
Abstract
Esophageal squamous cell carcinoma is one of the most common malignant tumors. The oncogene c-MYC is thought to be important in the initiation, promotion, and therapy resistance of cancer. In this study, we aim to investigate the clinicopathologic roles of c-MYC in esophageal squamous cell carcinoma tissue. This study is aimed at discovering and analyzing c-MYC expression in a series of human esophageal tissues. A total of 95 esophageal squamous cell carcinoma samples were analyzed by the western blotting and immunohistochemistry techniques. Then, correlation of c-MYC expression with clinicopathological features of esophageal squamous cell carcinoma patients was statistically analyzed. In most esophageal squamous cell carcinoma cases, the c-MYC expression was positive in tumor tissues. The positive rate of c-MYC expression in tumor tissues was 61.05%, obviously higher than the adjacent normal tissues (8.42%, 8/92) and atypical hyperplasia tissues (19.75%, 16/95). There was a statistical difference among adjacent normal tissues, atypical hyperplasia tissues, and tumor tissues. Overexpression of the c-MYC was detected in 61.05% (58/95) esophageal squamous cell carcinomas, which was significantly correlated with the degree of differentiation (p = 0.004). The positive rate of c-MYC expression was 40.0% in well-differentiated esophageal tissues, with a significantly statistical difference (p = 0.004). The positive rate of c-MYC was 41.5% in T1 + T2 esophageal tissues and 74.1% in T3 + T4 esophageal tissues, with a significantly statistical difference (p = 0.001). The positive rate of c-MYC was 45.0% in I + II esophageal tissues and 72.2% in III + IV esophageal tissues, with a significantly statistical difference (p = 0.011). The c-MYC expression strongly correlated with clinical staging (p = 0.011), differentiation degree (p = 0.004), lymph node metastasis (p = 0.003), and invasion depth (p = 0.001) of patients with esophageal squamous cell carcinoma. The c-MYC was differentially expressed in a series of human esophageal tissues, and the aberrant c-MYC expression could be a potential factor in carcinogenesis and progression of esophageal squamous cell carcinoma. There was a statistical signification for c-MYC in esophageal squamous cell carcinoma patients to analyze clinicopathological features. It possibly becomes a new diagnostic indicator of esophageal squamous cell carcinoma.
Introduction
Esophageal squamous cell carcinoma (ESCC) is the eighth most common cancer and the sixth most frequent cause of cancer-related death in the world. 1 ESCC is one of the most frequent cancers worldwide that affects individuals after 50 years of age in a 3:1 ratio between males and females.2,3 ESCC is one of the most frequently diagnosed malignant tumors in developing countries. 3 Epidemiological studies have shown an increase in incidence in areas such as West and North of China, Hong Kong, Japan, South Africa, France, and Brazil.4,5 Despite progress in the multimodality treatment of esophageal cancer in the past several decades, the prognosis for esophageal cancer remains poor, especially in North China. 6 ESCC, which is the major histologic subtype of esophageal cancer, is prevalent in Asia but rare in the Western world. 7 The overall survival for ESCC patients is relatively short, with a 5-year survival rate of approximately 14%. 7 Most patients with ESCC are diagnosed at an advanced stage, and metastasis to the regional lymph nodes occurs frequently. 8 The development of ESCC is associated with the accumulation of multiple genetic/epigenetic alterations, including the activation of oncogenes and/or the inactivation of tumor suppressor genes. Amplification and overexpression of c-MYC are involved in development of ESCC.
C-MYC is considered to be a proto-oncogene that is often activated in carcinogenesis and abnormal proliferation. The protein product of c-MYC oncogene predominantly locates in the nucleus, and the expression of this oncogene is considered to play a role in controlling the transition of the cell cycle.9,10 The proto-oncogene MYC, located at 8q24.1, encodes a nuclear phosphoprotein, regulates almost 15% of human genes, and is activated in 20% of all tumors. 11 C-MYC is a transcription factor acting as a master regulator of genes involved in cell cycle progression, cell growth, differentiation, metabolism, and apoptosis. It is also a potent cellular oncogene that is found to be frequently deregulated in human cancers. This pathological upregulation is frequently due to chromosomal translocations leading to promoter rearrangement, gene amplification, and viral-mediated insertional mutagenesis.12,13 C-MYC is a transcription factor that regulates a broad range of cellular processes, which have been recognized to contribute to the initiation and progression of tumors. Overexpressed c-MYC is found in a large part of ESCC patients and is related to poor outcome. 14 In addition, amplification of c-MYC oncogene has been shown in esophageal cancers.4,15,16 However, the clinicopathological significance of c-MYC in ESCC has been rarely reported. Thus, this study was designed to investigate the impacts of c-MYC on the clinicopathological features of patients with ESCC. This study detected and analyzed the expression of c-MYC in a series of human esophageal tissues. The c-MYC expression was examined in tissue by various experimental methods. In addition, the relationship between c-MYC and clinicopathological significance of ESCC patients was analyzed.
