and CRC, include cancers of the ovary, breast, gastric, urinary tract, biliary tract, skin, and so on. 6
Genetic study is a gold standard test to determine a genetic abnormality. However, it has a high cost and is not readily available in most laboratories. Hence, screening an individual at risk using data such as age at EMC diagnosis, presence of other cancers or cancer in family members, and laboratory investigation of tumor tissue is more cost-effective.7–9 An examination of tumor tissue is done either by a polymerase chain reaction to amplify the microsatellite foci to detect microsatellite instability (MSI) or by an immunohistochemical (IHC) study to detect a loss of mismatch repair (MMR) protein.
Microsatellite is a sequence of nucleotides forming the deoxyribonucleic acid (DNA) or genome. Abnormal DNA sequencing or incorrect DNA base pairs, so called MSI, may occur during DNA replication. In normal physiologic systems, abnormalities are corrected by the MMR protein regulated by MMR gene. In individuals with MMR gene mutation as in Lynch syndrome, abnormal DNA would be left unrepaired, accumulate, and eventually result in cancer. The MMR gene has many locations, such as MutL homolog 1 (MLH1), postmeiotic segregation increased 1 (PMS1), postmeiotic segregation increased 2 (PMS2), MutS protein homolog 2 (MSH2), and mutS homolog 6 (MSH6).
Because EMC is more common in Western countries, limited information was available in Asia especially about genetic-related disorders including a loss of MMR protein. The objective of this study was to determine the prevalence of MMR defect (MMRd) identified by a loss of protein by IHC study of EMC tissues. The associations between MMR protein loss and clinicopathological features as well as survivals were also studied.
Materials and methods
The study was conducted following approval from the institution’s ethics committee for research. Inclusion criteria were all EMC patients who underwent surgery in the institution between 1 January 1995 and 31 December 2016 and had available pathology reports. Surgery generally included total hysterectomy, bilateral salpingo-oophorectomy, and lymph node dissection if indicated. Patients who had radiation or chemotherapy as a primary treatment prior to surgery, did not undergo hysterectomy, did not have clinical data, as well as those who had no available or inadequate tissue from hysterectomy specimen were excluded.
Clinicopathological data collected included age at EMC diagnosis, general features of the patients including ethnicity and other medical morbidities, presence of other cancers, any cancers in the family, type of those cancers, International Federation of Gynecology and Obstetrics (FIGO) stage, primary location of EMC in the uterus, histopathology and grade, depth of myometrial invasion, lymphovascular invasion (LVSI), lymph node metastasis, duration of follow-up, status of disease, and living status. Data of stage among patients treated prior to 2009 were taken from a database of our previous report which had re-classified disease stages according to the FIGO 2009 criteria. 10
The IHC study for the four MMR proteins (MLH1, MSH2, PMS2, and MSH6), including the methods of interpretation and evaluation for the intra- and inter-observer reliability by the two researchers, is described in Data Materials. Cases with positive IHC staining of all four proteins were regarded as intact MMR protein (MMRi). Cases with negative staining of one or more MMR protein were interpreted as loss of MMR protein or MMR defect (MMRd).
Data analyses for the prevalence of MMRd, survivals, the association between the MMR status and clinicopathological factors, and the association between clinicopathological factors including MMR status and survivals are described in detail in Data Materials.
Results
Out of 474 EMC patients identified, 89 were excluded: 44 had no available paraffin tissue blocks of hysterectomy specimens, 25 had no residual cancer or had only endometrial hyperplasia, 12 had inadequate tissue for IHC process, and 8 had either pre-operative chemotherapy or radiation therapy prior to surgery. A total of 385 patients met inclusion criteria and were included in the study. All were Thai with 62.3% having co-medical morbidity of hypertension, diabetes mellitus, obesity, thyroid disorders, or their combinations. Data of medical illnesses in most patients had been reported in detail in our previous study. 11
From the first 40 slides, the kappa values of interpretation were 0.688 for inter-observer reliability and 0.741 and 0.833 for intra-observer reliability. From all 1540 slides (385 cases), the inter-observer reliability was 0.977. All 70 slides with discordant results of positive or negative staining between the two authors were studied and discussed before reaching a consensus.