Materials and methods
Tissue specimen collection
The study included 95 consecutive patients who underwent surgery for histologically verified esophageal squamous cell at the Department of Surgery, Gansu Provincial Hospital, between April 2014 and November 2016. A total of 95 specimens of human ESCC and paired adjacent normal tissues (ANT) and 81 specimens of atypical hyperplasia tissues (AHT) were obtained from patients of different grades who underwent esophagectomy at the Surgical Oncology Department. All patients never received any radiotherapy or chemotherapy prior to surgery. All specimens were acquired from three parts, respectively, in cancerous tissue, moderate and high AHT adjacent to carcinoma, and normal esophageal mucosa (which were confirmed by pathology). All the samples were histopathologically diagnosed as ESCC, and the following information was recorded for each patient: age, gender, ethnic, tumor location, tumor size, degree of differentiation, clinicopathological stage based on the seventh edition of the American Joint Committee on Cancer (AJCC) staging system, 17 and lymph node status. This study was approved by the Ethics Committee of Gansu Provincial Hospital (syll2015009), and all patients gave their informed consent prior to inclusion in the study.
Immunohistochemistry
The detection of c-MYC expression by immunohistochemistry (IHC) was carried out with the mouse anti-rabbit c-MYC monoclonal antibody purchased from ABclonal Biotech Co. (Woburn, MA, USA). All the specimens have been formalin-fixed and paraffin-embedded in advance and prepared for future use. Tissues were cut 3-µm thick and mounted on slides. After placing at room temperature for 60 min, tissue sections were deparaffinated twice in xylene 10 min per time, rehydrated five times in gradient ethanol (100%, 95%, and 80%) 10 min per time, and then rinsed with water and phosphate-buffered saline (PBS) for 5 min. The slides were placed in citrate buffer and heated to boiling in a microwave for 8 min for antigen retrieval. When the slides were naturally cooled, they were washed with PBS two times 3 min reduplicative; 0.3% H2O2 was then added to the section followed by incubation in a wet box for 10 min at room temperature and rinsed with PBS three times for 3 min; and the sections were blocked with 10% normal serum for 45 min. Rabbit anti-human c-MYC antibody (1:100; rabbit monoclonal antibody; ABclonal) was added, and slides were incubated overnight at 4°C. The next day, the slides were washed with PBS first and then biotinylated goat anti-rabbit secondary antibody was applied. The sections were incubated at room temperature for 15 min subsequently, followed by washing with PBS again. dibutyl phthalate was added to the slides for incubation, and the degree of dyeing was observed and grasped under a microscope; the sections were then washed and counterstained with hematoxylin, using hydrochloric acid alcohol for differentiation. According to the reverse order of rehydration above-mentioned for dehydration and then hyalinizing the slides with xylene, finally, a coverslip was added to the slide for microscopic examination.