Mean age of the patients was 57.3 ± 10.8 years, with 62.3% aged ⩽60 years. The majority had early stage (I–II) diseases (75.8%) and grade 1–2 tumors (72.5%). Endometrioid carcinoma, with or without other minor components, was most commonly found (90.4%). Out of 295 patients with available data, 16.9% had history of other cancers whereas 6.1% had a history of cancer(s) in the family.
Our study found that 44.9% of all 385 cases showed MMRi (positive expression of all four MMR proteins) and 55.1% had MMRd (negative expression of at least one MMR protein). Only one protein defect was found in 28.8%. Others had two (37.3%), three (16.5%), or all four MMRd (17.4%). Overall, either isolated or in combination, the most common defect identified was MSH6 followed by PMS2, MLH1, and MSH2 in order of frequency. Details of MMR protein expression are shown in Table 1.
Immunohistochemical expression of MMR protein in endometrial cancer.

MMR: mismatch repair.
The IHC expression of MMR proteins according to the clinicopathological features of the patients was studied (Table 2). Regarding the three clinical features of age, family history of cancer, and presence of other cancer, we found mean ages of the patients with MMRd and with MMRi were not significantly different: 56.8 ± 10.32 years versus 57. 9 ± 11.46 years (p = 0.363). Nevertheless, MMRd was found to be significantly higher in patients aged ⩽60 years than the older age group: 59.2% versus 48.3% (p = 0.037). We could not demonstrate significant association of MMRd and presence of other cancers or family history of cancer despite a higher prevalence of MMRd particularly in those with family history of cancer (72.2% vs 57.4%, p = 0.217). Types of other cancers and cancers in family members according to the status of MMR protein are shown in Table 3. Clinical data of other synchronous or metachronous cancer(s) in some patients were detailed in our previous work. 12
Clinicopathological features of endometrial cancer patients by the expression of MMR proteins.

MMR: mismatch repair; FIGO: International Federation of Gynecology and Obstetrics.
Non-endometrioid included serous carcinoma, clear cell carcinoma, and carcinosarcoma.
History of other cancers and family history of cancer and the status of MMR proteins.
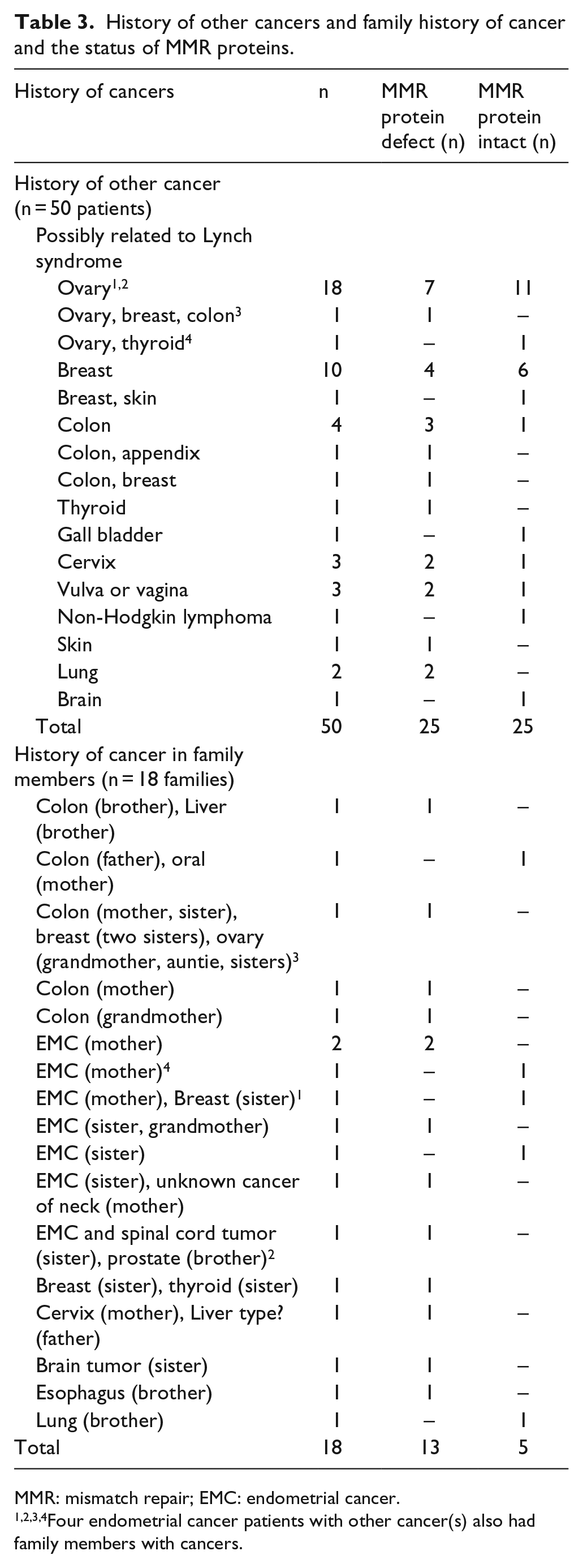
MMR: mismatch repair; EMC: endometrial cancer.