Western blotting
The tissues obtained were cut using scissors and then the tissue samples were homogenized in an ultrasonic instrument. Following centrifugation at 5000g for 15 min at 4°C, the protein concentration was measured with a bicinchoninic acid (BCA) protein assay kit (23227; Thermo scientific, Pudong New Area, Shanghai). The protein samples with the tissue homogenates were electrophoresed, and the sample volume was calculated via protein concentration. Total protein (15 µg) was separated by 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) (15% gel, voltage: 60 V, 30 min and then 120 V, 90 min) under denaturing conditions and transferred to polyvinylidene difluoride (PVDF) membranes (electric current: 200 mA, 90 min). Membranes were blocked in 5% non-fat milk (27°C, 60 min) and then incubated (4°C, overnight) with the c-MYC antibody (1:1000; A1309; ABclonal Biotech Co.). After incubation with horseradish peroxidase (HRP)–conjugated secondary antibodies (27°C, 60 min), goat anti-rabbit (1:1000; ZhongShan Golden Bridge Biotechnology, Beijing, China) together with an HRP-conjugated primary antibody for β-actin (1:1000;TA-09; Zhongshan Golden Bridge Biotechnology), immunoreactive proteins were visualized using the LumiGLO chemiluminescent substrate (Cell Signaling Technology Inc., Danvers, MA, USA). Densitometric analyses were performed using Scion Image software.
Evaluation of immunostaining
The expression of c-MYC was assessed by two independent pathologists who had no previous knowledge of clinical data. The staining intensity score was classified as 1 (weak), 2 (moderate), and 3 (strong). The percentage of positive cells was scored as 0 (≤5%), 1 (6%–25%), 2 (26%–50%), 3 (51%–75%), and 4 (76%–100%). The staining intensity and percentage of staining cells were then multiplied to generate the immunoreactivity score for each case, ranging from 0 to 12. Tissue sections with an immunoreactivity score ≥4 were considered to be positive (high) expression, while a score <4 was considered as negative (low) expression. Pictures of representative areas containing the diagnosis of interest for each sample were taken and blindly scored by two observers.
Statistical analyses
The statistical calculation was carried out using version 17.0 of the SPSS software for Windows. Our study was designed to detect and analyze the c-MYC expression in a series of esophageal tissues and to test and verify the c-MYC expressed in esophageal cancer tissue. The χ2 test was used to analyze the statistical difference among ANT, AHT, and esophageal cancer tissues. The relationship between c-MYC expression and clinicopathological factors of esophageal cancer patients was statistically estimated using χ2 test. In all analyses, p value <0.05 was considered to be statistically significant.
Results
Clinical characteristics of ESCC patients
In our samples, 62 (65.3%) patients were males and 33 (34.7%) cases were females, and the average age at diagnosis was 60.5 years. In all, 73 of the cases were moderately and well differentiated, while 22 of the cases were poorly differentiated. In total, 95 patients were classified according to AJCC as follows: pathological stage T1, 26 (27.3%); pathological stage T2, 15 (15.7%); pathological stage T3, 30 (31.5%); and pathological stage T4, 24 (25.5%). In addition, 53 (55.8%) cases were with the lymph node metastasis, while 42 (44.2%) cases without the lymph node metastasis. Detailed characteristics of the patients included in this study are summarized in Table 1.
Characteristics of 95 ESCC patients included in this study n (%).

n: total number of cases, AJCC: American Joint Committee on Cancer.
C-MYC IHC results
C-MYC was expressed in the various esophageal tissues at different amounts. And, c-MYC expression appeared in the form of a nuclear staining pattern (Figure 1). Compared with the ANT and the AHT, c-MYC was highly expressed in esophageal cancer tissues. In most (58/95) ESCC cases, the c-MYC expression was positive in tumor tissues. The positive rate (PR) of c-MYC expression in tumor tissues was 61.05% (58/95), obviously higher than the ANT (8.42%, 8/95) and AHT (19.75%, 16/81). When comparing the two groups, the difference is statistically significant (p < 0.05) (Table 2).

Immunohistochemical expressions of c-MYC across various esophageal histologies (original magnification ×200): (a) the adjacent normal tissue, (b) the atypical hyperplasia tissue, and (c) cancer tissue.
C-MYC protein expression in normal, atypical hyperplasia, and cancer tissues.

C-MYC western blotting results
WB for c-MYC revealed little c-MYC protein expression in esophageal adjacent non-cancerous tissues. C-MYC expression was found in ESCC (p < 0.01) and atypical hyperplasia samples (p < 0.01). Figure 2(a) is a representative western blot for c-MYC protein expression, demonstrating higher c-MYC protein expression in ESCC. Furthermore, all samples positive for c-MYC were subject to densitometry, and the average c-MYC expression levels in ANT compared with adenocarcinoma are represented in Figure 2(b).