1,2,3,4Four endometrial cancer patients with other cancer(s) also had family members with cancers.
Among the pathologic features studied, early stages and absence of lymph node metastasis were significantly associated with higher rates of MMRd than the comparative groups. Although we found that EMC originated from lower uterine segment (LUS) and endometrioid cancer had higher rate of MMRd, the differences were not statistically significant. Upon logistic regression analysis, no factors were independently associated with MMRd (data not shown).
After a median follow-up of 64.3 months (range = 0.07–266.9 months), 21 (5.5%) had progressive diseases while 33 (8.6%) had recurrences. A total of 80 patients (20.8%) died. The 5-year progression-free survival (PFS) was 84.5% (95% confidence interval (CI) = 80.2%–88.0%). Causes of death were from EMC in 45 patients (11.7%), medical illnesses in 25 (6.5%), and other cancers in 10 (2.6%). The 5-year overall survival (OS) and EMC-specific survival (ESS) of all patients were 82.5% (95% CI = 77.9%–86.1%) and 87.1% (95% CI = 83.0%–90.2%), respectively.
Upon subgroup analyses for survivals (Table 4), we found that patients aged ⩽60 years, with early stage disease, endometrioid histopathology, tumor grade 1–2, myometrial invasion ⩽1/2, absence of LVSI, no nodal metastasis, and MMRd had higher 5-year survivals than other comparative groups. Figure 1 demonstrates significantly longer PFS and ESS (but not OS) of the patients who had MMRd than those with MMRi. When combined factors of stage and MMR status, the positive impact of MMRd on survivals was significant among patients with advanced but not early stage diseases.
Survivals according to prognostic features of endometrial cancer patients (n = 385).

PFS: progression-free survival; CI: confidence interval; ESS: endometrial cancer–specific survival; OS: overall survival; LUS: lower uterine segment; MMRd: mismatch repair defect; MMRi: mismatch repair intact.

(a) Progression-free survival, (b) endometrial cancer-specific survival, and (c) overall survival of endometrial cancer patients with normal and with defect mismatched repair genes.
The hazard ratios by uni- and multi-variable analyses of each prognostic factor are shown in Table 5. Only stage, histopathology, and LVSI were significant factors for survivals.
Hazard ratio of clinicopathological prognostic factor for survivals.

CI: confidence interval; PFS: progression-free survival; ESS: endometrial cancer–specific survival; OS: overall survival; MMR: mismatch repair.
Discussion
Aside from taking a thorough history, molecular and IHC studies of tumor tissue for MSI or MMR gene defect are used before proceeding to a genetic test. The study by IHC is more convenient and cheaper, with comparable function between the two tests. 13 Our study minimized the overinterpretation or underinterpretation of IHC study by several means. First, instead of tissue microarray, we selected the largest area of tumor without inflammation or necrosis from the slide before processing the tissue block for IHC study. Second, the qualitative criteria for IHC interpretation were quite rigid such that even faint or focal positive staining was interpreted as positive. These were to avoid any undetected positive area of protein expression (overinterpretation of MMRd). Finally, two researchers studied each slide independently with a high kappa value of correlation.
Most data of genetic aberration, particularly MMRd in EMC, have been derived from Western populations3,14–18 with a few reports from Asia.19–24 Our study, which was the first study of MMRd among Thai EMC patients, in a tertiary hospital in urban area of Thailand included 385 Thai EMC patients. Despite a high percentage (62%) of co-medical illnesses which were well known risk factors for EMC (sporadic cases in particular), the 55% of MMRd suggesting the possibility of genetic risk was quite high comparing to 18%–40% found in other studies from the West3,14–18 or from Asia.19–24Aside from the ethnic difference which was reported to influence the rate of MMRd, 22 different proportions of other features may contribute to the differences: for example, age, history of other cancers in individuals and cancers in the family which are associated with higher genetic risk, histopathology, and even screening techniques used (tissue microarray or whole tissue section). Some authors included patients aged <50 years 25 and found slightly more frequent MMRd than others which also included patients aged >50 years:22,26 30%–34% and 19%–24%, respectively. Our study included EMC patients of all ages (mean = 57 years) yet found high MMRd. The high rate of other cancers in our study, 17% compared to 6%–7% in other studies,23,27 may be one reason. This high rate of other cancers in our study may partly be due to a long follow-up period of over 5 years (up to 22 years) compared to 4 years (up to 17 years) in another study. 27 Although we found a lower rate of family history of cancers than in other studies (5% compared to 8%–11%),24,27 we were aware of the underestimation because of a less common practice of a detailed family history taking in our culture resulting in unrevealed or incomplete data record on this issue. The percentage of endometrioid pathology in each study may also contribute to the difference. One study which found overall 28% MMRd reported a higher rate of 45% among endometrioid cancer but not in serous or clear cell carcinoma. 28 Our study found 57% MMRd in endometrioid cancer yet 41% in non-endometrioid cancer. Hence, the rates of MMRd from these studies were influenced not only by a single feature alone but rather by many in combination
Regarding the type of each protein defect, previous studies from other populations showed various rates of each affected gene in EMC patients: 21%–45% for MSH2, 20%–54% for MLH1, 16%–71% for MSH6, and 15% for PMS2.3,14–18 Our findings of 30% to nearly 40% of the three MMRd (MSH6, PMS2, and MLH1) were in the range reported in previous studies. An exception was a defect of MSH2 that was relatively low (16%) compared to those of other studies. Nevertheless, these rates of each MMRd from our study and previous studies from the West were much higher than the China study which reported MMRd in 16% of MSH6, 12% of MSH2, 8% of PMS, and only 6% of MLH1. 24
Considering the low prevalence of 3%–5% of germ-line mutation among the MMRd,28,29 MMR study in all EMC patients was not practical especially in limited resourced areas. Among organizations which recommended cancer tissue screening prior to a genetic test for Lynch syndrome, some recommended the test in all individuals with EMC regardless of age13,30,31 or family history of cancer. 13 Others recommended limiting only to patients aged ⩽60 years.29,32
Our study found a significant association between age ⩽60 years and MMRd. Hence, selective tissue screening only in patients aged ⩽60 years may be more appropriate in a low-resource setting. By age criteria, only 240 aged ⩽60 years would be submitted for tissue examination instead of all 385 cases. Aside from age, other important features indicating screening are other primary cancers in the patient and history of related cancer in close relatives.30–34 Although a higher prevalence of MMRd in our patients with family history of cancers was not statistically different from those without defect (72% vs 57%, p = 0.217), we interpreted that a 15% difference was clinically meaningful and a positive family history should reinforce the indication for screening. By these two combined criteria of age ⩽60 years and positive family history, only 14 patients were strongly encouraged to undergo tissue study.
We explored our contradictory finding of a lower rate of MMRd in patients with other cancers, particularly ovarian and breast cancers, which are also common in Lynch syndrome aside from CRC. Among 19 and 11 EMC patients who had ovarian cancer and breast cancer (without CRC), only 7 and 4 had MMRd, respectively. One systematic review found that only 51% of breast cancer showed evidence of MMRd or had increased risk of Lynch syndrome. 35 The sporadic nature of EMC or adjuvant tamoxifen for preceding breast cancer may be among the reasons. Another possibility was the other genetic derangements. One study which explored germ-line mutation in ovarian cancer found that 2% was caused by MMR gene mutation and 11% by mutation in BRCA genes. 36 Particularly in those with hereditary ovarian cancers, 10%–15% was found to be from Lynch syndrome and 65%–75% was from breast–ovarian cancer syndrome. 37 Unfortunately, the cost of an MMR or BRCA gene mutation study to confirm the genetic derangement is very high and not readily available in our laboratories.