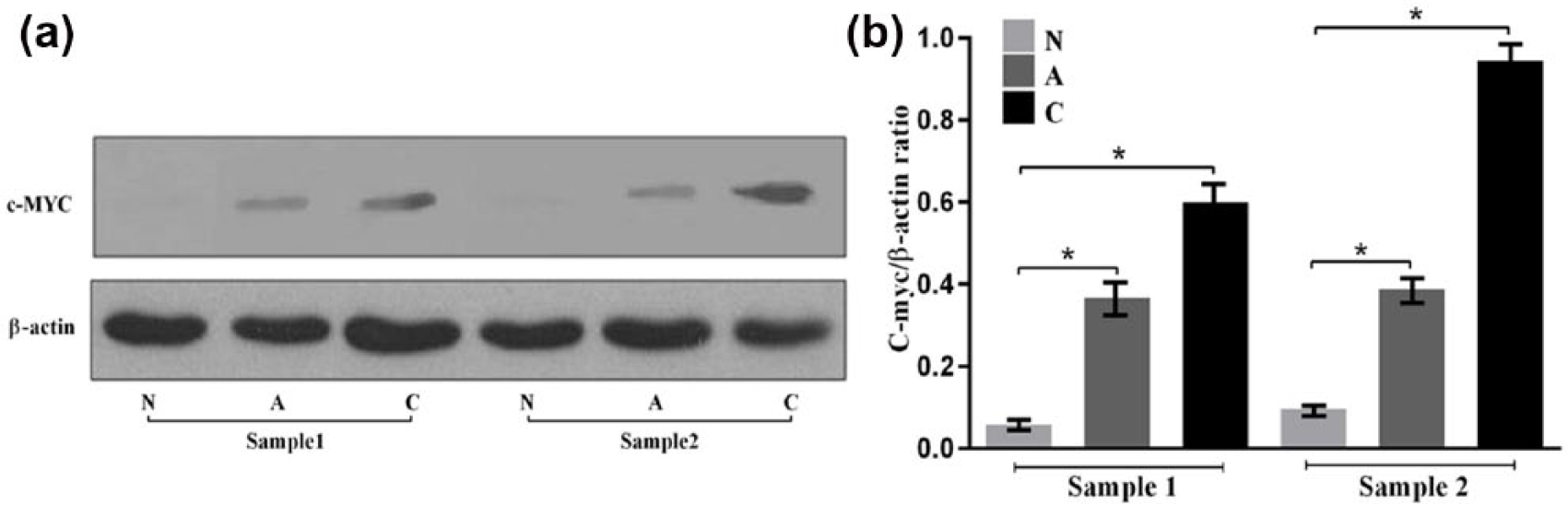
(a) Expression of c-MYC protein was evaluated by western blotting. Western blot for c-MYC protein demonstrating high c-MYC protein expression in esophageal cancer (C) compared with atypical hyperplasia (A), with undetectable levels in normal esophageal (N) samples. β-actin was used as a loading control. (b) Quantitation of western blots of c-MYC by densitometric scanning. The relative expression of c-MYC protein was higher in atypical hyperplasia (A) and esophageal cancer (C) samples (*p < 0.01 vs normal esophageal (N) samples).
Correlation between c-MYC and clinicopathological factors
Statistical analyses were done to examine the correlation between the expression of c-MYC protein and the clinicopathological characteristics of ESCC. As shown in Table 3, the PR of c-MYC expression was 40.0% (6/15) in well-differentiated esophageal tissues, 41.4% (24/58) in moderately differentiated esophageal tissues, and 81.8% (18/22) in poorly differentiated tissues, with a significantly statistical difference (p = 0.004). The PR of c-MYC was 41.5% (17/41) in T1 + T2 esophageal tissues and 74.1% (40/54) in T3 + T4 esophageal tissues, with a significantly statistical difference (p = 0.001). The PR of c-MYC was 45.0% (18/40) in I + II esophageal tissues and 72.2% (39/55) in III + IV esophageal tissues, with a significantly statistical difference (p = 0.011).
Correlation between c-MYC expression and the clinicopathological characteristics of the ESCC patients.

A statistically significant correlation between c-MYC protein expression and tumor differentiation degree, infiltration depth, lymph node metastasis, and clinical stage (p < 0.05) has nothing to do with patient age and gender (p > 0.05).