Concerning the relationship of MMRd and pathological features, previous studies reported inconsistent findings. Some found no relationship between MMRd and stage or grade of EMC. 38 Some authors demonstrated that EMC with MMRd or EMC related to Lynch syndrome frequently had cancer originating at LUS. 39 Other studies especially from the West reported that these EMC had more aggressive features than sporadic EMC, such as, larger tumor size, more likely to be non-endometrioid or grade 3 cancer, deep myometrial invasion, more frequent LVSI, and at a more advanced stage.29,39–42 Although our study found our EMC patients with MMRd more frequently originated from LUS and had endometrioid histopathology, the differences were not statistically significant from those with MMRi. Other pathologic features in our patients with MMRd were more favorable than those with MMRi in terms of early stage and absence of nodal metastasis. The more favorable features of patients with MMRd in our study were similar to some other reports particularly from Asia that also found early stage, more endometrioid histology, and lower grade tumor among patients with MMRd.21,23
Likewise, the prognostic influences of MMR defect on survivals could not be confirmed in all studies. Some studies showed lower survival rate of EMC patients with MMRd20,28,43,44 whereas others could not demonstrate any difference.40,45,46 Our study found, in concordance with more favorable clinicopathological features, that patients with MMRd had longer survivals (Table 5 and Figure 1), which was consistent with a few studies from Asia showing better survival for MMRd patients.19,21,23 Although MMR status showed no significant impact on survival from multi-variable analyses in our study, the influence of MMRd on features of disease and a trend for survival of patients especially with advanced stage diseases may add more information in counseling patients regarding prognosis and a more specific treatment plan.
Our study has strength in certain aspects. First, it is among a few reports from Asia exploring the MMR gene defect in EMC patients. Second, we included a large number of patients with relatively complete clinicopathological data. Third, a long follow-up duration may positively affect the findings of other cancers in the same individuals and cancers in the family members, which were dynamic and could increase from the cumulative incidence. Last, a large tumor area for pathological process and interpretation was carefully selected and interpreted independently by two researchers to increase the reliability of the test. Nevertheless, we were aware of certain limitations. There have been few data of genetic cancer in the Thai population; hence, both patients and physicians were not aware of this risk making data from our review on cancers in family members incomplete. Second, we did not perform tumor MLH1 methylation for those with MLH defect to exclude sporadic cancer due to lack of unavailable resources. Nevertheless, we had only eight cases with isolated MLH1 defect whereas others had MLH1 defect with the other MMR proteins defect, so the prevalence would not be substantially decreased. The last limitation was our financial restriction, so molecular and genetic tests were not performed. Further genetic study would be helpful for definite counseling to patients regarding risk of other cancers in themselves and family members.
In conclusion, the prevalence of MMRd in our Thai EMC patients was quite high. All involved physicians should consider submitting EMC tissue testing for MMRd especially in patients younger than 60 years, with a history of other cancers or cancers in the family, cancer originating from the LUS, early stage, or without lymph node metastasis. Lastly, the better prognostic features and survivals of our Thai EMC patients with MMRd were similar to findings from other studies in Asia, which differed from the West. Further studies, of larger Asian populations or a systematic review with meta-analysis, are warranted.
Footnotes
Acknowledgements
The authors thank Mrs Bulan Sriratanapan for her laborious work in searching for the pathologic slides and blocks, Mrs Unaporn Trongsakul and Mrs Pornphimon Kongjan for their excellent work in tissue processing for immunohistochemical study, and Dr Sumonmal Manusirivithaya and Mr Jason Cullen for their assistance in manuscript preparation. Si.T. contributed for the conception and design, pathological study, collecting clinical and pathological data, data analysis, writing the manuscript; T.K. for collecting clinical data, data management, editing and approval of the manuscript; and Su.T. for pathological study, collecting pathological data, editing and approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research was approved by the Ethical Committee for Research on Human Subjects of the Faculty of Medicine Vajira Hospital (COA 22/2559).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Faculty of Medicine Vajira Hospital research fund.