The PR of c-MYC was 77.4% (41/53) in lymph node metastasis and 47.6% (20/42) in no lymph node metastasis. C-MYC expression strongly correlated with clinical staging (p = 0.011), differentiation degree (p = 0.004), lymph node metastasis (p = 0.003), and invasion depth (p = 0.001) of patients with ESCC, whereas no statistical differences have been found between c-MYC expression and gender (p = 0.716) or age (p = 0.830) of patients with ESCC. Taken as a whole, these observations supported the notion that the increased c-MYC expression is associated with ESCC clinical progression.
Discussion
C-MYC is regulated in part through mitogenic stimuli and is activated constitutively in cancer cells through gene amplification, chromosomal translocation, point mutation, and mitogenic stimulation. 18 C-MYC is a transcription factor acting as a master regulator of genes involved in cell cycle progression, cell growth, differentiation, metabolism, and apoptosis. We retrieved literature and found that c-MYC is one of the most prevalent oncogenes altered in human cancer. 19 It is deregulated in about 50% of tumors, especially in Burkitt lymphoma and also existed in gastric, cervix, colon, breast, and lung cancers.20,21 In recent years, several studies have demonstrated that microRNA (miRNA) regulates esophageal squamous cancer cell proliferation through suppression of c-MYC pathway.15,16,22 This pathological upregulation is frequently due to chromosomal translocations leading to promoter rearrangement, gene amplification, and viral-mediated insertional mutagenesis.23,24 Most patients with ESCC are diagnosed at an advanced stage. Despite recent improvements in its treatment, the clinical outcome of ESCC patients remains unsatisfactory.20,25,26 Further investigation of the underlying molecular markers to improve the outcome of patients with ESCC is urgently needed. In this study, we found that c-MYC was overexpressed in various tissues of ESCC.
We first detected and analyzed the expression of the c-MYC in a series of human esophageal tissues, including the ANT, AHT, and tumor tissues, and illustrated that c-MYC expression differs in various types of esophageal tissue by immunohistochemical detection and western blot. We found that the c-MYC expression increased in esophageal cancer tissues, and the PR of c-MYC significantly increased with the malignant degree of ESCC patients. Furthermore, the increase in c-MYC expression has been started from the AHT and finally highly expressed in esophageal cancer tissues. In addition, we also explored the correlation between the expression of c-MYC protein and the clinicopathological characteristics of ESCC. We showed that the positive expression of c-MYC was significantly correlated with clinicopathological characteristics. The c-MYC was highly expressed in more tumors with poor differentiation degree, highly expressed in invasion depth, and highly expressed in lymph node metastasis than no lymph node metastasis, suggesting that c-MYC could be a potential prognostic factor for patients with esophageal cancer and provide evidence for diagnosis and treatment of esophageal cancer. 27 These findings suggest that the aberrant c-MYC expression could be an adverse underlying factor in carcinogenesis and progression of ESCC, and high levels of c-MYC expression were associated with the clinical development of ESCC. Apparently, our study is limited to detecting the c-MYC expression by IHC and western blot. Throughout the study, we just found that the expression of c-MYC has something to do with the clinical parameters of esophageal cancer by statistics. In this study, we did not investigate whether patient survival was correlated with the expressions of c-MYC. On account of the samples were collected from the patients who accepted radical surgery for esophageal carcinoma in our department in the recent 1.5 years, this cohort of patients are still in a timely follow-up status; the relationship between c-MYC expression and the 5-year survival rate of the patients will be statistically analyzed in the near future, which may further declare its role as a potential prognostic factor. Therefore, the relationship between the prognoses of ESCC patients with the c-MYC may be investigated by further study with a large sample size. It should be further verified by prospective analysis and more comprehensive follow-up.
In conclusion, this study indicates that the PR of c-MYC significantly increased with the malignant degree of ESCC patients. Moreover, high expression level of c-MYC has a significant correlation with poor prognosis of ESCC patients. The c-MYC could provide evidence for diagnosis and treatment of esophageal cancer.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Longyuan Youth Innovative Talent Support Project, Gansu Province Natural Science Fund (145RJZA117), Gansu Province Health Industry Research Project (GSWSKY-2015-11), and Postdoctoral Research Projects in Gansu Province (22097801).